
Abstract
Overeating is a common eating disorder and often leads to obesity and to significant physical, emotional, and social problems often warranting nursing care. Codependency has expanded beyond the chemical dependency field and describes the dysfunctional pattern of behavior of an individual in a relationship with another person or from survival in a dysfunctional family of origin. The psychological and behavioral factors surrounding overeating are noted frequently in the literature but are not emphasized in most overeating treatment programs. Anxiety, depression, anger, and compulsivity are the psychological problems often linked with overeating and codependency. The purpose of this study was to test the Codependency-Overeating Model (COM) by examining the relationship between overeating and codependency, anxiety, depression, anger, and compulsivity. The variables were measured with the Overeating Questionnaire, Codependency Assessment Tool, and Symptom Checklist-90-R. This study used a model-testing correlational design with 567 students recruited from a Mississippi community college. Pearson’s product–moment correlations noted weak correlations between age and anxiety (r = .12), age and depression (r = .20), age and compulsivity (r = .20), codependency and anxiety (r = .12), and codependency and anger (r = .16). No significant correlations were noted between overeating and codependency, anxiety, depression, anger, or compulsivity. Although the predictive relationships were not verified in the model, several important ways to minimize limitations in future studies were identified. The development and testing of the COM was the beginning step in pursuing a solid understanding of overeating and codependency and a catalyst for worthwhile future research.
Introduction
Severe overeating is a common eating disorder where the urge to eat more has spiraled out of control (National Institute of Mental Health, 2012). In the United States, lifestyles are fast paced, food is plentiful, and social situations are often centered on food. Bulik and Taylor (2005) defined overeating as eating more than the body needs to maintain health and a normal body weight, whereas Popkess-Vawter, Brandau, and Straub (1998) defined it as the taking in of excessive food without hunger until feeling physically uncomfortable. The consequence of overeating is often the serious public health problem of obesity. The cost of obesity totals US$147 billion annually and accounts for 9.7% of all medical spending (Flaskerud, 2010). The psychological and behavioral factors surrounding overeating are noted frequently in the literature; however, these are not emphasized in most prevention and treatment programs for overeating (Bulik & Taylor, 2005; Gambon & DeLuca, 2008; Linde et al., 2004; Meyer, 1997, Wyatt, Winters, & Dubbert, 2006). Considering the cost, fiscally, physically, and psychologically, more effective treatment for eating disorders should be a priority for behavioral health and mental health nurses (Roman & Reay, 2009).
Codependency was a term first used in the chemical dependency literature to describe the dysfunctional pattern of behavior of an individual in a relationship with another person who is addicted to alcohol (Cermak, 1986a). Many descriptions of codependency exist in the literature. Most agree that it is a learned behavior from surviving in a dysfunctional family of origin with resulting neglect of personal needs; focusing on another person’s needs, feelings, and behavior; and a dependency on others for emotional support and approval. Those suffering with codependency have boundary and control issues, low self-worth as well as physical, emotional, and psychological consequences. Individuals suffering with codependency are susceptible to stress-related medical problems as well as psychological problems (Cermak, 1986b; Crothers & Warren, 1996; Hughes-Hammer, Martsolf, & Zeller, 1998a, 1998b; O’Brien & Gaborit, 1992; Wegscheider-Cruse & Cruse, 1990; Whitfield, 1991). The concept of codependency has expanded past the addiction field. Codependency has been described in situations independent of chemical addiction and has been found to engender susceptibility to a myriad of health problems (Cermak, 1986a; Schaef, 1986; Wegscheider-Cruse, 1985; Whitfield, 1991). Anxiety, depression, anger, and compulsivity are the psychological problems most frequently noted in the literature associated with overeating and codependency (Cullen & Carr, 1999; Fischer, Spann, & Crawford, 1991; Gotham & Sher, 1996; Hinkin & Kahn, 1995; Hughes-Hammer et al., 1998a; Slochower, Kaplan, & Mann, 1981).
Three studies were found that suggest a connection between codependency and overeating; however, they did not specifically address overeating behavior (Allison, 2005; Meyer, 1997; Meyer & Russell, 1998). Meyer (1997) examined anorexia and bulimia, whereas Meyer and Russell (1998) examined eating disorders, particularly bulimia. Allison (2005) assessed the influence of codependency and binge eating on body mass index (BMI). There is a gap in the literature regarding the relationship between overeating, codependency, and many potential confounding variables. To begin to address this gap, the Codependency-Overeating Model (COM) was developed to provide enhanced knowledge of the connections between these phenomena. Mental health nurses and other health care providers are in a unique position to use successful interventions. The purpose of this study was to test the COM by examining the relationships between overeating and the predictor variables of codependency, anxiety, depression, anger, and compulsivity.
COM
The COM offers a framework for exploring proposed relationships between overeating and codependency. The substantial problem of overeating, the connection between codependency and disordered eating along with the scarcity of relevant empirical studies calls for more research in this area. The COM was developed to clarify the proposed relationship between codependency, overeating, and the psychological problems of anxiety depression, anger, and compulsivity.
The nursing theoretical perspective for the development and testing of the COM as a nursing research concern was provided by the Neuman Systems Model (NSM). The review of literature revealed that stressors are the origin of codependency and overeating. Neuman’s model illustrates a system in which nursing is concerned with the total person, their stressors, and the possible reactions to those stressors. According to the NSM, health problems are a concern to nursing, along with all the variables that affect a client’s response to stressors (Neuman, 1982). Guided by the NSM, a nurse can plan interventions to identify stressors, affect client responses to stressors, decrease client exposure to actual and potential environmental stressors, and assist clients to adequately cope with stressors.
The COM was developed from the Hughes-Hammer et al.’s (1998a) Model of Codependency. Hughes-Hammer et al.’s model was guided in part by the Wegscheider-Cruse and Cruse’s (1990) Codependency Model. The literature was searched for correlations between the factors proposed in the model. Review of relevant empirical studies led to the final COM (Figure 1). The Hughes-Hammer et al.’s (1998b) Model of Codependency is presented in Figure 2.

Codependency-Overeating Model
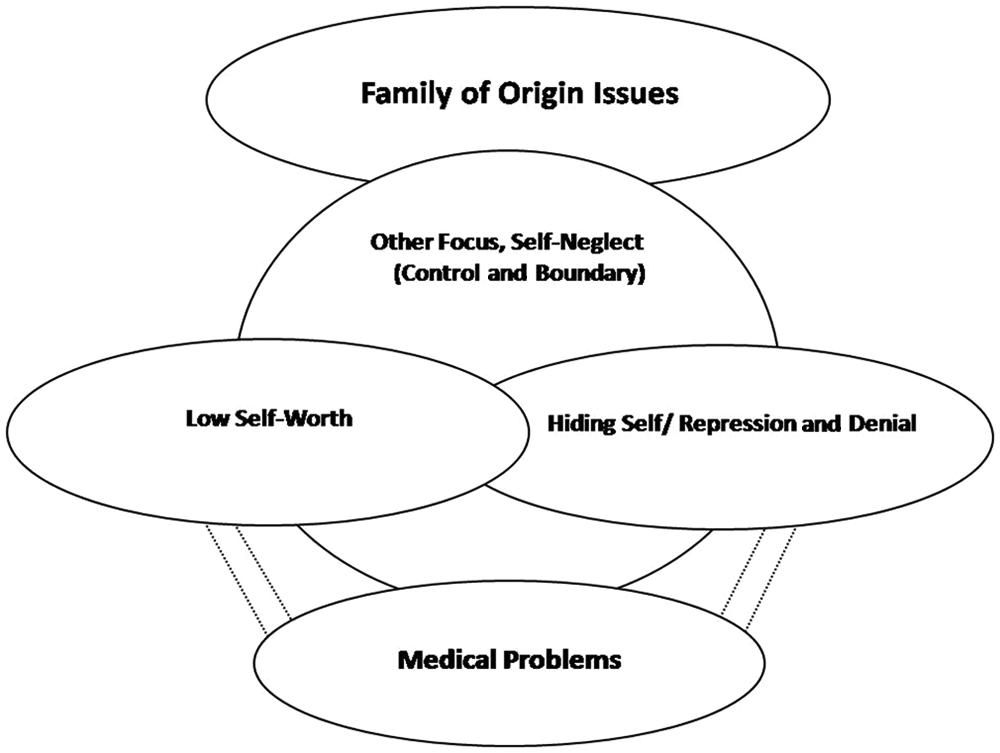
Hughes-Hammer, Martsolf, and Zeller’s (1998b) Model of Codependency
Method
Design and Research Questions
This study used a predictive model-testing correlational design to examine the overall predictive value of the COM and specifically the relationships between overeating, codependency, anxiety, depression, anger, and compulsivity and selected demographic- and health-related variables. The specific research questions addressed were as follows:
Research Question 1: Did codependency, anxiety, depression, anger, or compulsivity predict overeating?
Research Question 2: Did any single codependency symptom predict overeating? (Codependency symptoms included family of origin issues, other focus, self-worth, hiding self, and medical problems.)
Research Question 3: Did age, sex, race, personal history with drugs/alcohol, previous hospitalizations for mental health problems, or selected medical conditions predict overeating?
Research Question 4: Were the causal paths to overeating in the predictive model supported? What model of predictor variables best predicted overeating?
Sample and Setting
This study used a stratified cluster random sampling technique. The sample was stratified by campus with a random selection of class sections chosen from all introductory psychology and sociology students within each campus and among online students. Based on the number of students enrolled in each campus and the online classes for psychology and sociology, the required participation from each campus and online class was proportionally assigned and randomly chosen by computer based on the class section number. The sampling frame included 1,653 students from three campuses enrolled in psychology or sociology classes in a Mississippi (MS) community college. Students were eligible to participate if between the ages of 18 and 65 years and were not enrolled in the college’s nursing program where the researcher is a faculty member.
The students were stratified by campus, with random selection of class sections. This sampling approach produced 1,273 potential participants. However, due to student’s absences and withdrawal from classes, questionnaires were given to 810 students. A total of 602 participants returned the questionnaires (response rate = 74.3%) and 567 participants completed all four questionnaires (response rate = 70%).
Instruments
Overeating
Overeating, the variable of interest, was measured with the Overeating Questionnaire (OQ), an 80-item self-report questionnaire published by Western Psychological Services (O’Donnell & Warren, 2010). The OQ measures the key habits, thoughts, and attitudes related to obesity. The overeating score relates to the tendency to continue to eat even after hunger is satisfied. The items contributing to the overeating score included the following: “I always eat too much; I can’t say no to food at parties; If there is food left after a meal, I finish it rather than put it away; I feel I should always eat everything on my plate; I have gone on an eating binge; I hide the fact that I eat too much from other people; I stuff myself when I eat; I have trouble controlling how much I eat.” Cronbach’s alpha for the OQ ranged from .79 to .88 with .80 for the Overeating scale. Test–retest reliability ranged from .64 to .94 with the Overeating scale reported as .64. The validity of the OQ is documented in the OQ manual (O’Donnell & Warren, 2010). The overeating raw score was converted to a T-score by hand on each participant’s profile sheet. The T-score is a normalized standard score with a mean of 50 and standard deviation (SD) of 10. The score provides a comparison of an individual’s scores with the average performance of the normative group on which the scores are based. Raw- and T-scores were entered into Excel with T-scores categorized into low, average, high, and very high.
Codependency
Codependency scores were calculated from the Codependency Assessment Tool (CODAT), a 25-item 5-point Likert-type scale. The participants were asked to circle how they feel as indicated by the item on a scale from 1 = rarely or never to 5 = most of the time. To prevent response-set bias, one item is reversed-scored. Scoring for the CODAT includes a total score calculated by summing the responses on all 25 items. The possible range of scores is 25 to 125 with minimal codependency score = 25 to 50, mild codependency = 51 to 75, moderate codependency = 76 to 100, and severe codependency = 101to 125. Subscale scores can also be calculated, with a range of 5 to 25 for each scale. Subscales include Other Focus, Self-Worth, Hiding Self, Medical Problems, and Family of Origin. Reliability data for the CODAT including test–retest reliability and alpha, respectively, is as follows: Other Focus/Self-Neglect = .86/.85, Self-Worth = .90/.84, Hiding Self = .78/.80, Medical Problems = .94/.75, and Family of Origin issues = .90/.81 with total scale reliability of .90/.91 (Hughes-Hammer et al., 1998b). Detailed information regarding the development of the CODAT and the establishment of instrument validity was reported by Hughes-Hammer et al. (1998b). Demographic- and health-related information collected with the CODAT included gender, age, race, religion, marital status, number of children, employment status, level of education, past or present mental health problems, and past or present alcohol or drug problem for self, parents, spouse, or significant other (Hughes-Hammer et al., 1998b).
Anxiety, depression, anger, and compulsivity
The psychological problems of anxiety, depression, compulsivity, and anger were measured with the Symptom Checklist-90-R (SCL-90-R), a 90-item multidimensional questionnaire published by Pearson Education, Inc. (Derogatis, 1994). The answers to the paper and pencil questionnaire were entered into Q Local™, a computerized scoring and reporting system. Item verification was completed for each questionnaire. An interpretive report was generated with the raw and T-score entered into the spreadsheet. The depression score reflects a range of the manifestations of clinical depression, including symptoms of dysphoric mood and affect, feelings of hopelessness, suicidal thoughts, and other cognitive and somatic correlates of depression. The anxiety score includes the general signs and somatic correlates of anxiety. The hostility score reflects the thoughts, feelings, or actions characteristic of anger. The obsessive-compulsive score focuses on thoughts, impulses, and actions identified with obsessive-compulsive clinical syndrome and measures compulsivity. Internal consistency scores on a 1976 study ranged from .77 for psychoticism to .90 for depression with a 1988 study documenting a range of .84 for interpersonal sensitivity to .90 for depression. Test–retest reliability for a 1983 study cites a low of .78 for hostility to a high of .90 for phobic anxiety. A 1988 study documents a range of .68 for somatization to .83 for paranoid ideation and test–retest reliability for the Global Severity Index (GSI) as .84. The establishment of validity for the instrument is detailed in the manual for the SCL-90-R (Derogatis, 1994).
Data collection procedure
After approval from the community college president and the university Institutional Review Board, the psychology and sociology instructors were contacted for a convenient time during class for students to complete the questionnaires. If faculty could not give class time for completion, the researcher was allowed enough time to explain the study with a locked box placed in the faculty’s office for return of the questionnaires. All potential participants were given an oral and written description of the study with assurances about confidentiality and their right to refuse to participate. The cover letter also informed the participants that consent was implied by the completion and return of the questionnaire. The students were given the option of participating in a random drawing for three US$100 Wal-Mart gift cards as incentives to participate. The researcher was the sole data collector and the only individual with access to the questionnaires before identifying information was removed.
Data analyses
The data were entered into SPSS (Version 19). Auditing was completed with error rate <2%. Descriptive statistics were used to describe the sample. Correlations were tested using Pearson’s coefficient of correlation (Pearson’s r).
Results
Description of the Sample
Of the 567 participants completing all four questionnaires, 372 (65.7%) were women and 194 (34.3%) were men. One participant listed gender as “other” (0.2%). The participants ranged between 18 and 56 years of age (M = 22.7, SD = 6.81). The majority of students were between 18 and 21 years of age (68.7%), White (64.6%), freshmen (54.7%), single (81.7%), Christian (75.3%), and without children (64.7%). Most of the participants were Mississippi residents (95.1%) and employed (59.8%), with food service the most frequently listed occupation at 10.9% and a personal income less than US$10,000 (63.7%). The majority was underweight (11.6%) or normal weight (40.6%) with 24.5% overweight and 23.3% obese. Fifteen participants were pregnant (2.6%), and 94.5% reported not having an eating disorder. Twenty-seven participants (4.8%) stated they had previous hospitalizations for mental health problems. Seventy-three participants (12.9%) reported having a personal history of alcohol or drug abuse (past or present), 64 (11.3%) reported having a spouse or significant other with a present or past history of alcohol or drug abuse, and 140 (24.7%) reported parents with a present or past history of alcohol or drug abuse. See Table 1 and Table 2 for the demographic- and health-related characteristics of the sample.
Demographic Characteristics of the Sample

Note: Due to participants not answering all questions, several categories list frequency <567.
Health-Related Characteristics of the Sample
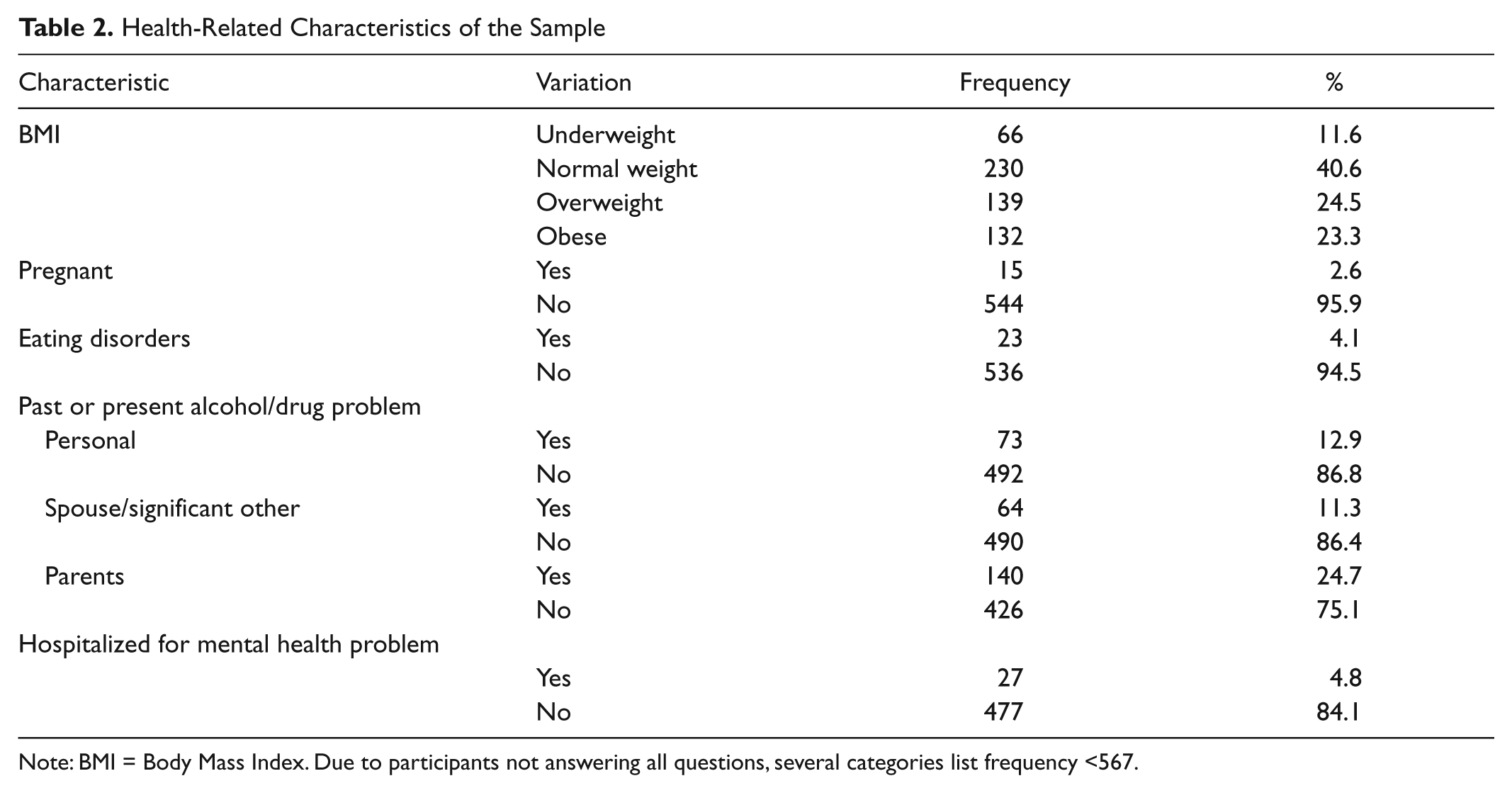
Note: BMI = Body Mass Index. Due to participants not answering all questions, several categories list frequency <567.
Description of Overeating
Overeating T-scores ranged from 2 to 78 (M = 48.84, SD = 10.42). Overeating was reported by 14.3% of the participants with 85.6% reporting scores indicating they were not overeaters. Of the participants scoring in the overeating category, 65 (11.5%) scored “high” and 16 participants (2.8%) scored “very high.” The majority of participants (83.6%) scored <60T on the Defensiveness (DEF) scale, which indicates accuracy in responses. Likewise, the majority of Inconsistent Responding (INC) scores (90.3%) were ≤4, indicating that the responses were an accurate description of self. Significant differences were noted when overeating was cross-tabulated with age. A greater incidence of high overeater scores was reported by the 22+ group (16.4%) compared with the 20 to 21 (11.2%) and the 18 to 19 age group (7.6%). The very high overeater scores were reported by 4.5% of the 20 to 21 age group, compared with 1.9% by the 18 to 19 age group and 2.3% by the 22+ age group.
Description of Codependency
Codependency scores ranged from 25 to 121 (M = 47.87, SD = 15.75). Only four participants (0.7%) scored in the severe codependency category; therefore, the moderate and severe categories were combined. Significant differences were noted when codependency was cross-tabulated with race, academic standing, hospitalization for mental health problem, and past or present alcohol/drug problem (personal, spouse/significant other, and parents). Mild codependency was reported by 32.1% of the White participants compared with 21.3% of the Black participants, while 7.4% of Whites reported moderate/severe levels of codependency compared with 3.8% of the Black participants. The sophomore students also reported a higher incidence of mild codependency (32.7%) compared with the freshman students (26.1%) with 10.4% of the sophomores reporting moderate/severe levels compared with 2.3% freshman. In the participants reporting a previous hospitalization for mental health problems, 33.3% reported mild codependency compared with 29.4% by the group that had never been hospitalized. The group with previous hospitalizations reported 22.2% moderate/severe codependency levels compared with 5.3% by the group that had never been hospitalized. The participants with a past or present alcohol/drug problem for self, spouse/significant other, or parents reported a greater incidence of mild and moderate/severe levels of codependency compared with the group with no past or present problem with substance abuse. Thirty-five percent of those with a personal drug/alcohol problem reported mild codependency compared with 28.1% of those with no problem, whereas 19.2% with a personal drug/alcohol problem reported moderate/severe codependency compared with 4.3% of those with no problem. Thirty-four percent of those with a spouse or significant other drug/alcohol problem reported mild codependency compared with 28.2% of those with no problem, whereas 15.6% with a spouse/significant other drug/alcohol problem reported moderate/severe codependency compared with 5.1% of those with no problem. Forty percent of those with a parental drug/alcohol problem reported mild codependency compared with 25.4% of those with no problem, whereas 12.1% with a parental drug/alcohol problem reported moderate/severe codependency compared with 4.3% of those with no problem.
Description of Anxiety, Depression, Anger, and Compulsivity
Anxiety scores ranged from 37 to 81 (M = 57.04, SD = 12.70). There were 201 (35.4%) participants with anxiety T-scores ≥ 63. Depression scores ranged from 34 to 81 (M = 60.02, SD = 10.87). There were 235 (41.4%) participants with depression T-scores ≥ 63. Anger (noted as hostility on the SCL-90-R) scores ranged from 40 to 81 (M = 58.97, SD = 11.68). There were 215 (37.9%) participants with anger T-scores ≥ 63. Compulsivity (noted as obsessive-compulsive on the SCL-90-R) scores ranged from 37 to 80 (M = 62.12, SD = 10.74). There were 299 (52.7%) participants with compulsivity T-scores ≥ 63.
Relationship Between Variables
When selected demographic characteristics of the sample were correlated with the variables of anxiety, depression, compulsivity, and anger, a weak correlation was found between age and anxiety (r = .12), depression (r = .20), and compulsivity (r =.20); otherwise, no significant correlations were found. A weak correlation was found between codependency and anxiety (r = .12) and between codependency and anger (r = .16).
Testing of the COM
Related to Research Question 1, there were no significant correlations between overeating and any of the variables; therefore, codependency, anxiety, depression, anger, or compulsivity did not predict overeating. Related to Research Question 2, no significant correlations were noted when codependency symptoms were correlated with overeating. Related to Research Question 3, no significant correlations were found when personal history with drugs/alcohol, previous hospitalizations for mental health problems, or medical conditions were correlated with overeating; therefore, these demographic- and health-related characteristics did not predict overeating. Related to Research Question 4, no significant correlations were found between codependency, anxiety, depression, anger, compulsivity, and overeating; therefore, the causal paths to overeating in the predictive model were not supported.
Discussion
The literature on overeating and codependency has summoned further clarification. In the 2001 article “Is Codependency a Meaningful Concept,” Stafford (2001) called for more research aimed at further validation of the codependency construct. Codependency continues to be criticized in the literature as a weak theory lacking an effective operational definition. Although it has been asserted that no single theory adequately accounts for the development or treatment of overeating as an eating disorder, it is considered a serious disorder and effective treatment should be one of the top priorities for behavioral health (Roman & Reay, 2009). The current study was undertaken to examine the relationship between overeating and codependency to address concerns about both of these issues. Although the results of this current study did not substantiate the predicted relationships in the COM, several worthwhile findings were revealed that contribute to the literature regarding codependency and overeating.
The majority of participants in this study reported minimal codependency, which supports the findings in the literature that codependency is not a widespread problem in the general population (Martsolf, 2002; Martsolf, Hughes-Hammer, Estok, & Zeller, 1999; Martsolf, Sedlak, & Doheny, 2000). In the current study of students enrolled in a community college in the mid-south, codependency scores were higher in the White participants, those with mental health hospitalization histories, and with previous or past alcohol or drug problems for self, significant others, or parents. These discoveries about the prevalence of code-pendency are congruent with findings from other studies (Gotham & Sher, 1996; Hughes-Hammer et al., 1998a). Data analysis in this study found a weak correlation between codependency and anxiety, and between codependency and anger, which is consistent with the findings in past literature (Cullen & Carr, 1999; Fischer et al., 1991; Gotham & Sher, 1996; Hinkin & Kahn, 1995). No significant correlation was found between codependency and depression, or between codependency and compulsivity in this study, a finding that is inconsistent with other studies in the literature (Cullen & Carr, 1999; Gotham & Sher, 1996, Hinkin & Kahn, 1995; Hughes-Hammer et al., 1998a). Reasons for the incongruence in findings could include use of different instrumentation for data collection and dissimilar demographic- and health-related variables. The sample in this study consisted of healthy nonpatients, the majority of whom were young, White, and single.
Although the COM was grounded in the literature, this study found no statistically significant relationship between overeating and anxiety, depression, compulsivity, or anger. This finding is contrary to the literature that anxiety, depression, anger, and compulsivity contributed to eating (Arnow, Kenardy, & Agras, 1992; Ruderman, 1983; Slochower et al., 1981; Stickney, Miltenberger, & Wolff, 1999). The association between codependency and eating issues was noted in the literature; however, overeating was measured with instruments other than the OQ, which was used in the current study. The studies in the literature also differed from the current study in sample size, ethnicity, mean age, relationship, and/or weight status. Interestingly, 47.8% of the participants self-reported they were overweight or obese, but only 14.3% reported themselves to be overeaters with their answers to the OQ. Although the INC and DEF scores on the OQ indicated the participants answered based on item content with low response bias, the validity of the instrument to measure overeating is called into question.
A careful research design, sampling plan, and strong recruitment strategy were used in this study to control the extraneous variables and secure a representative sample; however, several limitations were noted. These limitations include response bias in the self-reported data, testing fatigue with the use of four instruments, and instrument format and clarity. The instruments used in this study utilized different methods of answering the questions, including circling, bubbling, filling in blanks, and check marks. Some forms had perforations, flaps, as well as front-and-back answers, making the process somewhat more difficult for some students. The study findings are generalizable only to the students at this MS college.
Recommendations for Future Research
Qualitative inquiries are necessary to describe, explore, and explain the phenomena of overeating. Additional studies are also needed to develop stronger instruments to measure overeating. This study could be replicated with more diverse participants who are more likely to have mild or moderate/severe codependency levels. As has been noted, although the prevalence of codependency in the general population is relatively low, it does create significant life disruptions for those who are touched by its presence (Whitfield, 1991). Therefore, any research designed to examine codependency in relation to other variables needs to draw on a target population likely to be susceptible to codependency. In addition, recruiting participants from addiction treatment centers, eating disorder (overeating) clinics, or psychology practices that treat codependency or eating disorders could enhance the sample characteristics.
Summary
A model of overeating has been carefully constructed to portray literature-based propositions about the complex interrelations between overeating and codependency, mediated and moderated by selected demographic- and psychological characteristics. This article describes the initial attempt to explore these complex interrelations in a single study. Although the relationships in the model were not statistically significant and the predictive relationships were not verified, the COM can provide a base for nursing research to guide future studies with different samples, utilizing different instruments, designs, and methodology. This was a beginning step in gaining understanding of overeating and codependency and serves as a catalyst for future nursing research in this area.
Footnotes
Acknowledgements
The researcher wishes to express appreciation to Dr. Deborah Konkle-Parker and Dr. Lei Zhang, associate professors at the University of Mississippi Medical Center, for their valuable comments and assistance as members of the dissertation committee. The researcher also thanks Dr. Kim Hoover, Dean, University of Mississippi Medical Center, School of Nursing, for her contribution to the data analysis and Dianne Scott, MSN, RN, for her assistance in data scoring. In addition, the researcher expresses appreciation to the community college administration, faculty, and students for their assistance and participation in data collection.
Authors’ Note
This article is based on the research conducted for the first author’s doctoral dissertation, which was completed in March, 2012, at the University of Mississippi Medical Center in Jackson, Mississippi.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Funding for the research was provided by grants from Sigma Theta Tau International and the University of Mississippi Medical Center.