
Abstract
This article identifies cultural models of osteoporosis, as shared by community-dwelling older women in southeastern Australia, and compares these with cultural knowledge conveyed through social marketing. Cultural models are mental constructs about specific domains in everyday life, such as health and illness, which are shared within a community. We applied domain analyses to data obtained from in-depth interviews and stakeholder-identified print materials. The response domains identified from our case studies made up the shared cultural model “Osteoporosis has low salience,” particularly when ranked against other threats to health. The cultural knowledge reflected in the print materials supported a cultural model of low salience. Cultural cues embedded in social marketing messages on osteoporosis may be internalized and motivating in unintended ways. Identifying and understanding cultural models of osteoporosis within a community may provide valuable insights to inform the development of targeted health messages.
According to the National Health Survey, one in two women and one in three men in Australia above 60 years are likely to experience an osteoporotic fracture (Australian Bureau of Statistics [ABS], 2009). Sustaining an initial vertebral fracture is said to increase the risk of subsequent fracture (Briggs, Greig, & Wark, 2003; Sontag & Krege, 2010), and each fracture event sustained is thought to be associated with excess morbidity and mortality (Pasco et al., 2005). Osteoporosis is estimated to cost the Australian taxpayer some AU$7 billion a year (The Royal Australian College of General Practitioners, 2010). Most people who have osteoporosis do not know it (Taylor, Gill, Phillips, & Leach, 2003), which represents a lost opportunity for timely help-seeking and behavioral change to mitigate risk of fracture and its sequelae. Furthermore, the large numbers of people classified as being at “modest risk” in fact sustain more than half of all fractures occurring in the community (Pasco et al., 2006)—that is, outside of hospital or community care settings—suggesting that public health measures that motivate behavioral change may be more effective in preventing fracture than attempting to provide medical therapy to such a high proportion of the overall population.
However, the statistics indicate that these measures are not universally effective. For example, a large Australian population survey reported that men and women across all age groups not only underestimated the risk of getting osteoporosis in the future but also had little knowledge of the disease and its risk factors (Taylor et al., 2003). This study of 3,001 randomly selected adults found that the overall perceived risk of getting osteoporosis was low (59.7%) or moderate (40.6%). This knowledge gap occurs elsewhere; worldwide, osteoporosis remains largely undiagnosed (Taylor et al., 2003) and underinvestigated (Cheng & Green, 2008; Otmar et al., 2011). Furthermore, it has been widely reported in Australia and internationally that prescription rates for osteoporosis treatments, as well as adherence to treatment, are suboptimal (Cadarette, Gignac, Jaglal, Beaton, & Hawker, 2009; Gold & Silverman, 2006; Kaufmann et al., 2005; Lekkerkerker et al., 2007; Rossini et al., 2006). For example, a 2007 systematic review found a wide variation (17.9%-78.0%) in patient persistence with bisphosphonate treatment at 12 months (Cramer, Gold, Silverman, & Lewiecki, 2007).
Understanding how consumers in specific sociocultural settings view a given health problem is essential in developing effective, targeted social marketing messages to influence positive health behaviors and health-seeking (Mostow et al., 2010). In this article, we compare cultural models of osteoporosis shared among older women in the study region with those embedded in social marketing messages on osteoporosis.
Materials and Method
Note that we use the term “consumer” in reference to adult members of the general community, regardless of whether they are consumers of health services, after Buckley and Ó Tuama’s call for an expansion of “the notion of the health service user to include those who may not be directly using the health service, but who are consuming health messages” (Buckley & Ó Tuama, 2010, p. 593). It would not have been appropriate to refer to participants in the community case study as “patients” or “clients”; all participants in the study could be considered consumers of health messages, a central topic in this article.
Social marketing approaches typically rely on theories of consumer behavior such as the health belief model, theory of reasoned action/planned behavior, and social cognitive theory; however, there is little consensus on which models are most appropriate for particular populations and problems (Lefebvre, 2000), and little is understood about how consumers’ experiences of a particular disease or condition can be utilized to complement these theoretical models and thus enhance social marketing approaches (Barg & Grier, 2008). A cultural models approach provides an inductive method by which to understand consumer responses to health communications in the domain of interest (Barg & Grier, 2008). Underpinning the cultural models approach are two related theories about the nature of knowledge and meaning: (a) that as human beings, we each uniquely attribute meaning to phenomena, as well as to our own existence within the world (social constructivism), and (b) that the world holds no meaning prior to our experience of it (social constructionism; Crotty, 1998; Patton, 2002). In this context, we sought to explore participants’ perspectives as individuals and as actors within their society/community, since the two roles are separate, yet deeply connected.
Hawkins, Kreuter, Resnicow, Fishbein, and Dijkstra (2008) described three distinct categories on a continuum of techniques used in health communications: mass communication, targeting, and tailoring. At the one end, mass communication broadcasts identical messages to “relatively large, undifferentiated audiences” (Kreuter et al., 2008, p. 455) and may be considered less than ideal in communicating about a condition such as osteoporosis, since the message may not be relevant to large segments of the broadcast audience, and those segments of the audience for whom it may be relevant could assume that the messages are intended for others, or at least not for them. At the other end of the continuum, tailoring customizes messages “matched to the needs and preferences of individuals” (Kretuer et al., 2008, p. 455). Given evidence that tailored health messages are better read and recalled than nontailored messages (Kreuter, Oswald, Bull, & Clark, 2000), it would appear to be an ideal technique for communicating with people who need to be provided with relevant information about osteoporosis, but is understandably expensive in terms of cost and effort required to gather and maintain data from and about the intended audience (Hawkins et al., 2008). Targeting presents a middle-ground technique for communicating with large audiences about issues relevant to them, using the technique of “segmentation,” whereby a proportion of the population, such as a demographic category, receives a shared message (Hawkins et al., 2008). In this article, it is assumed that identification and understanding of the dominant cultural models shared among the target audience of women aged 75 years and older will provide insights into the appropriate segmentation of health messages to them, and that identifying the cultural knowledge underpinning the print materials will help to indicate whether their messages were appropriate for this market segment.
Cultural models are mental constructs about specific domains in everyday life, such as health and illness, which are shared within a community, and which may assist efforts to interpret human behavior (Barg & Grier, 2008). While individuals, families, and organizations have their own models for how the world works, based on their respective experiences and influences, the models that are shared within a community become the cultural models of that society (Dressler, 2004). Consensus theory states that a cultural domain exists when there is a moderately high level of consensus within the community in question (Furlow, 2003). In the case of osteoporosis, the cultural domain “osteoporosis” is confirmed by consensus within the medical fraternity, which also provides a consensus definition for the profession. However, this is not to say that the same cultural model exists—if indeed it does exist—at the community (i.e., lay person’s) level or among other groups in society. It is possible that, for example, policy makers, economists, medical practitioners, and ordinary members of society have different cultural models of the same phenomenon. Furthermore, a high level of consensus does not mean that cultural beliefs about a phenomenon are homogeneous or that they are shared among all members of the community. In this article, we aim to identify the dominant cultural models that may assist in health communications in a particular setting. In so doing, we draw on aspects of cultural consensus theory. We do not apply the theoretical model for quantitative analysis, but to support the notion that consensus underlies cultural models.
Cultural models may be uncovered through a variety of research strategies. For example, cognitive anthropologists examine data on how people talk and behave to uncover cultural models that explain how they function within their respective societies (Quinn & Holland, 1987). In the United States, Barg and Grier (2008) used qualitative interviews to identify a cultural model of breast cancer shared by African American women, which suggested that they did not perceive the disease as particularly relevant to them, despite prevailing messages in the media. Thus, cultural models can help to explain both the superficial and deeper meanings attributed to phenomena within a community. A superficial meaning of osteoporosis could be the fact that it is a condition affecting the bones; a deeper meaning might be inferred from the common adage that osteoporosis is a “silent disease.” Identifying and understanding the dominant cultural models shared within a community can therefore be used to inform the development of appropriately targeted social marketing messages and campaigns. The findings from the Barg and Grier study demonstrated how salient social marketing messages might be developed to effectively reach its particular target audience.
In this article, we aim to explore dominant cultural models of osteoporosis shared by members of the Geelong community, and to compare that with the cultural knowledge implicit in relevant social marketing materials on osteoporosis, including popular print media such as women’s magazines. Using this construct, we offer a novel approach to understanding consumer perspectives and responses to health communications on osteoporosis. To the best of our knowledge, to date no Australian studies have been conducted to explore cultural models of osteoporosis, and we are unaware of any studies examining cultural knowledge of osteoporosis as represented in social marketing.
Setting
The study was undertaken in the regional city of Geelong in southeastern Australia. Geelong has a moderately large, stable population (160,991 at the 2006 Census; ABS, 2007) and is located within the national statistical boundary known as the Barwon Statistical Division (BSD). At the 2006 Census, the total population of the BSD was 197,477 and its characteristics included 51.3% females, 78.9% Australian born, 0.7% Indigenous Australian, 14.2% aged 65 to 84 years, and 2.1% aged 85 years and older. More than 70% of residents owned or were purchasing their own home, and 93.7% of the labor force was employed at the time of the 2006 Census. In these and other respects, the region’s social, cultural, and geographical demographics closely resemble national socioeconomic indicators, making it an ideal setting for epidemiological and other research (Pasco, Henry, Gawdry, Nicholson, & Kotowicz, 1999).
Participants
Eight participants were assigned to one of two case studies presented in this analysis, which was nested within a larger qualitative study (n = 65) of challenges and enablers in the prevention and treatment of osteoporosis in women and men aged 55 years and older. Recruitment was achieved by soliciting volunteers through community notices, articles in local media, flyers, and word of mouth.
Cultural models present somewhat of an enigma; it is acknowledged in the literature that it would be near impossible to uncover all the cultural models about a topic held within a given community, not only because of the sheer number and the likely complexity of links and overlaps of potential cultural models, but also because these models are dynamic and dynamically held and shared (Holland & Quinn, 1987). Therefore, it is difficult to be sure about the number of cultural models that could be said to represent a population, or to prescribe the number of people who ought to share a cultural model for it to be considered dominant within that community segment. For these reasons, we opted for the well-known qualitative method of saturation. In-depth interviews with women aged 75 years and older were conducted sequentially, until saturation of the predetermined topics (Liamputtong, 2009). A total of eight women were interviewed. Although it was possible to interview more women, it was felt that this would not enrich the study, given that its purpose was exploratory and to conduct in-depth and detailed analysis, with a focus on models in language, which is a methodological learning reported by other qualitative studies on osteoporosis (see, for example, Lettenmaier et al., 1994; Skolbekken, Østerlie, & Forsmo, 2008).
Ethics Statement
The study was conducted in accordance with the World Medical Association (2008) Declaration of Helsinki and approved by the Barwon Health Human Research Ethics Committee. All participants read and signed a participant information and consent form prior to being interviewed. All participant names used in this article are pseudonyms.
Data Gathering
Semistructured, in-depth interviews were conducted by the first author (R.O.) at our research facility on the Geelong Hospital campus in central Geelong. A loose set of predetermined topics was used to invite participants in both groups to describe their understanding of the condition of osteoporosis (what it is, what causes it, whether it is treatable and/or preventable) and what they may have heard others say about osteoporosis. Fracture case study participants were also asked about the circumstances of their fracture(s); any immediate and subsequent treatment received, including investigation for osteoporosis; their reaction to the fracture and, if relevant, their reaction to receiving a diagnosis of osteoporosis. Probing and follow-up questioning were used to encourage reflection and detailed responses. At the conclusion of the interviews, which lasted at least 90 min, participants were prompted to comment on anything related to osteoporosis and/or fracture that had not already been covered in the discussion.
Key stakeholders were consulted to provide copies of, or references to, print materials to which participants in our study, including the case studies, were likely to have been exposed in the past 5 years. Stakeholders included local and state government health departments, Barwon Health (the major health services provider in the region), local medical practitioners, pharmacies, researchers in osteoporosis, and consumers. We also searched local media and a popular (national) women’s magazine for articles on osteoporosis. The materials identified for inclusion in the analysis included fact sheets, online (printable) patient information sheets, pamphlets, booklets, and magazine articles. We selected materials on the basis of relevance (provides information about osteoporosis) and circulation (confidence that study participants were exposed to, or were likely to have had access to, one or more of the print materials over the past 5 years). The appendix provides a complete list of the 10 items included in the study.
Data Analysis
Theories of the organization of cultural knowledge provided a framework for our analyses of the verbal data and the print artifacts examined for the present study. Cognitive anthropological approaches suggest that cultural models (which we identify from what people say, or do not say) are related to behavior “in complex, powerful ways . . . Cultural models frame experience, supplying interpretations of that experience and inferences about it, and goals for action” (Quinn & Holland, 1987, p. 4). In the present context, when we identify participants’ cultural models of osteoporosis and compare these with the cultural knowledge implicit in the social marketing messages about osteoporosis to which they may have been exposed, we can reasonably link these with their behaviors in relation to osteoporosis and its management. For example, in a community in which cultural models of osteoporosis revolve around the notion of osteoporosis being a result of a deficit of calcium, and social marketing messages encourage an increase in calcium intake, some people may be motivated to change their diet while others may take a calcium supplement, and yet others may do nothing. Neither the cultural model nor the social marketing messages can be said to cause such behavioral change (or no change), but each plays a role in influencing the person’s decision making. Since we cannot be sure about the strength of influence, it is important to ensure that social marketing messages are as closely aligned as possible with cultural models held by the intended audience.
For the purposes of our analysis, we assigned the data collected from the eight participants so they formed two collective and intrinsic case studies (Silverman & Marvasti, 2008). The collective case study method involves selecting a few cases to illustrate and analyze the topic of interest as a single case, while the intrinsic case study method involves selection of cases specifically for their relevance to the study question. Together, these methods provide a powerful means for intensive investigation. Thus, the four participants selected to the “fracture case study” were those who had sustained one or more fractures in the previous 5 years, and the four in the “community case study” were consumer volunteers from the local community.
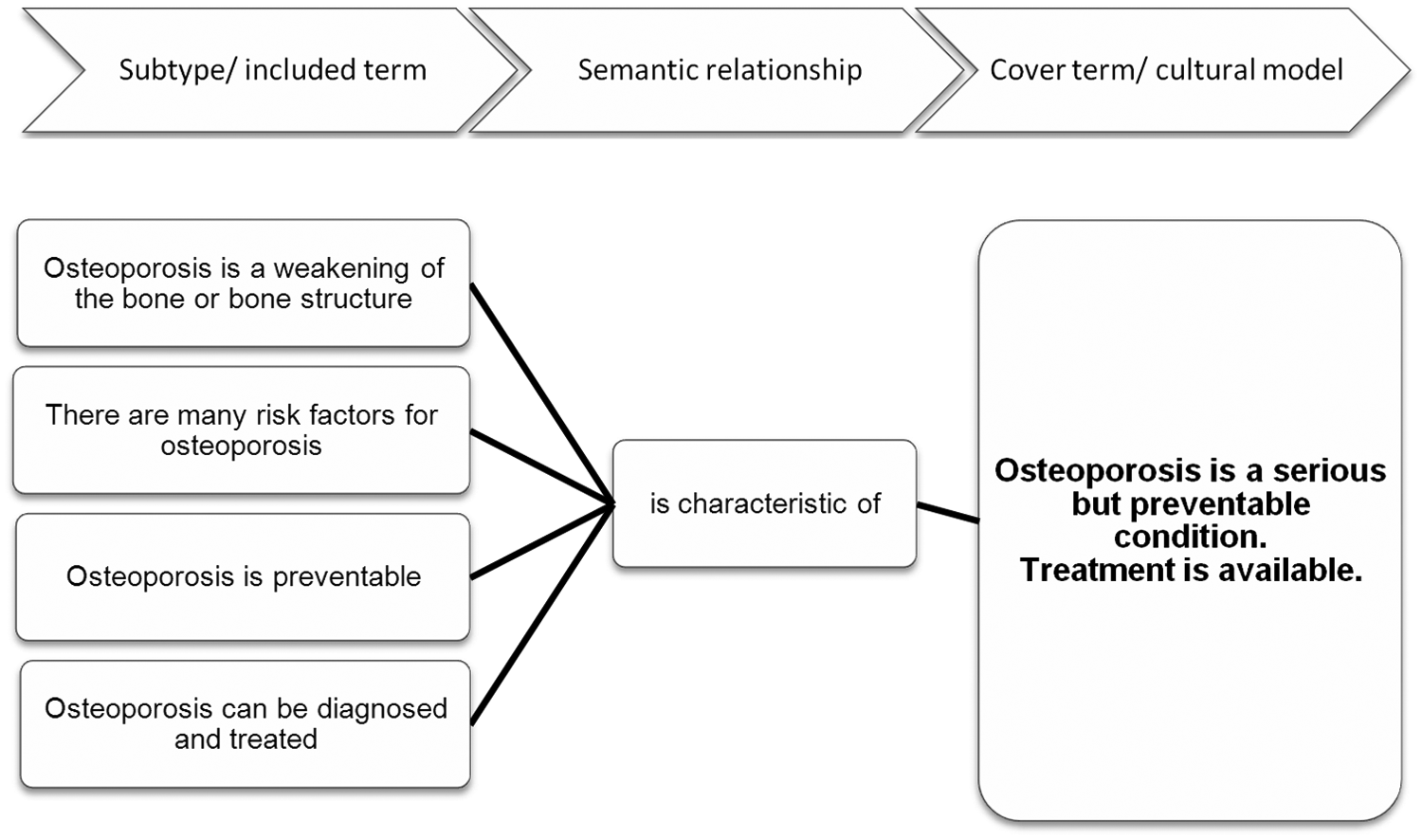
The interviews were audiorecorded, transcribed, and sent to participants for verification. Once finalized, the transcripts were imported into NVivo 9 (QSR International, 2010) for coding, using the constant comparative method described by Boeije (2002). Peer review (by coauthors M.M., J.A.P., M.A.K.) of coding schemes and conclusions was used to check validity and dependability (Liamputtong, 2009). Once coded, the data were analyzed using Spradley’s system of domain analysis, which specifies three types of domain: folk, mixed, and analytic (Spradley, 1979a, 1979b). A domain is defined as “an organizing idea or concept” that forms the basic unit in a cultural setting (Neuman, 2003). From the folk domains (terms used by participants) in the data, we identified a series of mixed domains: labels given or added by the researcher to folk domains. Then, from these mixed domains, we inferred meaningful categories and identified patterns in the data, to which we assigned analytic domains, or terms that encapsulated the cultural models shared by participants. Figures 1 to 4 demonstrate the process: Statements in the left-hand columns (“subtype/included term”) represent the mixed domains that emerged as category labels from combinations of researcher paraphrasing of chunks of data and the coding of participants’ statements in response to a question such as, “What is osteoporosis?” Several further combinations of category statements were tested to create the cover term (the cultural model in the right-hand column) as the overarching statement, and the center columns suggest its semantic relationships with the mixed-domain categories. This approach is both innovative and sensitive, in that it requires close attention to be paid to language—of both participants and researchers—and the relationships between specific terms used to identify cultural meaning (Neuman, 2003).

Cultural Model 1—domain analysis worksheet
Message 1—domain analysis worksheet

Message 2—domain analysis worksheet
Message 3—domain analysis worksheet
The process described above for domain analysis of the interview data was also used to identify cultural knowledge implicit in the social marketing materials identified for examination in the study, and this analysis included assessment of each publication for its clarity, accuracy, and general tone (e.g., whether the tone was informative, reassuring, matter-of-fact, or invoked fear or anxiety).
Results
In-Depth Interviews
The four women in our fracture case study each reported having received a diagnosis of osteoporosis and experiencing multiple fractures during her adult life. Fracture sites included wrist, hip, spine, ribs, scapula, pelvis, and foot. Two of the women were taking prescribed osteoporosis treatment, one was taking (self-prescribed) calcium and vitamin D supplements, and the fourth was not taking any medication or supplements related to fracture or osteoporosis. While all four were currently living in their own homes, two resided within a retirement village. Two women were widowed, the third was married, and the fourth had never married. Only one of the interviewees was born in Australia, and she had lived in the region all her life; the others were born in the United Kingdom, and each had resided in the region for at least 20 years.
Data from interviews with the remaining four women were analyzed as a comparison case study (the “community case study”), acting as a form of verification of the fracture case study. Three of the women in the community case study reported having received a diagnosis of osteoporosis; two were currently on bisphosphonate treatment as well as calcium supplementation, while the third had been taken off her bisphosphonate treatment 2 to 3 years prior to interview, after having taken it for 10 years. This treatment cessation was reportedly a precautionary measure on the part of her doctor, who she said was concerned “because we don’t know the long-term problems.” Although all four women reported having fallen in the previous 12 months, none had experienced a fracture in the previous 15 to 20 years, if ever. The women were all living independently; three of these within a retirement village setting. Three women were widowed, while the fourth was married. Two were born in Australia and had lived in the region all their lives; the other two were born in the United Kingdom and Indonesia and had resided in the region for 14 years and 51 years, respectively.
Identifying the Shared Cultural Model
In analyzing the data from the fracture case study, seven subtypes (or parts of the domain) emerged in the course of identifying the mixed and analytic domains within the shared cultural model, “Osteoporosis has low salience”: (a) osteoporosis is not a serious disease, (b) osteoporosis has low impact, (c) osteoporosis has many possible explanations or causes, (d) osteoporosis happens to other people, (e) a healthy/balanced lifestyle prevents osteoporosis, (f) a diagnosis of osteoporosis does not necessarily motivate behavioral change, and (g) the “silent” disease made visible.
Cultural Model 1: Osteoporosis Has Low Salience
Osteoporosis is not a serious disease
Osteoporosis was not considered to be a “serious disease” in and of itself, particularly when compared with other chronic conditions. For our participants, among the many threats to health, osteoporosis did not rise to nearly the same level of salience and concern as heart disease, stroke, cancer, and even arthritis. For example, according to Petra,
1
I’ve always thought, of all the things I’ve got—there’s a few things—osteoporosis is the [pause] least of my problems . . . I’ve got arthritis. Now, if I had a choice of getting rid of that or osteoporosis, I would say the arthritis, because that hurts all the time.
Only one participant, Beulah, considered osteoporosis to be a serious disease, second only to stroke as a threat to health, due to the risk of fracture and consequential limitations to mobility:
I felt I was coping with all the other problems that I had, and this one [osteoporosis] is the one that has been most limiting. So I’d put it fairly high on the scale of “not good.”
Osteoporosis has low impact
Participants were not unduly concerned about having osteoporosis, even after receiving a diagnosis. This was related to the first subtype (“osteoporosis is not a serious disease”), both of which are consistent with the literature on Australians’ (lack of) concern about osteoporosis, relative to other chronic conditions (Miller & Tuffin, 2009). It also highlighted the general attitude toward aging at this stage in participants’ lives:
I see it just as part of getting older. Because you can’t get older without problems. (Katrin) No, I don’t think I am really concerned. I guess because I’m getting to the latter end of my life, that maybe I just think, make the most of it while I can. (Yvette)
Osteoporosis has many possible explanations or causes
I understand that it’s a—more or less a disease of the bone, where the bones get very porous and brittle, and so they can break very easily . . . it’s not necessarily connected to old age, I know. But it seems to get worse as we get older. (Yvette) [W]hen I was sick with my ulcerative colitis and had to have steroids, I started taking calcium then, because I knew that [osteoporosis] was always a possibility. (Beulah)
Participants held contradictory beliefs about the cause(s) of osteoporosis. On one hand, there was a perception that they themselves could exercise considerable control over getting osteoporosis, while on the other hand, genetic factors were viewed as paramount.
[Y]ou know, for years I didn’t drink milk, or eat cheese or butter, so I think mine is quite self-inflicted. (Charmaine) I guess it’s something to do with the genes and makeup of the individual person. (Yvette)
Osteoporosis happens to other people
Although they expressed the view that osteoporosis was not alarming, participants were surprised and initially did not believe their diagnoses. It was something they had witnessed or heard of in others but never expected they would have to confront. One participant said that even though she had sustained several fractures prior to sustaining her spinal fracture, this singular event compelled her to accept the diagnosis of osteoporosis.
And [the medical specialist] took one look at me, and he said, “You’ve fractured your spine.” And I said, “No, I haven’t.” He said, “You have!” A complete shock . . . A complete shock, because at that time I was going to do aerobics at the gym, four times a week. I was walking from North Geelong into town, all the time. It was a tremendous shock, and I wouldn’t believe it. I just said, “It can’t be!” (Charmaine)
A balanced lifestyle prevents osteoporosis
Participants believed that a healthy person who lived a balanced lifestyle would not get osteoporosis. This was described as having a “good” diet and regular exercise, and together these were thought to be protective.
A diagnosis does not necessarily motivate behavioral change
Once a diagnosis of osteoporosis had been made, participants did not feel compelled to make significant changes to their lifestyles.
My husband said, “You have to be more careful and not fall.” But falling is . . . an accident. You can try [to be more careful] but it becomes very paranoid, so I don’t. No, I didn’t change anything. No, nothing. (Katrin)
One woman moved very quickly from her initial reaction of shock and disbelief to what might be described as denial or complacency: “I think once the initial, you know, shock that you’ve got it is over, then I put it to the back of the mind.” (Yvette)
The “silent” disease made visible
This subtype emerged in analyzing both what was said as well as what was not, or what Neuman refers to as “negative evidence” (Neuman, 2003).
Osteoporosis, you don’t feel it, until you fall and break something. (Petra)
The interview technique of “active listening” allowed the researcher “to listen to what was said and how it [was] said” (Liamputtong, 2009, p. 50), and then to follow up with prompts where appropriate. Field notes provided data on silences, indicating uncertainty or establishing unspoken boundaries to the interview. Participants’ own expressed views of osteoporosis differed from those they ascribed to the community. For example, in response to the question of whether a stigma existed in the community in relation to osteoporosis, all participants firmly denied this was the case. Their silences suggested, “I am not one to perpetuate stigma,” and yet they all mentioned the “dowager’s hump” (kyphosis) with not a small measure of concern, at times even dread.
I always thought from the time I was diagnosed, I’m not going to [get a dowager’s hump], I’m going to stand up straight . . . But I’ve had it for all those years, and I don’t really have a dowager’s hump. (Petra)
Here, while Petra has rejected the notion of community stigma, she also expressed a relief at being spared this affliction, suggesting otherwise.
Each of the seven subtypes (or included terms) described above has a defined semantic relationship with the cultural model “low salience” (Figure 1). In this analysis, each of the first six subtypes has the semantic relationship “is a reason for” the cultural model of low salience, while the seventh subtype has the semantic relationship “is a result of” the cultural model of low salience.
Analysis of the data from the community case study confirmed the cultural model, “Osteoporosis has low salience,” identified from the fracture case study. We also identified an additional subtype unique to the community case study.
Osteoporosis comes with aging and thinning of the bones
Apart from one participant, who reported that she had no experience or knowledge of osteoporosis, there was an acceptance of osteoporosis as a normal and natural consequence of aging.
Well, I think as you get older, you know . . . it’s the thinning of the bones; that’s how I think of it, or some people refer to it as “bone softening.” (Anna) But most people—a few people that I know have got osteoporosis and have had falls and have had fractures. But I just, personally, I see it just as part of getting older. Because you can’t get older without problems. (Katrin)
Print Materials
The cultural knowledge underpinning the messages in the print materials were categorized into three distinct messages; using the same process as for the cultural models, we identified several subtypes describing each message.
Message 1: Osteoporosis Is a Serious But Preventable Condition. Treatment Is Available
Within this message, osteoporosis was identified as a serious but preventable condition for which effective tests and medications were available. While the texts were not explicit in their use of the term serious, and none described osteoporosis as a “disease,” the seriousness of the condition was conveyed through the tone and presentation of content about osteoporosis, and by the organizational branding associated with health care. The print materials produced by Barwon Health, Better Health Channel, Osteoporosis Australia, and the pharmaceutical company Merck Sharp & Dohme presented messages that fitted within this cultural conception. The pamphlet by Osteoporosis Australia was designed and targeted specifically for men. However, it was included in the study since it had been identified by a stakeholder as a “good” resource on osteoporosis to which participants in the study may have been exposed in the previous 5 years. While the pamphlet included facts and information about risk factors for osteoporosis in men, it also included clear information about osteoporosis in general and the importance of vitamin D in the maintenance of healthy bones.
Osteoporosis is a weakening of the bone or bone structure
The print materials each provided a clear and unambiguous definition of osteoporosis.
Osteoporosis is a condition where bone structure deteriorates . . . the outer bone “shell” becomes thin . . . weakening the bones and increasing the risk of fracture. (Barwon Health) Osteoporosis means “bones with holes.” Bones lose their strength and density, become fragile and break (fracture) more easily. (Better Health Channel) Osteoporosis is a condition where bones become weakened and fracture more easily than normal bone. (Osteoporosis Australia)
There are many risk factors for osteoporosis
The materials were explicit in the view that there was no single cause or factor that placed a person at risk for osteoporosis. Each publication in this group listed a range of risk factors, and identified those people who might be at higher risk of osteoporosis. They also debunked common myths about osteoporosis being “a women’s disease,” highlighting that both men and women could be at risk.
Several factors can place a person at risk of osteoporosis. . . . Sex hormones . . . have a fundamental role in maintaining bone strength in men and women. (Better Health Channel) Who is at risk? Both men and women older than 20 years, but especially over 50 years of age. (Barwon Health)
Osteoporosis is preventable
Each publication answered an explicit question about whether osteoporosis could be prevented but did not apportion blame or accusation at those who did not follow the recommendations for doing so, for example, “Some things you can do now to maintain or increase strength of bones and help protect against osteoporosis (followed by a list; Barwon Health).
Osteoporosis can be diagnosed and treated
All four publications provided clear and relatively detailed information on how osteoporosis might be investigated and diagnosed, and described the range of available medications and other interventions. Implicit within these materials was the message—delivered in a reassuring tone—that effective treatments were available.
Diagnostic densitometry and specialist endocrinologists are available for referrals to treat and monitor patients with osteoporosis and fractures. (Barwon Health) If osteoporosis is diagnosed early and effective treatments are used, bone loss can be prevented from getting worse. (Osteoporosis Australia) If I need treatment, what’s available? There’s one fact that you really should know about osteoporosis: it’s never too late to start . . . Today, there are several treatments available which may help strengthen your bones. (Merck Sharp & Dohme)
Message 2: Osteoporosis Is a Common Problem Among Older Women. We Should All Try to Maintain Healthy Bones
Within this message, osteoporosis was defined as a problem commonly occurring among women at or after menopause. Medications as well as lifestyle factors—essentially, having a diet rich in calcium and regular exercise—were presented as solutions to treating the problem. Readers were repeatedly urged to check their intake of calcium and to seek medical advice about osteoporosis. The four print materials developed by Novartis Pharmaceuticals and the Australian Dairy Corporation (one of these in conjunction with Arthritis Foundation of Australia) published messages that fitted within this cultural conception.
Osteoporosis is a common problem
Although this was not explicitly stated in the publications, they gave the strong impression of osteoporosis being a common occurrence in the community. There was also a sense of heightening readers’ awareness of a pervasive problem.
Approximately every 5 to 6 minutes someone is admitted to an Australian hospital with an osteoporotic fracture. . . . You may have osteoporosis and not know it. (Novartis Pharmaceuticals) The longer we live the more likely we are to develop osteoporosis. . . . Osteoporosis is an increasing health care problem in all aging communities. (Australian Dairy Corporation)
Older women are at high risk
Along with the pervasive presence of osteoporosis in the community was the message in the publications that women were at considerable risk, particularly from the onset of menopause. Statements about men also being at risk were obscured by the repetition of descriptions of women’s risk.
More than half of older Australian women will suffer an osteoporotic fracture during their lifetime. (Novartis Pharmaceuticals) Who are at risk from osteoporosis? . . . Caucasian (fair skinned) and Asian women . . . Women after menopause and women having an early menopause. Women who have dieted excessively. (Australian Dairy Corporation)
Healthy bones are the responsibility of the individual person
The four publications presented the universal message that healthy bones were attainable if the individual person followed certain recommendations. They did not provide guidance outside of those recommendations, but did state that readers should seek medical advice if they had concerns.
To prevent fractures you need to keep your bones strong. (Novartis Pharmaceuticals) The recommended calcium intake chart is a general guide to the amount of calcium we should be eating daily according to our age. Check to see whether you are getting enough calcium daily. (Australian Dairy Corporation; Australian Dairy Corporation and Arthritis Foundation of Australia)
Healthy bones are achieved or maintained through this product
Not only were healthy bones attainable, but they were attainable through the use or consumption of a particular product or product type. This subtype appeared to reflect the publishers’ commercial and/or other interest in producing the publication, for example, the Australian Dairy Corporation’s interest in promoting dairy products.
Your doctor has prescribed Aclasta® to treat your osteoporosis. (Novartis Pharmaceuticals) It is easy to aim for two, three, or four serves of dairy products daily in a balanced diet, and . . . there are many low fat dairy products to choose from. (Australian Dairy Corporation) Dairy foods are best because they are especially high in calcium. (Australian Dairy Corporation and Arthritis Foundation of Australia)
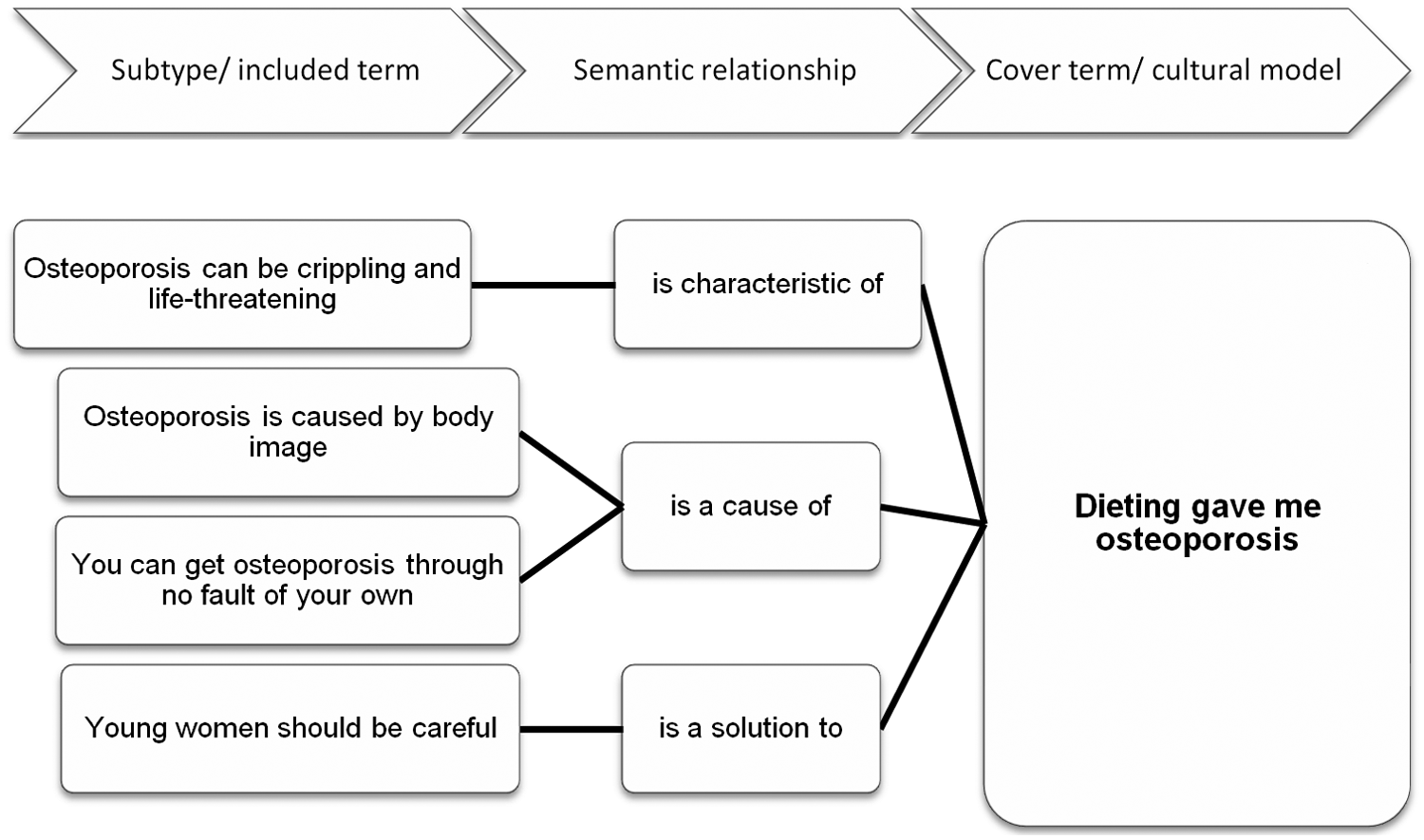
Message 3: Dieting Gave Me Osteoporosis
The two articles by Woman’s Day magazine fitted within a cultural conception of osteoporosis as an alarming disease that could be visited on young women at any given moment, either through no fault of their own, or due to having an unhealthy body image. Within this message, osteoporosis was not so much defined as dramatized into a life-threatening condition.
Osteoporosis can be crippling and life threatening
The articles presented a consistent view that osteoporosis was a cause for alarm.
Former model and actress Britt Ekland . . . weight loss has left her crippled with osteoporosis. (October 2007) [The medical specialist] told me I might only have been a day away from not being here at all. . . . Basically, my body was shutting down. (June, 2007)
Osteoporosis is caused by body image OR You can get osteoporosis through no fault of your own
The Woman’s Day articles present conflicting views on the possible cause(s) of osteoporosis. On one hand, a pervasive desire for a “size zero” body among young women was the cause of dieting, which in turn caused osteoporosis: “‘Dieting is why I now have osteoporosis’, she [Britt Ekland] tells British newspaper Daily Express. Britt says she was plagued by body image problems from an early age” (October 2007).
On the other hand, osteoporosis was presented as a mysterious condition that could arise without prior warning: “The X-rays did in fact show that this otherwise fit, healthy 30-year-old had severe osteoporosis. . . . We don’t really know why I developed osteoporosis.” (June 2007)
Young women should be careful
Both articles highlighted that young women were at risk of getting osteoporosis.
Sue is now determined to let younger women know that osteoporosis can happen . . . at any age. (June, 2007) Britt hopes her story will serve as a warning to young women today. (October 2007)
Discussion
The four cultural concepts that emerged in the present analysis—the cultural model that “Osteoporosis has low salience” and the messages that “Osteoporosis is a serious but preventable condition for which treatment is available”; “Osteoporosis is a common problem among older women, we should all try to maintain healthy bones”; and “Dieting gave me osteoporosis”—highlight the range of views on osteoporosis present in our community of interest. There were clearly discernible differences as well as similarities between the cultural model identified among the study participants and the messages that emerged from analysis of the print materials included in the study.
Our findings from the fracture case study concur with international studies indicating a high level of disinterest in osteoporosis among middle-aged and older women. In a qualitative study conducted in Scotland, Backett-Milburn, Parry, and Mauthner (2000) were surprised to find that only a minority of the women in their study, aged 40 to 55 years, mentioned osteoporosis without prompting, and when they did so there was little interest in osteoporosis as a health concern (Backett-Milburn et al., 2000). Similar findings were indicated by Meadows and colleagues in Canada (Meadows, Mrkonjic, & Lagendyk, 2005; Meadows, Mrkonjic, Petersen, & Lagendyk, 2004), and Reventlow and Bang (2006) in Denmark, where women’s views of osteoporosis were found to be influenced by stereotypes of aging and inevitable bodily decay.
It is interesting to note that while osteoporosis was similarly of low salience among our community case study, these participants were more sanguine about osteoporosis than those in the fracture case study, considering osteoporosis to be a condition caused by age-related thinning of the bones. While this difference between the groups was subtle, it is nevertheless an important distinction; the women in the fracture case study had firsthand experience of the consequences of bone fragility that they did not put down to aging, even if their level of concern about osteoporosis matched that of participants in the community case study.
Our findings from both case studies also concur with a major Australian study suggesting that osteoporosis is considered to be of low salience within the general community. The Australian Better Health Initiative (BHI), announced in 2006, is a large-scale, national communications strategy that uses the threat of chronic disease to motivate lifestyle change among Australians. The primary target for the first phase of the BHI campaign involved 25- to 50-year-olds, and the secondary target 45- to 65-year-olds. In the campaign’s baseline survey (n = 2,506), respondents had ranked osteoporosis 14th in a list of 18 chronic diseases (Miller & Tuffin, 2009). Thus, it would be fair to say that osteoporosis ranks relatively low among Australians’ health concerns, and this is reflected within our case study sample.
The cultural model “Osteoporosis has low salience” included a strong association with the dreaded “dowager’s hump” held by the women in the case studies in relation to osteoporosis. Nevertheless, this association was not sufficient cause for osteoporosis to be prioritized among the women’s health concerns. The Norwegian HUNT study provides an interesting contrast; the women in that study also were reported as holding strong associations between osteoporosis and “hunchedback bodies” (Skolbekken et al., 2008, p. 2570), but they appeared to express far greater concern and curiosity about the condition than did their Australian counterparts—though it is possible that this was as a result of the high level of support for the HUNT study reported among residents of the county in which the study is located.
Notwithstanding the above, why was osteoporosis considered to be of low salience among Australian participants, given that all but one had received a diagnosis of osteoporosis? One reason could be a lack of knowledge about the condition, as suggested by the study cited in our introduction (Taylor et al., 2003). A case in point was one participant in the community case study who had never experienced a fracture and reported having no knowledge of osteoporosis.
Given their recent fracture history, perhaps it would not be unreasonable to expect that participants in the fracture case study would rate osteoporosis higher in their list of health concerns. However, if their fracture experience did not result in a change in their knowledge of the condition, it is perhaps unlikely that it changed their perception of its salience. A recent Australian study by Levinson and colleagues assessed elderly patients’ knowledge of osteoporosis during and 3 months after hospital admission for minimal trauma fracture (Levinson, Leeuwrik, Oldroyd, & Staples, 2012). Levinson et al. (2012) found that knowledge of osteoporosis did not improve in the 3 months after fracture, and concluded that “current strategies for patient education in osteoporosis did not result in increased patient knowledge about their disease.”
Concomitant with our speculation above that fracture case study participants might rate osteoporosis relatively high on their list of health concerns due to their fracture history is the notion that the strength of participants’ views about osteoporosis and its management may be dependent on the proximity of their encounters with the concept of osteoporosis. This might include how long ago participants—or a family member or friend—received a diagnosis of osteoporosis, visited a doctor for a condition that might have exposed them to discussions or health-promotion materials about osteoporosis, or otherwise were exposed to any form of dialogue or information about it.
Another reason for the low salience may be that the women’s own lived experiences were incongruent with the messages they received about osteoporosis from their medical practitioners and/or social marketing materials they may have encountered. Like the women in Barg and Grier’s study (2008), they may believe that these messages do not apply to them because the components of their cultural model of osteoporosis are not addressed in those messages. This was evident in the fracture case study, but not in the community case study. We speculate that views among the fracture case study differed precisely because of participants’ recent fracture experiences. Social marketing messages could be made more relevant to women such as our participants by segmentation or targeting (Kreuter et al., 2000) that addresses their age/life stage, fracture history, and knowledge. For example, a pamphlet provided to elderly women attending a fracture clinic could focus on interventions to prevent a recurrence of fracture, while one provided to elderly women attending a general medical practice would need to provide more basic information relevant to primary prevention of osteoporosis in older women.
We note that this discussion occurs within a societal framework in which the dominant discourse is one of equity in the doctor–patient partnership in health, that consumers are empowered through access to quality information (Henwood, Wyatt, Hart, & Smith, 2003). However, it does not necessarily follow that consumers empowered with information—quality or otherwise—will translate their knowledge into positive health behaviors.
A further complicating factor linked to consumer health behaviors relates to the capacity to access health information and, by extension, the relationship to health outcomes. Access to health information is increasingly universalized through the ubiquity of the Internet, but this access is mediated by socioeconomic factors such as income and employment status (Reinfeld-Kirkman, Kalucy, & Roeger, 2010). The relationship between socioeconomic status and health outcomes is a topic that has attracted much attention in research in recent decades (Huguet, Kaplan, & Feeny, 2008) and may well be a salient factor in how people respond to health communications about osteoporosis. However, studies on the relationship between socioeconomic status and health outcomes among older people are only just beginning to emerge in relation to chronic conditions such as hypertension (Kaplan, Huguet, Feeny, & McFarland, 2010), and a gap remains in relation to income disparity and the prevalence of osteoporosis.
Social Marketing and Osteoporosis
The print materials provided by key stakeholders for inclusion in the study did not send a universal message about osteoporosis. As might be expected, the materials produced by the publicly funded health and information providers (Barwon Health, Better Health Channel, and Osteoporosis Australia) presented messages that were clear, balanced, informative, and reassuring, while those obtained from other sources (pharmaceutical companies, the dairy industry, and Woman’s Day magazine) ranged from laissez-faire statements about osteoporosis and its management to fear-based exhortations for young women to “be careful.” The fact sheet produced by pharmaceutical company Merck Sharp & Dohme was a notable exception, although it was specifically produced for general medical practitioners (this fact sheet was included in the analysis because a general medical practitioner stakeholder had offered it as evidence of information he provided to his patients when diagnosing osteoporosis).
While the first two messages in this section of the analysis appeared to be similar, there was one major difference: the balanced and reassuring approach taken by the public health and information providers, as opposed to the commercially laden messages presented by the pharmaceutical and dairy industry representatives. Both messages presented current and accurate data on the prevalence of osteoporosis, but the communication of this information in Message 2 (“Osteoporosis is a common problem among older women, we should all try to maintain healthy bones”) could have led readers to believe that osteoporosis was far more prevalent than it really was. Older women, in particular, were the focus of these messages. Furthermore, there was a strong emphasis in Message 2 on the individual’s responsibility to maintain healthy bones, primarily through calcium supplementation and osteoporosis medication, and this message was reflected in Cultural Model 1, where some women believed that osteoporosis was lifestyle-related and therefore self-inflicted.
Message 3 (“Dieting gave me osteoporosis”) took a distinctly different approach to communicating about osteoporosis. In these magazine articles, osteoporosis was presented as a mysterious disease to which young women in particular should be alerted. Neither article gave any indication of the known risk factors for osteoporosis, nor its recommended treatment or management. The cultural knowledge conveyed through Message 3, thus, did not reflect the available scientific evidence on osteoporosis, and they also did not reflect Australian policies on raising awareness of the condition.
In 2002, the Australian Government committed AU$11.5 million over 4 years to “osteoporosis awareness raising, support for better self-management and health service improvements,” and in 2006, that funding was extended for a further 4 years (Australian Government, 2006). Under the 2006 to 2010 Better Arthritis and Osteoporosis Care program, activities for osteoporosis included a “Prevent the next fracture” awareness program, a vertebral fracture initiative for general medical practitioners and consumers, an osteoporosis self-management training module, a national osteoporosis multicultural initiative, a vitamin D and calcium awareness program, a national dissemination project for the healthy bones school kit, a national osteoporosis risk factors awareness program, a “Men and Osteoporosis” program, a National Patient Support program, and an evaluated program of community service announcements (Australian Government, 2010). In 2005, the Vitamin D and Calcium Forum, a joint initiative of Osteoporosis Australia and the Australian and New Zealand Bone and Mineral Society, developed recommendations aimed at achieving improved vitamin D and calcium nutrition among Australians; a range of publications targeted to consumer and professional audiences was published as a result (Osteoporosis Australia and Australian and New Zealand Bone and Mineral Society, 2005).
Considering the findings presented in this article, it appears that not much of these extensive social marketing programs have penetrated our study region. While there were some scant references in the print materials analyzed at Messages 1 and 2, none of the messages in these campaigns was reflected in the articles analyzed at Message 3. Having said that, though, it is difficult to obtain clear evidence either way in the research literature; there remains a dearth of research evaluating social marketing campaigns on osteoporosis—the messages imparted as well as their uptake—within the country generally, and specifically in the study region.
The cultural model identified from our case studies, “Osteoporosis has low salience,” did not differ as notably as it diverged from Messages 1 and 2. Given participants’ view of osteoporosis as having low salience, the cultural knowledge in Message 1 that osteoporosis was in fact a serious condition and in Message 2 that it was common among older women might hardly have provided reasons for participants to reprioritize osteoporosis above the health conditions and diseases they had placed ahead of it. Although we do not have evidence that our participants specifically were (or were not) exposed to the print materials analyzed in our study, it is not difficult to see how Messages 1 and 2 may have missed the mark with them. The materials were not particularly well targeted toward women of their age, and therefore participants may not have considered these as being relevant to them (Barg & Grier, 2008; Buckley & Ó Tuama, 2010).
Cultural Model 1 (“Osteoporosis has low salience”) and Message 1 (“Dieting gave me osteoporosis”) could be seen as representing two views on opposite extremes regarding osteoporosis. It is unlikely that the alarmist targeting of young women in Message 3 would have swayed our participants’ views from osteoporosis as a condition of low salience to one that might be life threatening. The use of a former model now aged in her 60s would be unlikely to provide the desired connection with the targeted audience of young women. As shown by Buckley and Ó Tuama, a recent trend toward the use of celebrities in testimonial-style health promotion could have the unwanted effect of “heighten[ing] feelings of disconnection” (Buckley & Ó Tuama, 2010).
Women’s magazines have long been recognized as strong influencers in women’s health education. An extensive body of research has established the importance of this medium in empowering women to be informed about their bodies, their health, and as consumers of health care (Barnett, 2006; Weston & Ruggiero, 1985-1986; Zuckerman, 1998). Thus, the cultural knowledge identified from the print materials in this study, particularly the women’s magazine, could be said to be reinforcing of a perception of the low salience of osteoporosis—clearly an unintended, negative consequence from the perspective of the authors.
Target Marketing Versus Nontarget Marketing
In the psychology of market effects, persuasion is enhanced when there is a match between the message and the target market, while “negative nonmarket effects” may occur when there is not (Aaker, Brumbaugh, & Grier, 2000). In the case of osteoporosis, this presents a strong argument for the development of health messages based on the target market’s cultural model(s) of osteoporosis. By nature of their proximity, older women living in our study region will have shared experiences and problems, so it is not unreasonable to expect that they might have a shared model of osteoporosis and that this model might overlap with the one identified among the women in our study, albeit a small sample. Thus, key features of a shared cultural model might be used effectively to target older women in the region with social marketing messages and interventions that aim to prevent or treat osteoporosis. As already stated, if these features are not taken into account, older women in the community might think that the messages and interventions they encounter about osteoporosis do not apply to them (Barg & Grier, 2008) and that they do not need to change their behaviors in relation to osteoporosis.
The cultural model of osteoporosis that emerged from our case studies emphasized the low salience, or low prominence, of osteoporosis among older women, including those with a diagnosis of osteoporosis and those who had recently experienced fracture. While it is important to note that the views and attitudes represent the women in our sample at this specific age and stage in life, nevertheless, they point to key features of programs and policies developed in the prevention and treatment of chronic conditions such as osteoporosis.
Strengths and Limitations
A significant strength is that this is the only study we know of that has explored and compared cultural models of osteoporosis among consumers and cultural knowledge of the condition as represented in social marketing campaigns, in Australia as well as internationally. However, we emphasize the exploratory nature of the study and the limitations inherent in the small sample. Qualitative explorative studies can offer a deep understanding of the mental or cultural models underlying people’s thoughts or beliefs about a phenomenon, which can be used as a focus for communication about that phenomenon. The case studies presented in this article provide some insights into knowledge, beliefs, attitudes, and cultural models of osteoporosis, and highlight divergent messages implicit in social marketing campaigns implemented through print materials. These findings cannot be generalized to the broader population. Given the considerable gap in the literature evaluating social marketing campaigns and messages related to osteoporosis prevention and treatment, the study signals a need for further research to determine the prevalence of the cultural knowledge highlighted in the present analysis, as well as others extant in the community. Indeed, culture represents a significant gap in the research of health communications (Barg & Grier, 2008). Future research also might helpfully provide comprehensive content analyses of key social marketing campaigns on osteoporosis—in print and nonprint formats—and examine behavioral responses to these. We are acutely aware of the fact that participants in our study may have been exposed to other print campaigns as well as a range of nonprint campaigns, including television advertisements for calcium supplements and dairy products, and this presents a substantial opportunity for future research. A further gap, the perspectives of medical practitioners, is currently being explored in our main study.
Conclusion
We identified cultural models as a novel approach to understanding consumer perspectives of osteoporosis and comparing these with cultural knowledge implicit in social marketing print materials. It is clear that consumer knowledge, understanding, attitudes, and behaviors regarding osteoporosis need to be improved to reduce its vast health burden. But social marketers, too, can benefit from having a deeper understanding of the cultural models that drive consumer knowledge and behaviors in relation to osteoporosis. We echo Barg and Grier (2008) in calling for “prevention models that consider consumers’ lived experiences.” Our findings suggest that broadly formulated marketing messages designed to reach mass audiences may have unintended negative consequences, and that cultural models can be used in developing appropriately targeted, salient messages.
Footnotes
Appendix
Notes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Julie A. Pasco, Geoffrey C. Nicholson, and Mark A. Kotowicz were in receipt of a grant from Amgen (Europe) GmBH, but the funding body played no part in the design or conduct of the study; in the collection, management, analysis, and interpretation of the data; or in preparation or approval of the manuscript.