
Abstract
There is a great deal of literature examining the benefits and relevance of community participation and community capacity building in health promotion and disease prevention endeavors. Academic literature embracing principles and commitment to community participation in health promotion practices often neglects the complexities involved and the flexibility required to work within this approach. This article addresses some of these challenges through a case study of two projects funded by Provincial Wellness Grants in Newfoundland and Labrador, a province in Canada with a strong tradition of community ties and support systems. In addition to addressing the unique circumstances of the community groups, this research allowed the authors to examine the situational context and power relations involved in the provision of services as well as the particular forms of subjectivity and citizenship that the institutional practices support. Recognizing this complex interdependency is an important step in creating more effective intervention practices.
Introduction
Since the Ottawa Charter and the Epp Report in the 1980s, Canadian official documents and academic literature have strongly emphasized the need for individuals, communities, and organized groups to participate in initiatives related to their health and well-being (Goodman et al., 1998). The axiomatic argument behind this emphasis is that, for these programs to be effective, the people for which a program is intended should have a voice in the design and implementation of these interventions, as people’s participation depends on what they consider meaningful and relevant in the context of their visions, experiences, and values (Jackson et al., 2003; Minkler & Wallerstein, 2007; Smith, Littlejohns, Hawe, & Sutherland, 2008).
Public institutions have echoed these community and participatory principles throughout Canada, and they are part of most official documents. For example, the Provincial Wellness Plan (PWP) in Newfoundland and Labrador (NL) asserts that it “reflects an increased focus on a shared responsibility for health and provides direction for promoting health, preventing illness and injury, and increasing the capacity of individuals, groups, communities and sectors to take action for wellness” (Government of Newfoundland and Labrador, 2006).
Although practitioners and researchers in the fields of health promotion and disease prevention have earnestly embraced the rhetoric of community capacity building and the related notions of community organizing, community development, and social capital, working with a community approach is not as straightforward a task as some literature might lead us to believe (Labonte, 2007; Syme, 2004). This article addresses some of these challenges through a case study of two projects funded by the Provincial Wellness Grants in NL, a province where community ties and support systems have been traditionally strong and important. Our research aim was to explore how this sense of community would respond to proactive involvement in health and wellness activities as suggested by the PWP, and how this corresponds to our academic notions of community capacity building.
The Various Meanings of Community and Community Capacity Building
Chaskin (2001) defines community capacity building as “the interaction of human capital, organizational resources, and social capital existing within a given community that can be leveraged to solve collective problems, and improve or maintain the well being of that community” (p. 295). Most related literature elaborates on the multiple dimensions involved in community capacity as well as discusses pathways for its implementation and/or evaluation (Baker & Teaser-Polk, 1998; Chaskin, 2001; Smith, Littlejohns, & Thompson, 2001). Where the positivist approach prevails, the goal is mainly the measurement of these dimensions (Goodman et al., 1998; Hawe, King, Noort, Jordens, & Lloyd, 2000; Maclellan-Wright et al., 2007). The participants in most empirical, quantitative studies have usually been volunteers or staff from health promotion agencies or organizations structured in coalitions (Berger, 2005; Chavis, 2001; Cramer, Atwood, & Stoner, 2006; Francisco, Paine, & Fawcett, 1993) and have rarely involved grassroots members of society (Jackson et al., 2003).
From a more critical perspective, other authors have questioned the use of the community capacity building approach in research and intervention, highlighting the contested aspects of community and community capacity building (Craig, 2007; Diamond, 2004; Mowbray, 2005; Simpson, Wood, & Daws, 2003; Williams, 2004). One of the criticisms is that projects that promote “capacity” and “self-sufficiency” may be guises through which governments minimize their accountability for larger social ills. Community capacity building projects may act as a means to boost the reputations of politicians and government officials, playing upon the well-intentioned connotations that surround the concepts of community, community capacity, and social capital (Mowbray, 2005). This diverts attention from the larger causes of socioeconomic disparities to the responsibility of the individuals living in lower income communities, thereby placing blame on the victim and focusing on “defective” populations (Craig, 2007; Mowbray, 2005; Williams, 2004).
An intermediate position considers that community capacity and its various dimensions are operational guidelines to be monitored or evaluated with participants (Labonte & Laverack, 2001a). From this perspective, the ideas of process and outcome are interdependent, mutually benefiting the outcomes of health promotion programs and the participants involved (Labonte & Laverack, 2001a, 2001b; Labonte, Woodard, Chad, & Laverack, 2002). According to Labonte and Laverack (2001a), community capacity can be more adequately defined as a descriptor of “social and organizational relationships . . . with dynamic qualities rather than static properties” (p. 112). This creates an extra challenge for the health promotion planning process, as it involves incorporating a capacity building relationship. This relationship implies a kind of interaction that favors values of equity and respect, and facilitates participation, leadership, organizational structures, resource mobilization, and critical assessment. These qualities depend not only on internal aspects of individuals and social groups but also on the availability and quality of public infrastructure (Hawe et al., 2000; Labonte & Laverack, 2001a; Laverack, 2006a, 2006b).
The underlying assumption of community in most community capacity building endeavors is of a definable, homogeneous group or a social unit with some kind of affiliation (geographical, social/institutional, and psychological), working with external agents that provide support. The problem with this assumption is the romanticized way the term community tends to be used (Labonte, 2007). As expressed by Labonte (2007), “community ceased to be a subject (a group of people acting with their own intent), and became an object (community as a target of health programs) or an adjective accompanying the real subjects” (p. 83).
This objectification of the term community usually underestimates cultural complexities existing in any group of people, such as different interests, perspectives, and experiences. It also ignores the power relations as well as the fluid and situational nature of human groups (Chiu, 2008). We agree with Walter (2007), who suggests approaching community as a “multi-dimensional-dynamic system (people and organizations, consciousness, actions, and context) of which we are a part” (p. 68). This approach, Walter asserts, “enables us to see ourselves and each other as part of a dynamic system that is continually being created and re-created and that affects and is affected by our consciousness and actions” (p. 70). Consciousness, as part of our subjectivity, involves life stories, sense of identities, language and cultural values, as well as awareness of power relations. All of these play a central role in our social interactions and the kind of social commitments we get involved in (Freire, 1974). It is also clear that by living in social relations, every person or organization is potentially a part of different communities.
For the purpose of this research, we defined community as an orientation for action, as the research dynamic was intended to be a facilitating process to foster assets, resources, and networking possibilities (Simpson et al., 2003; Smith et al., 2008; Walter, 2007).
Method and Methodology
Methodology: A Qualitative Research Paradigm
Considering that every community group has unique circumstances, we chose to study local dynamics through a participatory action-research agenda that was framed as strengths-based, focused on the process, and sustained in notions of sharing power or power/with through open dialog (Minkler & Wallerstein, 2007; Walter, 2007). Three particular features characterize participatory action research: shared ownership of the research project, community-based identification and analysis of social problems, and an orientation toward using research results to facilitate community action and change (Kemmis & McTaggart, 2000). Incorporating these features ensures that research is conducted in a manner consistent with community values and that the research process and findings are relevant to the people involved.
Method: The Research Process
In the first stage, we performed a literature review, with a special focus on the different community capacity building frameworks and evaluation tools that have been developed both in Canada and internationally. We also contacted provincial and regional health and wellness authorities to form an advisory committee to support the research team. This research was approved by the Human Investigations Committee of Memorial University in August 2009.
Selecting community group participants
The selection criteria as defined in the research proposal were (a) a community group that is fairly conscious of/experienced in the affirming and challenging elements inherent in the process of community capacity building and that will welcome additional support from the research-intervention process and (b) a community group relatively inexperienced in community capacity building and uncertain of how to form relationships that will enhance their initiative, contribute to its successful execution, and disseminate the knowledge and experiences acquired.
Notably, within these criteria, the selection of the programs submitted was solely based on the quality of the funded proposals, as evaluated by the Provincial Wellness Committee. After a thorough study of 32 health promotion initiatives from the region funded by the PWP for 2010, we selected two community initiatives from one of the nine rural regions in the province: (a) one focused on a community kitchen program at a community center in a social housing neighborhood of the largest town (about 4,000 inhabitants) in the region and (b) another more generally focused on wellness activities developed at the community center of a small town in an isolated area of the same region. To preserve the confidentiality of the individuals and their places of residence, we refer to the two participating community groups as “Site A” and “Site B.”
A Provincial Wellness consultant facilitated initial contact, and we prepared a two-page informative summary for our first meeting with the two groups. The meeting included a motivational presentation of the research and objectives, highlighting the tenets of the participatory-action research approach and an open discussion to enable the groups to determine their interest in participating in the research project.
Research methods
In addition to the literature review, we collected data through participant observation, informal conversations, group interviews, and individual interviews. Two key informant interviews provided the opportunity for service providers from the region to expand on their personal experiences (Murray, Pullman, & Rodgers, 2003).
Participants signed informed consent forms before every group discussion at both sites. The attendants were usually divided into smaller groups of three or four to discuss the questions and later presented their answers to the entire group. The data from this later group discussion were recorded and transcribed. In each new meeting, the principal investigator (PI), responsible for the data collection process, systematically presented the main points from the previous meeting for participants to confirm or comment on. From May to December 2010, we held four group discussions and six individual interviews at Site A, with a variable number of participants ranging from 6 to 13. At this site, in addition to the PI and a research assistant, the community kitchen facilitator and a staff member from the neighborhood attended the group meetings. Most of the group participants at this site were female, with the exception of three males in one of the sessions (1 staff member and 2 participants).
At Site B, all participants were female and the two members of the research team were the only nonresidents. Participants at this site decided to have only group sessions, and we jointly planned and held four meetings with a variable number of participants (5-34). A possible explanation of this preference may be that they felt they had greater control and confidence over setting the agenda by publicly revealing the extent to which their views were shared by peers. However, a known drawback to group discussion and focus groups is that participants may not be as candid in group settings as they would be in private, clinical settings (Wilkinson, 1998). Also, the moral dimension of health tends to limit the degree of disclosure in public settings, as opposed to private, face-to-face interactions (Radley & Billig, 1996).
Considering the differences between the sites, we have organized the data from each place according to the guiding themes: participants’ ideas about personal and community health, how they framed community capacities or strengths, and how they felt with regard to their funded program.
From the beginning, we realized that although we expressed our openness to work with the participants in a participatory action-research agenda and they accepted, this was still our idea rather than theirs. Because the research was not an initiative coming from the participants, we were seen as authority figures no matter how we framed our role in the research process. On occasion we felt that participants’ responses were being tailored to fit what they believed the researchers wanted to hear. Therefore, the analysis of the data will explore interactions between participants’ accounts and the research context, the institutional health agenda, and the ways the social and institutional environment has built particular forms of subjectivity and citizenship.
Overview of Findings
General Social Background
The area where both research sites are located is one of the nine regions of the Rural Secretariat in NL. Almost half of the population is concentrated within the two central towns, located near one another, and the other half is widely dispersed in the vast region. The main economic activities include tourism, seafood processing plants, and one medium-sized industry. Like other rural areas, the region faces many challenges, including a stagnant economy, increasing out-migration rates, decreasing employment levels, and an aging population (Eastern Health, 2006).
Interviews with regional service providers highlighted that members of communities in the region generally adopt a skeptical attitude toward newcomers. This is most noticeable among the older population. Communities tend to remain isolated due to geography and shy away from talk of amalgamation. We found that mistrust came from the struggle to allocate scarce resources. However, participants recognized that the amalgamation of schools has promoted contact and acceptance among youth from different communities. Another barrier they identified was the lack of public transportation in the area. Specifically, public transportation was restricted to a local taxi service. In addition, people do not want to travel after dark or in the winter due to road conditions and isolation. In other cases, individuals are unable to afford travel due to cost or limited access to vehicles.
Relevant social networks are limited to family and friends. The only grassroots organization at Site A is the Tenants Association, but members asserted that participation was rather limited. At Site B, there is a “Recreation Committee” and a “Come Home Committee,” but the two committees consist of many of the same people.
Most participants recognize that the older generation experiences technological barriers, as knowledge of the Internet is generally limited to the younger generations. The inconsistency of Internet access and a lack of computer skills were acknowledged as problems by participants from both research sites.
Program at Site A
The program’s main focus was on a community kitchen, but it also examined other areas related to health and well-being such as physical activity, tobacco control, and environmental health. The community center, mainly funded by the Newfoundland and Labrador Housing Corporation, was responsible for running the program. The center provides services for approximately 110 families living in the neighborhood, of which fewer than 25% of the family heads are employed.
Summary of the Collected Data
Program Background
The community kitchen program was started by volunteers in 2007, with a small group of consistent participants both from within the neighborhood and from without. The program was, at the time of the research (2010), facilitated by a paid community kitchen coordinator in biweekly sessions with four to six participants per session due to the limited size of the kitchen. Although they received the funding from the Provincial Wellness Grants Program, participants emphasized that the main problem was the sustainability of the kitchen due to the loss of momentum when funding expires. This was a permanent concern, as organizations can only apply for grants once per program. A staff member expressed that for the past 3 years, each time the community kitchen exhausted its funding it also lost connections with the people who had been attending its cooking sessions. A lack of funding might result in the loss of the kitchen program coordinator, which could be another setback to maintaining relationships with participants of the program.
Health Concerns
The first session focused around the question “What things are most important to me in terms of my health?” The main issues identified by the group interviews included (a) quitting smoking, (b) healthy eating, (c) more volunteering and involvement in community life, (d) exercise/active lifestyle, and (e) access to sports and recreation activities. In all of the sessions, people highlighted how important the kitchen gatherings were for their mental health. Other aspects mentioned included a good social life, caring for older people, having regular checkups, laughter, meditation, being careful to prevent injuries, and knowledge and awareness.
Throughout the research, participants emphasized healthy eating as a priority, but it became clear that the social environment plays a strong role in defining eating habits and food choices. In one interview, we learned that a participant in her late 50s had never eaten uncooked greens in her life and was not about to begin. Another interviewee explained that she had a preference for boxed macaroni and cheese because it tasted good and was affordable. In a group discussion, it was also emphasized that not having private transportation (and having no public transport available in town) results in many people in the neighborhood relying on frozen or canned food rather than fresh items.
With regard to health in the community (“What things are most important when we think about health in our communities?”), participants mentioned both the high number of “youth with problems” and vandalism as ongoing issues. Concerns about youth were mainly related to substance abuse problems. Arguments to explain substance abuse included easy access to drugs and alcohol in the neighborhood and lack of services to help people with addiction problems. The community center staff hope to counteract the problem through information sessions with local police and health authorities. They noted that they expect things to improve with the arrival of a new addictions and outreach counselor recently hired by the regional health authority.
Concerns over the health and isolation of some seniors were also expressed, remarking that seniors often find it too difficult “to cook just for themselves.” Participants also discussed the need for outdoor and indoor spaces for physical activity and recreation. However, one participant commented on the difficulties of engaging people in healthy lifestyles: despite the existence of gym equipment in the same building where the kitchen sessions were held, the equipment was rarely used. There is also a walking trail about six blocks down the hill from the community center, but most participants have only taken short walks in the past, complaining that they suffer from “shortness of breath,” due to smoking and being overweight. When one of the youngest women in the group was vocal about her success in quitting “because of medical advice regarding lung problems,” a few others expressed a wish to stop smoking as well, which shows the relevance of local role models.
In two of the four group sessions, participants lamented the lack of involvement of many people in the neighborhood, arguing that “there is a lack of community togetherness.” Issues of trust were mentioned, for example, while discussing the failure of the Block Parent program for promoting neighborhood safety, commenting that getting involved “could be dangerous.”
Community Assets
The second group meeting focused on the strengths and assets of the community. When participants were asked about what they considered to be positive community resources, it was difficult for them to reflect on “community strengths or assets.” When we prompted them to express their personal strengths, a different range of ideas came easily, from being a supportive/caring person and volunteering to helping elders and having good housekeeping abilities.
However, the only thing that the group mentioned with regard to “community capacity” was “community togetherness,” referring to the large event Come Home Year 2008, which brought many of the people in the town together. During this event, the community kitchen set up a booth to provide snacks, increasing the group’s visibility in the community. As in the previous session, participants felt events and gatherings are needed “to catch the interest of others in community actions to promote health” and to make a concentrated effort in finding alternative funding to sustain the community kitchen. They also emphasized as positive a 6-week program designed by the community center staff to prepare people for working opportunities, which has been beneficial “in raising self-esteem.”
When prompted again to think of other community strengths, group participants highlighted needs instead, including (a) more personal commitment and community participation; (b) finding ways to help the community; (c) helping kids to stay in school, achieve higher education, and have better job opportunities; (d) knowing how to get a job or having more incentive for people to get off income support; (e) a new literacy program for all ages; (f) skills development for all ages; (g) supporting elders, youth, single parents, and minorities; (h) a neighborhood watch; (i) education for parents/policy support; (j) social outings and recreational activities for all ages; (k) home support for new mothers; (l) more involvement in community well-being from government, general population, and youth; (m) fighting against drugs and alcohol; and (n) implementing a community van or public transportation. Their lack of power to tackle these complex issues themselves was evident throughout the research.
The Challenges of Community Transportation and Participatory Engagement
During the third meeting, we invited participants to choose a priority out of the main areas of interest discussed in the previous session. Participants chose to discuss the need for a community van, as the lack of public transportation is a major issue for the people in the neighborhood. However, it was a challenge to get people to tackle this issue and engage in the solutions to their own problems. The common response was “let’s talk to [the director of the center] about it to see what he can do.” Participants felt discouraged: in a previous attempt a couple of years before, they had had a van serving the neighborhood for a few weeks, but the service was shut down due to the influence of the local taxi company. Events such as this illustrate how institutionalized power relations hamper a community’s sense of control and reinforce a “why bother” attitude.
Self-evaluation survey
The final session involved a written evaluation of the kitchen program and brainstorming of ways to add the community garden idea to the community kitchen project to apply for a further institutional grant. The evaluation and consultation with community members was suggested by the researcher, but only five participants and three staff members were present in the final session.
The community kitchen was not only valued as a space for health education and nutrition, but more importantly, it also acted as a place for socializing and recreation, which might be a far more relevant outcome to judge from people’s expressions and experiences. Still, a main drawback was the program’s sustainability due to the lack of consistent funding.
Participants considered the greenhouse and the community garden positive adds-on to the community kitchen program. They recommended that the garden be located close to the community center so that everyone would benefit from it. However, they also suggested fencing the garden due to possible vandalism and a lack of trust in some of their neighbors.
Reflection on Research Site A
The community center staff care about the community participants, and community members consider staff “nice at doing their jobs.” In the service provider–client dynamic that we observed, community members tended to rely on community center staff to handle problems, as was noted with the transportation issue and, previously, with the addictions and vandalism problems in the area. Another evidence of the participants’ lack of initiative is the way the kitchen program is organized. To guarantee participation in the kitchen sessions, the kitchen coordinator telephones to ask who is available for the next day as a sort of invitation or reminder. When there is only a calendar of sessions or when there is no reminder, people tend to simply forget.
Staff members feel immense pressure to show the results of their hard work. With inconsistent, limited, short-term funding, service providers tend to develop proposals based on what is offered by the funding agencies. With this in mind, they often write proposals for neighborhood programs with little or no consultation from the potential participants. As they cannot be sure that they will get the funding, they argue that they prefer not to create expectations in the participants. Considering the institutional setting of social assistance, the risk of developing patronizing relationships with participants is permanent, perpetuating the cycle of dependency. The complexity of this dynamic is clearly expressed by a staff member:
Here, their parents were in the system, they’re in the system, their children are in the system. And that cycle never seems to be broken . . . they can’t live without the government now because they do not make enough. If they go out to work for minimum wage, they’re making less than being home on social services because then they got to pay their own rent, their own drugs, their heat and lights.
For different reasons, lack of trust among neighbors is common, and although some families live in the neighborhood for generations, mobility is also high due to the transient nature of the subsidized housing program. This poses another problem in gaining consistent participation, as some people may move as soon as they can afford a different living arrangement.
Due to the complexity of problems arising from low-income sectors, a focus on healthy eating proved to be very limited in its approach, and thus it is also important to explore ways to improve the unequal distribution of access to social and economic resources.
Program at Site B
Following the call for grant applications, the program at Site B focused on all the priorities of the Provincial Wellness Grant Program, seeking to promote general good health and well-being. The Recreation Committee, who presented the proposal, welcomed the research project and expressed its decision to use the grant money to support wellness activities such as seniors’ mobilization, catering for outreach events, buying sports equipment such as basketballs, and for transporting people to and from a swimming pool in another community.
Summary of the Collected Data
Program Background
The Recreation Committee, formed by 12 women in this small community of about 200 persons, was determined to keep the community center running and to provide wellness activities, as the center is the only place for socializing in the area. About 25 years ago, the church donated the community center building to the town and for a long time, it was used only occasionally for dancing or darts.
The community is one of a group of four very small isolated towns in the area with a total population of 870 people. Although there is no history of cooperation between these communities, things may change for the new generation as children from all four communities now share a K-12 school. Almost half of the population between ages 18 and 64 have not finished high school. Out-migration has been high, and personal income per capita (after tax) was Can$10,800 in 2006. The unemployment rate for people aged 15 and older was 45.6%. Employment during the full year was only 13.8% in the region. A total of 65.9% worked seasonally and supplemented this income with employment insurance, whereas 12.5% received income support. The 2006 self-reliance ratio—a measure of the community’s dependence on government transfers—was 54.8% (Newfoundland and Labrador Statistics Agency, 2010).
Health Concerns
As at the other research site, the focus of the first session was to discuss the question “What things are most important to me in terms of my health?” The three discussion groups during this session noted three areas of importance: (a) getting exercise; (b) enjoying outdoor activities, such as gardening—a self-sustaining activity for some of the participants; and (c) eating healthy, home-cooked food. Other important aspects included being around their children and doing activities with them, getting enough sleep, volunteer work, cooperative living and support for each other, access to community services, socializing, stress-free life, and the freedom of living in a small community: “a safe place for children to grow up.” Some participants smoked, but only one of the participants, in private, mentioned quitting smoking.
In response to the question “What things are most important when we think about health in our communities?” participants focused on caring for their physical environment and the outdoors. A couple of gardeners who grew vegetables and flowers every summer suggested starting a community garden to get children and seniors engaged in active living.
Participants also considered organizing a wellness fair to share their ideas and experiences with the other communities nearby, with the expectation that people in these towns may want to join in on activities at the local recreation center or set up wellness activities in their own towns. Like in Site A, they also considered social events a good strategy for bringing people together, as a recurrent complaint was the lack of participation.
Community Assets
During the second meeting, there were 25 participants and the focus was on strengths and assets in the community. They felt positive about (a) the Entertainment/Recreation Committee; (b) the fire brigade; (c) a small church group; (d) the “Come Home” Committee, which was organizing a gathering for 2012; (e) celebrating holidays with dances (i.e., Halloween, Canada Day, Christmas, New Year’s Eve, Valentine’s, and St. Patrick’s Day); and (f) hobbies such as fishing and gardening. In addition, they were glad that (thanks to the community center) seniors, who were rarely active, had become engaged in activities such as storytelling and Bingo.
A significantly gendered attitude toward active living was highlighted. Participants asserted that when men retire or are without work, they tend to be more sedentary than women. As some of the women commented, they “just watch TV or hang with friends.” They spoke fondly of a now-defunct softball team in the community, and shared the concern of trying to engage men and youth in outdoor activities.
Conflict and Loss of Leadership
In an informal meeting at Memorial University with the two leaders of the Recreation Committee before the next scheduled group meeting, the leaders expressed great expectations about the following group discussion to define the activities to be developed during the next months. Unfortunately, the scheduled meeting was canceled because of conflict and division in the Recreation Committee. These two leaders and primary contacts, as well as two other members, resigned and stepped down from the committee, creating a leadership void.
Meeting the Remaining Members
After the PI contacted the remaining committee members, we organized a new meeting with them. They discussed the positive outcomes of the Wellness Grant, which had given them resources for keeping the community center functioning, allowing them to develop activities with seniors and children, to celebrate events, and to hold an exercise class on Mondays and Thursdays. They emphasized that seniors enjoy meeting at the community center and it may be the only activity outside their home available to them. Committee members insisted on the idea of bringing in more participants and encouraging community members to become vocal about the future of the Recreation Committee. They suggested a forum, decided in favor of a written evaluation, and anticipated a high number of participants to the event. The date was set for a week later, and they agreed to invite a well-known regional physical educator as a motivational guest speaker. However, without leadership, there was less enthusiasm.
Site B self-evaluation survey and public forum
It was notable that instead of doing the organizing themselves, the committee decided to hire a former committee chair not living regularly in town to organize and facilitate the public forum, prepare the draft of the survey, and be responsible for the reports for the Wellness Grant authorities. The limitations for engaging participants were again evident, as only 13 local adults and 6 children attended. They handed in the self-evaluation survey at the end of the meeting. All the community members considered the community center a positive asset, and with different expressions agreed that they enjoy the community center events and the sense of community these events provide. When asked about improvements to community programs and events or suggestions for new programs, most participants requested the traditional programs and information sessions encouraging healthy lifestyles, such as healthy cooking classes and exercise programs.
Participants acknowledged in the survey that structured programs and improvements to the community center require participation in and commitment to administrative tasks. However, only 2 out the 13 participants expressed willingness to help in the tasks involved, and none of the participants wanted to assume a leadership role.
Reflection on Research Site B
When visiting the areas near Site B, there is a sense of how isolated these rural communities are. Many of the houses are only inhabited in the summertime. However, among those who stayed year-round, it was evident that they enjoy the isolation of the community and “living their way.” At the beginning, a sense of mistrust was expressed in informal conversation, as a couple of participants asked the PI, “Why do you bother coming this far?”
Except for the most outspoken leaders (who resigned), the other members openly resisted getting involved in leadership positions. However, despite the conflicts within the Committee Board, a sense of community is evident in the informal relationships they maintain. They all know their neighbors, who are often family related and are open to help in critical situations, especially with the elderly population.
Discussion of Research Findings
Although Newfoundlanders and Labradorians are often known for their sense of community, we questioned whether this sense of community held the same connotations as the rhetoric around the often reified terms of community and community capacity found in some academic definitions and official documents. This research endeavor faced limitations: the geographical distance of the research site, the short-term funding of the programs, and the ambivalence of the programs’ funding agency with regard to involvement in the research. Our status as “outsiders” placed additional limits on our research with both funding agencies and community groups.
Other research efforts conducted in this rural area (Eastern Health, 2006; Gibson & Vodden, 2010) as well as in other regions of rural NL (Close, Rowe, & Wheaton, 2007; Gray & Sinclair, 2005; House, 2003) have observed the locals’ cautious attitude toward outsiders as well as an evident aversion to formal community involvement and/or assuming leadership roles. Critical international literature on this topic argues that organized grassroots groups are usually part of the “better-off” sectors of society, whereas in many small communities and low-income sectors, informal cultures of engagement prevail (Williams, 2004).
The evaluations of the Newfoundland and Labrador Heart Health Program (2002; Holmes, Neville, Donovan, & MacDonald, 2001) and the subsequent PWP (Department of Health and Community Services—Government of Newfoundland and Labrador, 2008) also identified that there is a need for continued resources and efforts to enhance leadership and the capacity to mobilize communities, to recruit and train participants, and to maintain ongoing communication of shared knowledge and experiences.
As these concerns remain part of the PWP’s rhetoric, the researchers juggled this challenge with the main research agenda, focusing on whether the PWP programs could adequately engage local people within the unique context of each group. Instead of simply accepting the official rhetoric, the social complexities of community groups prompted the main researcher to focus on studying the particular community dynamic (i.e., geographic and social background) of each program in these two different sites and explore the specific situational context as related to both institutional public health practices and to the way services and programs are provided. We also investigated how much participation is influenced by the particular forms of subjectivity and citizenship that the sociocultural environment is generating with regard to health (Bunton, 2008; Lupton, 1999). We argue that social context, institutional practices, and forms of subjectivity are intricately interdependent, and recognizing this complexity might help us to reflect on ways to develop more efficient intervention practices.
The Social Context
In the case of Site A, the program was designed as a service to a particular neighborhood, characterized by low-income residents and exposure to different degrees of social exclusion and vulnerability (Stephens, 2008). Our research shows that a sense of cohesion and a sense of control are very limited among people living on social assistance. Although their health is highly influenced by the conditions in which they live, people often seemed powerless to make any kind of change about “the way things are,” as clearly evidenced in the case of the public transport issue. Dependency on others to provide for them is a learned behavior and influences their ability to make changes in their lives. They usually rely on what paid community center staff, as intermediaries in the provision of these programs, can provide.
We witnessed that the most popular programs in the neighborhood are those addressing more vital services for families, such as early childhood and children’s school support, and those that provide work experience, as most of our participants wanted to find a job. Nonetheless, the way funding is provided forces community center staff, as much as other service providers, to offer the services within a top-down relationship. As funding is not always guaranteed, they are hesitant to consult with community members for fear of creating expectations that may go unfulfilled.
Staff are usually constrained by limited economic resources as well as by the complexity of the problems involved. People open to receiving services tend to passively avail of what is offered. Still, for some socially disadvantaged groups, health-focused programs may even be perceived as an additional source of stigma and therefore a space for resistance; this is likely one of the reasons why some people refuse to participate (Stead, McDermott, MacKintosh, & Adamson, 2011).
The sense of community was often expressed in informal ways through “looking out for the elderly people in the neighborhood” and “caring for family and friends in need.” The fact that grassroots members in these community groups often do not fit with our academic conceptions does not by any means imply a lack of skill on the part of residents or even staff. More vulnerable sectors of society are more likely to engage in “informal” community relationships (Chappell, Funk, & Allan, 2006; Rapport, Snook, Evans, & Tee, 2008; Williams, 2004). While these informal supportive interactions are not often identified by community members as social capital or community capacity, they still have beneficial effects for the people involved. Failing to see this different kind of engagement, as Williams states, “not only underemphasizes a culture of community participation that is widespread but also ends up imposing onto less affluent groups a relatively foreign form of community involvement that does not mirror their current participatory cultures” (pp. 737-738).
Similarly, there are challenges often faced by rural, isolated communities in NL that were observed at Site B. One difficulty encountered is community members conditioned to staying within small, familial networks, “minding only their own business.” While we uncovered much evidence of how important informal social relationships have been for the well-being and survival of community members, there was an overt rejection of engagement in the Recreation Committee’s tasks, which ended with the resignation of the main leaders of the organization.
However, as Mowbray (2005) argues, government-funded community programs may not be adequately tailored and/or appropriate for populations with low levels of formal social cohesion. In these cases, capacity building strategies to engage people in the programs must be part of the human investment, both in the case of nongovernmental organizations as well as less-structured groups lacking the necessary organizational skills (Labonte & Laverack, 2001a, 2001b). This fact moves us to analyze the institutional background.
The Institutional Public Health Practices
Research findings reveal that there are challenges to participatory-action endeavors without structural support, local resources, and contextual considerations of the manner in which health promotion services and programs are provided (Carr, Lhussier, Wilkinson, & Gleadhill, 2008).
The broad mandate of the government funding agency and the prevailing biomedical model of public health have institutionalized vertical forms of intervention (Bunton, 2008; Lupton, 1999). An institutional deficit-focused approach prevails, and both service providers and lay people have in mind this expert–health consumer relationship. While participants were discussing the youth with problems in the neighborhood, for example, the focus was on pathologizing the condition, disregarding the social, economic, and political environment of the issue. The expectation for a solution was then placed upon the addictions expert. Also evidenced in the selection process and the official literature of the PWP is the fact that the health promotion interventions that receive funding are mainly addressed to change individual lifestyles and behaviors. The challenge remains to incorporate the role of the socioeconomic and cultural environments influencing the “unhealthy” choices.
During the research process, we experienced firsthand that without a joint commitment with programs’ funding agencies, our ability to support the capacity building of both research sites was limited, as the two groups were only accountable to the agencies from which they received funding. Although Wellness Consultants maintained sporadic contact with both community groups throughout the research process, Newfoundland’s geography and other structural limitations (i.e., consultants’ workloads and other institutional priorities) prevented the consultants from being personally involved with the researchers and participants in these communities and from developing a parallel “empowering” track, as suggested by Labonte et al. (2002), Laverack (2004), and Laverack and Labonte (2000, 2006a, 2006b).
We contend that the level of commitment for capacity building should function both ways: a political, top-down conviction on what is facilitated and a bottom-up involvement in what is likely to be achieved. This relationship is always interdependent, as neither group can achieve its goals without the other (Laverack & Labonte, 2000). To visualize this experience, Figure 1 depicts the research environment.
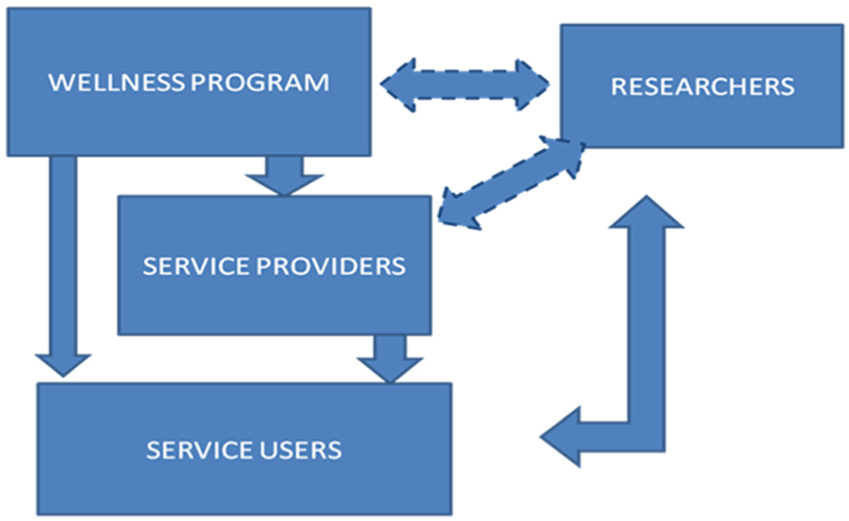
Visualization of relationship between researchers and other parties
The Social Environment and Forms of Subjectivity and Citizenship
Having highlighted the local and institutional constraints, we would also like to highlight the strong macroeconomic forces at work against the formation of meaningful relationships in the society. Globalization has made governments more likely to submit to the pressures of transnational market forces, where policies tend to be neoliberal/market driven, encouraging people to see themselves as consumers of services, rather than as participant citizens with rights and responsibilities. In addition to consumerism, wherein well-being is expected to come from external sources—for example, buying and using products and services produced by professionals and experts—individualism is another stronghold of the market-driven economy, as human beings are considered self-made agents whose plans, intentions, and behaviors take place in isolation from others and their broader environment (Traverso-Yepez, 2008). As Bauman (2001) argues, the more we lose a sense of being able to work with fellow citizens toward a common goal, the more the notion of community becomes nothing more than an idealized dream.
There is a contrast between the health promotion rhetoric of participation and capacity building and the individualism and consumerism trends encouraged by the economic system. Apart from health care, vital services and programs related to wellness in neoliberal societies like Canada’s are treated as an individual/private concern, and the current institution of health promotion programs with limited, short-term funding seems to mainly target the most vulnerable sectors of society. This minimalistic approach does not favor the creation and development of a sense of community.
There is also a culture of dependence on government services, which reflects the unanticipated effect of the provision of the social safety net in the postwar period of the 1950s; and more importantly, in the case of rural NL, after the collapse of the cod fishery and the moratoria imposed by the federal government in 1992 (Ommer, 2007). Those who stayed in rural communities moved away from self-sufficiency and became more dependent on services provided by government agencies.
Final Considerations
Our research demonstrates that communities are dynamic, mobile systems formed through the specific motivations of participants, with the power to avail (or not) of organizational resources and human and social capital to engage in higher levels of commitment. Consequently, it is clear that community capacity building cannot be designed or planned from outside, but must be consensually built by the stakeholders involved.
In our work with Sites A and B, we witnessed a demand for a broader approach to health and more intersectoral partnerships at the local, municipal, regional, and provincial levels. Distant/isolated communities and low-income sectors of NL may benefit from partnerships between the health sector, the Rural Secretariat, and local municipalities to support more integrated capacity building efforts. However, the health sector and the Rural Secretariat continue working within their own domains.
As these expectations were also beyond our power as researchers, we experienced firsthand the importance of a flexible program structure in addressing the unique circumstances of the two specific community groups (Carr et al., 2008). We learned once again that, considering the power relations and conflicts that are present in any social interaction, whenever immersed in community actions and working toward a common good, it seems more appropriate to think about “community capacity building” in terms of a dynamic set of values involving different degrees of commitment, solidarity, and, most importantly, openness to negotiating differences.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research has been funded by grants to Martha Traverso-Yepez from the Industrial Research and Innovation Fund (Grant Number 206949) and Memorial University of Newfoundland (MUN) Medicine Start-Up Fund (Grant Number 205973).