
Abstract
In 2010, nearly 400 million women worldwide were of menopause age (45-54). Although many women transition through menopause with ease, some experience distress and a subsequent decrease in quality of life. The purpose of this qualitative study was to examine the experiences of distress in women during the menopause transition. A narrative analysis methodology was used maintaining participants’ complete narratives when possible. In-person interviews of 15 midlife women were digitally audio recorded and transcribed verbatim. Women shared narratives of distress related to menstrual changes, emotional instability, vaginal dryness, and decreased libido affected by their relationships with self, partners, work, and family. Some experiences were presented against a backdrop of the past and influenced by concerns for the future. Detailed stories illuminated the effect that distressful symptoms had on quality of life and captured how intricately woven symptoms were with the women’s interpersonal and social lives.
Keywords
Introduction
In 2010, there were nearly 400 million women worldwide of menopausal age (45-54 years), and nearly 500 million women will be entering the menopause transition over the next 5 to 10 years (United States Census Bureau, 2010). Although many women transition through menopause with minimal discomfort, studies have shown that some women experience distress during the menopause transition (Alexander et al., 2007; Bauld & Brown 2009; Gold et al., 2004; Woods & Mitchell 2005). In addition, for some women, a decreased quality of life is an unfortunate consequence of distressful symptoms during the menopause transition (Avis et al., 2009; Blümel et al., 2011; Elavsky, 2009; Utian, 2005a).
Treatment for women during the menopausal transition, specifically hormone therapy (HT), has raised concerns for clinicians and women (Theroux, 2010; Writing Group for the Women’s Health Initiative [WHI], 2002). More than ever before, women seek alternatives such as herbs, soy products, and natural hormones (Hill-Sakurai, Muller, & Thom, 2008; Upchurch & Chyu, 2005), but the evidence does not consistently support the efficacy and safety of such treatments (Files, Ko, & Pruthi, 2011; Lethaby et al., 2007). For women whose lives have become disrupted, the medical community becomes a source of support as they seek explanations and assistance for their concerns (Ayuranci, Orsal, Arslan, & Emeksiz, 2010; Blümel et al., 2011; Guthrie, Dennerstein, Taffe, & Donnelly, 2003). However, when women present with symptoms attributed to menopause, the depth and breadth of the women’s experiences elude the health care practitioner and few options exist. What lacks is a clearer understanding of women’s menopausal symptoms within the context of their lives (Utian, 2005a, 2005b; Woods & Mitchell, 2005).
Background
A challenge in the study of distress during the menopause transition is that distress may mean different things to different people, including women and scientists. The inscrutability of distress as a concept precludes the ease by which it can be defined, understood, and measured (Massé, 2000). Generally, research foci tend to reflect three aspects of distress during menopause: (a) the primary experience of distress—anxiety, irritability, angst, depression—often attributed to potential neuroendocrine changes in the brain (Finset, Overlie, & Holte, 2004; Freeman et al., 2007; Rubinow & Schmidt, 2003; Steiner, Dunn, & Born, 2003; Woods, Carr, Tao, Taylor, & Mitchell, 2006); (b) a secondary response to the intensity and impact of empirically supported symptoms related to menopause, such as hot flashes, night sweats, and vaginal dryness (Avis, Crawford, Stellato, & Longcope, 2001; Brown, Gallicchio, Flaws, & Tracy, 2009; Guthrie, Dennerstein, Taffe, Lehert, & Burger, 2004); or (c) psychological states resulting from the emotional responses to menopause or aging (Lindh-A, Hoffmann, Hammar, & Kjellgren, 2007; Ogle & Damhorst, 2005), inability to cope with stressors (Bauld & Brown, 2009; Kafanelis, Kostanski, & Komesaroff, 2009), difficult life trajectories (Alexander et al., 2007), or innate personality traits that cause excessive stress reactions to midlife challenges (Bosworth, Bastian, Rimer, & Siegler, 2003; Kuh, Hardy, Rodgers, & Wadsworth, 2002). For the woman experiencing distress, the contextual background of her life will shape her experience (Strauss, 2011); yet this is nearly impossible to quantify through the use of instrumentation (Massé, 2000). The scope of her experience is beyond a questionnaire.
In a review of studies on menopause, Utian (2005b) declared there is strong evidence to support that only vasomotor symptoms and vaginal dryness can be directly attributed to the endocrinological changes occurring during the menopausal transition. However, he also emphasized that social, cultural, psychological, and environmental factors can influence the variety of responses that midlife women have to various symptoms, and that there is a “need to understand the factors that determine this variation in response” (Utian, 2005b, p. 8). In addition, Woods and Mitchell (2005) raised the concern that “clinicians do not have access to data about the meaning women assign to their experiences” (p. 155). Although efforts have been made quantitatively and qualitatively to study the psychosocial tapestry of midlife women, researchers have failed to capture the details of the rich contextual background of women’s experiences of distress in menopause.
A midlife woman’s life is complex; she is situated—physically, hormonally, emotionally—in her changing body. She also resides within her social, cultural, and economic environment. Although she has been the focus of a multitude of studies, the factors examined cannot wholly explain why some women experience distress during a normal reproductive transition such as menopause. An in-depth understanding of the physiological, psychological, social, and cultural influences of women’s experiences of distress during the menopause transition is lacking. Therefore, to gain a fuller understanding of the phenomenon, the purpose of the study was to investigate the various experiences of distress that women report during the menopausal transition.
The aim of this article is to present the analysis on the specific context of symptom experience as part of a larger study on distress during menopause (Nosek, 2007, 2012; Nosek, Kennedy, & Gudmundsdottir, 2010). The main research question of the study was as follows:
Research Question 1: From the perspective of the woman during the menopause transition (menopausal years), what is the essential experience of distress?
Method
This study used a narrative analysis methodology (Riessman, 1993). As a way to counter more abstract ideas, narratives create a concrete avenue to explore the understanding of human existence in relation to an individual’s interaction with the world (van Manen, 1990). Examining the rich contextual layers of women’s lives through shared stories of lived experiences allows for the salience of shared meaning embedded in the social, cultural, and intersubjective life world of midlife women (Bloom, 1998; Riessman, 1993).
Participants and Recruitment
Women, between the ages of 40 and 60, who were currently experiencing or had previously experienced distress attributed to menopause and were English speaking, were considered eligible participants (Nosek, 2012; Nosek et al., 2010). Only women who had experienced symptoms as a result of natural menopause or at least had intact ovaries were considered unless the symptoms reported were prior to an oophorectomy. Efforts were made to include women of diverse ethnic, racial, and cultural backgrounds to gain a broad representation of experiences (Nosek, 2012; Nosek et al., 2010). Because this study aimed to capture women who attributed their symptom experience to menopause, no diagnosing of menopause status was required other than what the women reported. Women who were not currently experiencing, or did not in the past experience, distress during the menopause transition were excluded because the specific focus of this study was on women who self-identified as experiencing distress attributed to menopause.
Most study participants responded to advertisements on an online community volunteer board or to flyers at grocery stores posted in two cities in California, USA. The remaining women were recruited through word of mouth or through snowballing techniques. A total of 15 women participated and were offered US$20.00 for each interview.
Data Collection and Analysis
Participants were interviewed in person using an open-ended interview guide and each interview was digitally audio recorded. The principal investigator conducted all interviews of the women who were interviewed once, for 45 min to 2 hr at a confidential place of their choice. A short questionnaire was used to assess demographics such as age, marital status, number of children, education level, and income. Each woman was first asked to share her experiences of menopause and to add any specific stories that would elucidate the distress of her experiences. Email correspondence was also included as data. All data were collected in 2006 and early 2007.
Audio-recorded interviews were transcribed verbatim by a professional transcriber who included interviewer’s questions and participants’ utterances, hesitations, false starts, and phrases to denote expressions such as laughter and intonation changes such as a whisper or loudness of voice. After organizing transcribed interviews in the ATLAS.ti 5.0 computer program, the interviews were read several times with attention paid to emerging narratives and themes. In addition, audio recordings were listened to during the analyses to capture these fluctuations that aided in the interpretation of the narratives. Elements from Riessman’s (1993), Gee’s (1985, 1986), Labov’s (1997), and van Manen’s (1990) methods were used for data analysis. Each offer a different method of analyzing the data but all the methods are within a narrative analysis methodology that emphasizes the identification of stories/narratives as a way of accessing insight to how individuals make sense of themselves and their external world (Frost, 2009). Gee’s poetic structures were employed for the discussion of findings from the larger study published elsewhere (Nosek, 2012) and was especially useful in the relaying of chaos narratives that appeared to have no apparent restitution (Frank, 1995).
Narratives used for this article particularly lent themselves well to be re-transcribed for analysis per Labov (1997) because they contained elements of a true story with the designated components: A = abstract (where narrators denote the beginning of a story), O = orientation (where we are oriented to time, place, and characters of the story), CA = complication action (where actions of the story unfold), E = evaluation (where narrators offer their emotional response or interpretation of the unfolded actions), R = resolution (where actions or crises are resolved), and C = coda (where we are brought back to present denoting the end of the story). The re-transcription of the narratives into elements of a story afforded the salience of what the narrator found important to relay, with special attention payed to the evaluation as it reflects the narrator’s interpretation of the event, and the meaning ascribed to it. Whenever possible, narratives were left whole to maintain the integral threads of participants’ voices and lives. Further details of data collection and analysis are reported elsewhere (Nosek et al., 2010).
Ethical Considerations
The study received ethical approval by the University of California San Francisco’s (UCSF) Committee on Human Research. Written informed consent was obtained from each participant. Confidentiality and the right of refusal at anytime were stressed. Pseudonyms chosen by participants were used in all documentation and recording of data.
Study Rigor
Several practices were employed throughout the study that aimed to establish methodological rigor (Riessman, 1993). Trustworthiness and credibility were enhanced by including direct quotes from participants’ interviews, incorporating member checking, using a research team for analysis, focusing on structure (where stories fell within the text, the utterances, tone, and volume used) and texture/content (the words chosen, the interpretations of experiences given by participants), and spending adequate time with the text to allow for “thick” interpretation (see Nosek et al., 2010, for further details regarding study rigor).
Findings
Sample Characteristics
Fifteen (N = 15) women between the ages of 40 and 59 were interviewed for up to 2 hr each. The youngest participant stated she began experiencing symptoms of menopause at age 31. Close to half of the women were still in menopause transition, and the rest were post menopause. A diverse sample was achieved with ethnic/racial backgrounds that included Latin, Caucasian, and African American. In all, 7 of the women were married or living with a partner, whereas 8 were single or divorced. The women’s employment included a range of occupations, and they were well educated and evenly distributed across income levels (see Table 1).
General Description of Participants (N = 15)
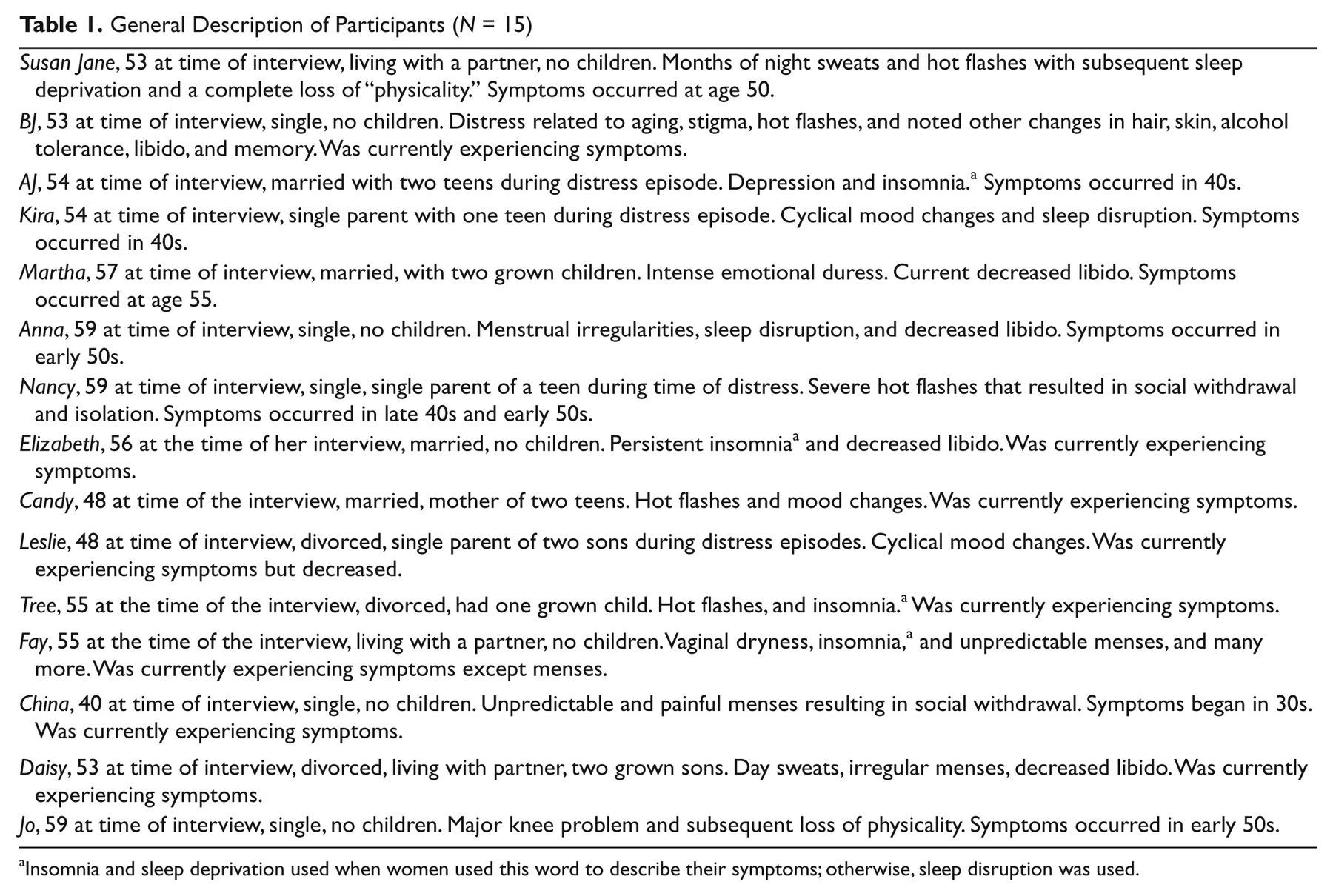
Insomnia and sleep deprivation used when women used this word to describe their symptoms; otherwise, sleep disruption was used.
Symptom Experience
The women reported a range of distressing symptoms such as hot flashes, night sweats, vaginal dryness, decreased libido, mood changes, menstrual changes, and sleep disruption (Nosek et al., 2010; see also Table 1). Findings on a theme related to the stigma of menopause (Nosek et al., 2010), a first person composite narrative of women’s experiences (Wertz, Nosek, McNiesh, & Marlow, 2011), and a case study on one woman’s transformative journey (Nosek, 2012) have been previously reported. The findings reported here are exemplars presented as full narratives that elucidate specific symptoms of menstrual changes, mood alterations, vaginal dryness, and decreased libido. Included also are narratives that portray the consequential impact on quality of life as a result of symptom experiences. Rich details of how the contextual backdrop of their lives pertaining to work, relationships, sexuality, and identity threads through their experiences will be particularly highlighted and maintained via the presentation of complete narratives when possible.
Menstrual Changes
Menstrual cycles that were unpredictable, painful, and heavy were reported by some of the women. One woman (pseudonym China) described the change in her menstrual cycles as her main concern in menopause. China was 40 years old at the time of the interview, and reported her symptoms began when she was in her 30s. She listed other symptoms such as urinary tract infections and sleep disruption, and then illustrated how she arrived at determining her symptoms were due to menopause. “‘You’re a classic case,’ I’ve heard it over and over, you know, ‘for menopause.’”
China occasionally worked as a football game concession worker. She narrated how the unexpected happened one day when she was at work. Her narrative is left intact except for the exclusion of utterances and is presented using Labov’s (1997) narrative approach.
I’m getting to the end of it [period] now. (A) I got my period a week and a half ago (O) and I had to [work] a football game and I was crying, and I thought I had to go pee and I didn’t. (CA) And I … I didn’t get a break. I had to beg for one. I thought I had to [pee] and it turns out it’s my period … It started out as a good day. By the end of it was bad. (E) It was a disaster … (E) It was horrible. Horrible. (E) Had I totally expected it and then, it would have been better. (CA) I just felt horrible. I felt crampy. I felt both. (E) I’m dealing with football fans and it’s terrible. So it was like the whole package. I had to beg for a break because I didn’t know what was going on. (R) I’m talking about like seven hours later. And they didn’t give me my ten-minute break. Oh I’m debating whether I want to go back and it’s not laziness. (C) Well don’t you think they’ll think I’m lazy? (E)
China brought to attention the distress related to the unexpected nature of the experience. However, not only did China have to deal with the physical symptoms of bleeding and cramping, but the demands of the work environment also greatly affected the situation causing her more distress. Amid her discomfort, she was unable to even take a 10-min break. She worried that if she did not return, they would think she was lazy. China clearly painted a picture of a woman anything but lazy, but the unfortunate reality of others’ inability to ever know what she experienced lingered in the aftermath of her story. The experienced distress becomes salient as she describes the unfolding of the day as it started out “good” and slowly turned “bad.” China’s evaluative statements, such as “horrible” (used repetitively) and “disaster,” confirm the impact this one day had for her. The pause that occurred in between the repetition of “horrible” as well as the decreased tone of her voice to nearly a whisper contributed to the listener’s understanding of the narrator’s anguish.
Mood Alterations
Emotional changes that also seemed to be unpredictable with rapid onsets concerned many of the women, and reports of their partners, family members, and they themselves not recognizing who they have become demonstrated the accompanied angst it caused. Martha’s main distressful episode was experienced in the context of a relatively stable work and personal life. Her relationship, a long-term marriage of 25 years, was generally a source of support for her. Her sons were grown and living outside the home. The following narrative about her primary experience of distress was shared at the very beginning of the interview. Her main experience of distress was an emotional episode that lasted only a day or two, but the fear of it repeating and the impact that it could have on her marriage and work propelled her to seek immediate treatment. The re-transcription of her narrative per Labov’s (1997) recommendation affords the reader the ability to follow the unfolding events and elements of this one point in time story.
Um, but the thing … that was really bad (A) was I just suddenly started feeling (O) so mentally out of it … just crazy. (CA) Like just very suddenly I felt … anxious. Uh, I felt anxious. I felt paranoid. (CA) I felt just really, really crazy. And it was like so out of context with my life, but I … I (E) just really felt like it had … it must be hormonal … (E) It just … it was just so off the scale for me. (E) I just went running to the doctor to get hormones, (R) I knew I was either going to lose my relationship, or I (raising volume) was going to lose my job, or I was just going to lose my mind. It’s just like that bad. (E) I cannot possibly function in my life with this. (E) So, it’s … it’s hard to explain, you know. Sudden mental illness. (laughter release) But I just felt so crazy and awful and, you know, just anxious. (CA) And just like I wanted to jump out of my skin. (C)
Martha emphasized the unexpectedness of her experience by using the word sudden twice in the first couple of lines and juxtaposed it with the contrast of her normal state of being. She stressed that she did not recall ever having any incidence like this in the past. Past and future merge in the present moment of her episode. Loss was the main fear for the future against the backdrop of a previously calm mind, and secure job and relationship. Her voice rose during this part of the story accompanied by a serious toned laughter as if the incredulousness of the situation was bordering on absurd.
Candy also shared concerns about mood changes. She relayed a story that included multiple family members, her coworkers, her husband, and her cat. Her mother brought to her attention that her “whole attitude has changed.” Her daughter reprimanded her for “snapping” at her grandmother. She was “edgy” at work because of “the changes.” Her husband just “backs off and he leaves [her] alone.” When asked what she found the most distressful about this, she concluded with, “My attitude, like I said it scares, it scares me. It really does because it’s like I’m a different, totally different person.” Candy expressed fear about not recognizing the person she had become. She came to this realization in relation to what was normal for her in the past. She relayed what was important to her—familiarity of self, and her relationships—at home and at work.
Vaginal Dryness
Fay lived with her boyfriend who was 12 years younger than she. This age dynamic became salient at other points during her interview. She relayed that a great source of her distress stemmed from vaginal dryness during intercourse. The following narrative describes one particular night of lovemaking with her boyfriend and her ensuing distress. This narrative was also re-transcribed using Labov’s (1997) method because it contained all elements of a true story.
Well I can give you a specific day. Um (pause) … (A) I was going through having sex with my boyfriend (O) and I was really enjoying it, and all of a sudden I got really, really dry. (CA) And he’s taking an antidepressant—It took him longer. And it began to really be painful. (E) And he didn’t want to stop (CA) because it meant that he’d have to build up impetus again, (E) and I had to forcibly ask him to stop and use a lubricant, (R) because it was getting painful (E) and I didn’t want to tell him it was getting painful (CA) because he was … I knew if he was hurting me he would stop. (E) He wouldn’t want to go on. And um, I just couldn’t get through to him (CA) because he couldn’t tell that I needed lubrication and it was just a painful reminder that I’m getting old. (E) So now we keep a ton of lubricant by the bed. (R) (C)
The iterative use of “and” revealed by the re-transcription of the narrative draws attention to the incessant layers of the event. The complexity of a symptom such as vaginal dryness unfolds as Fay relays details of one experience. Even after “forcing” her boyfriend to stop and use lubrication seems to resolve the problem, Fay continues on to emphasize the difficulty in achieving resolution and the meaning it had for her. We see how Fay’s boyfriend’s personal circumstance with depression and subsequent use of antidepressants affected his ability to reach orgasm, and amassed the distress related to Fay’s vaginal dryness. Yet, the fact that she “didn’t want to tell him” when it began hurting implied a strong need to care for him and his sexual needs. The 12-year-age difference between Fay and her boyfriend shaped her experience of this symptom reflected in her final evaluation that the whole episode was a reminder of aging. This profoundly portrayed the intensity of the meaning of the experience for her. She chose to discount his contribution to the problem and placed the onus on herself.
Decreased Libido
Martha told of her decreased sexual drive as she shared her concerns: “The other thing that uh, that was distressing to me um, was that my libido was really low … It’s just gotten worse and worse. I don’t like it at all.” She elaborated about why this was distressful to her. “That’s distressing because I think oh, you know, is this guy going to stay with me if I don’t want to have sex, you know?” The gravity of her concern was revealed as she emphasized that “it’s really not a good thing.” The decrease in libido highlighted the context of her concern as she worried about the effect it might have on her relationship. Decreased libido in and of itself was not an issue for Martha; it was the potential loss that could occur as a result that troubled her.
A decrease in libido among married women was not always presented as causing distress in the woman’s life as was the case for Martha. Elizabeth, a 55-year-old woman who had been married for many years, actually welcomed the change in focus that a decrease in libido afforded. She lamented that her previous focus on sex prevented her from doing things such as “research this historical period, or go make a quilt or go dancing.” However, she revealed the key to her success as a married woman with a newfound decreased interest in sex was that her husband had decreased interest also. “And it works in my relationship with my husband and … that’s all that matters. And … that’s what matters.” Her relationship was not threatened by her lack of libido, in contrast with Martha’s experience, and that’s “all that [mattered].”
Work environments, relationships, concerns for the future, and comparisons with the past affected the women’s experiences of distress. The context of their lives contributed to, or more accurately constituted, the distress experienced by the women.
Quality of Life
Various consequences occurred as a result of the women’s menopausal experiences. Some women were concerned that their symptoms would occur in the middle of a social situation and that they would be unable to manage their discomfort and thus would avoid socializing, or some would change lifestyles to compensate—ultimately causing a decrease in quality of life. The following stories depict the consequences of participants’ experiences that contributed to their distress.
What was most significant for China was the development of menopausal symptoms early in life. She addressed how menopause began taking a “toll” on her life quality. The sudden onset of symptoms precluded her from engaging socially for she felt her reaction to them would affect her ability to behave in an acceptable manner. China expressed the distress of this as she explained that she withdrew because she did not “want to lash out at people and be in pain and hunched over.” She felt robbed of her youth elaborating, “I haven’t dated in (pause) 2 years or had a boyfriend in 6. And it just didn’t feel good.” The following narrative by China demonstrates how severely China’s social life had been altered by her symptoms.
You’re going to laugh at this one. (A) This isn’t even a physical thing. This was a day I was actually feeling good. I’ll tell what was the most distressing one. I was going through my temp series; I had ended a job. (O) And I’m going down, I’m in the elevator … and I don’t know if they were lawyers or accountants … get on board. Just asked me if um, (CA) I wanted to join them. I mean as a friend … (CA) I was like I was feeling better but I was like, what if I see them again? (E) What if I come here again? What if I don’t feel good? (E) What if something … what if? You know. (sad voice) I was worried … (E) and I was actually feeling one of my better days. It was distressing … (E) It’s like what if I wasn’t feeling good and they’re wondering (CA) what’s wrong with me and … They’d be wondering why is she so unfriendly? (CA) I didn’t want to come off as being unfriendly. And he was … they were disappointed. (E) That’s how the whole thing came up. (C)
China hesitated to join the party out of fear of what might happen in the future. She worried about the future as she feared seeing the men at a later time when she was having symptoms. It was a fear of what might happen, not only in the immediate future but anytime later, that stopped her from participating in a simple social event. This clearly demonstrated the social impact of her symptoms on her life and the subsequent distress.
Nancy’s main distress was due to frequent and intense hot flashes describing, “as soon as one would go away within the next half hour, one would come back.” The frequency and duration of both the hot flash itself and its “gradual” dissipation created an almost continuous sensation. They affected every part of her life. She quit her gym membership because working out caused an increase in hot flashes. Even reading a newspaper became difficult: “If I was reading something and … and I had a hot flash, I’d probably quit … it would be distractive. I would lose the point of the article.”
Susan Jane addressed a decrease in quality of life as a result of her 9 months of night sweats. She elaborated, “For me it was such a decline in the quality of my life and in the quality of my physicality and the enjoyment of my sexuality that it wasn’t worth it.” She spoke of “riding a wave of ecstasy” until her menopause hit and declared, “that’s all over with, like all this work you’ve done, you’re back to square one.” Her recap of this loss was “a death beyond a death within a death.” Juxtaposing who she was before menopause with who she became post menopause clearly portrayed the drastic changes that had occurred for Susan Jane as well as the subsequent distress (see Nosek, 2012, for case study of Susan Jane’s experience).
The individual experiences of participants’ symptoms varied according to the circumstances and context of the women’s lives and encompassed interpersonal, social, and work situations. The consequences of symptoms manifested in a decreased quality of life for many of the women as they attempted to make sense of their embodied changes.
Discussion
This article focused on the specific contextual background of women’s experiences while adhering closely to the women’s narratives. The intact narratives reported in this study captured a rich life world perspective and facilitated the knowledge gained by closely examining the nuances and intricate web of midlife women’s symptom experiences attributed to menopause. Other findings from the original study have been reported elsewhere and demonstrate the use of multiple methods for data analysis (Nosek, 2007, 2012; Nosek et al., 2010); however, in this article, the narratives shared were mostly told as complete stories that warranted the use of Labov’s (1997) method. Nonnarrative segments were also incorporated (Gee, 1985, 1986) in findings shared by Susan Jane and Nancy that portrayed the effect of symptoms on their quality of life, and Candy as she spoke of her changes in mental state.
These findings demonstrated how the immediate world of the participants affected their distress, as well as how their symptom experiences affected their ability to interact with their immediate world. The temporal contexts of women’s lives became salient as their present situations arose from a comparison with past circumstances, and poised against future concerns. In previous studies, references to past are used generally from a life course perspective, where women’s stressful pasts are demonstrated to predict symptom experiences later in life (Kuh et al., 2002; Schmidt, Murphy, Haq, Rubinow, & Danaseau, 2004). However, they often imply that midlife challenges are just another crisis along the disruptive life trajectory of some women indicating an innate or learned inability to cope. Future is examined in a manner such as Reynolds’s (2000) study on catastrophizing where associations between distress and “despairing anticipations about the future” are found (p. 114). Using those frameworks, women are seen as inflating situations or lacking ability to control reactions to current circumstances. The stories told in this study portray women as having reasonable concerns for the future situated in socially and culturally shared values and life experiences. For example, the fact that Candy was experiencing symptoms much earlier than her peers most likely had contributed to her distress. Not only did she experience feeling “robbed of her youth,” but she may also have lacked a peer group to share with or gain support from.
Studies have examined other social factors of women’s distress and have found associations with social support, presence of teens in the house, marital satisfaction, and difficulties with family members (Avis et al., 2003; Chedraui, San Miguel, & Avila, 2009; Kuh et al., 2002; Price, Storey, & Lake, 2008; Schmidt et al., 2004). Avis and colleagues (2003) found that being married increased quality of life in midlife women across four ethnic groups. Many of the women’s narratives in this study involved partners. Martha’s marital status contributed to her experiences of distress mainly for fear of losing her partner due to her emotional instability and decreased libido. Conversely, Elizabeth’s decreased libido was not a problem for her because of her husband’s acceptance of it, which was “all that mattered.” Fay’s being partnered contributed to some of her distress because of the conflicting circumstances between their sexual needs. Hinchliff, Gott, and Ingleton (2010) conducted a qualitative analysis of women’s sexual relationships during menopause and demonstrated similar variations in women’s sexual experiences that were greatly dependent on the contextual tapestry that existed between the women and their sexual partners.
Some researchers have proposed that having multiple roles, including work outside the house, can buffer distressful menopausal experiences as they may increase women’s feelings of self-esteem and self-efficacy (Strauss, 2011). In this study, women either feared their symptoms would interfere in their ability to perform at work or work conditions exacerbated their difficulty in managing their symptoms.
Quality-of-life effects, commonly examined in studies of menopause, attempt to grasp the severity of symptom experience. However, the instruments used often fall short of unveiling the specifics of how the women’s lives are affected (Elavsky, 2009; Schneider, MacLennan, & Feeny, 2008). Utian (2005a) addressed how vasomotor symptoms can affect women’s quality of life, but added that the “effects are difficult to quantify because of the many factors that contribute to overall QOL satisfaction” (p. 3). Conversely, “many factors” of the participants’ lives in this report were illuminated via the rich stories that the women shared of their distressful experiences. Avis and colleagues (2009) reported that all menopausal symptoms examined in their study of midlife women were significantly positively related to reduced function on all five domains of a quality-of-life measurement. This is important to report, but again, their data founder to enlighten researchers and clinicians of any specific contextual details of the impact of symptoms on the women’s lives, as well as how the everyday worlds of the women contribute to the symptoms experienced.
Limitations
Interviewing partners and family members of women may have illuminated the extended impact of women’s distress. In addition, only heterosexual and able-bodied women participated. Experiences of lesbian and physically challenged women would have greatly enhanced the findings.
Conclusion
Experts in the field have recommended the exploration of the sociocultural elements of menopause experiences (Utian, 2005b; Woods & Mitchell, 2005). The results of this study revealed complex interpersonal and social elements of symptom experience during the menopause transition. Moreover, the framework and method used in this study afforded the rich examination of interactions between women’s experiences and their surroundings in a more informative manner. Qualitative data allow for a more in-depth view of participants’ lives, but more often than not, reports are given as a thematic analysis only, with very brief supportive excerpts. Keeping a narrative intact reveals much more of the intricacies of experiences, including the players involved, the everyday meaning persons place on these experiences, and the efforts involved in creating resolutions. The understanding gained from this narrative analysis of women’s experiences increases the awareness of a potentially misunderstood group of women.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was funded by a Betty Irene Moore Nursing Doctoral Scholarship.
Bios