
Abstract
Resilience is a multifaceted construct that refers to the positive adaptation of individuals, despite exposure to adversity. This study of resilience in older individuals who have experienced adversity was conducted to deepen the understanding of the factors that contribute to resilience in this population. This qualitative study used purposive and homogeneous sampling criteria to recruit nine participants above the age of 65 with a past history of childhood maltreatment who were judged by their health care professionals to be unusually resilient. Resilience was found to be highly evident in this sample, despite earlier trauma and the subsequent challenges of old age. The authors found active engagement in relationships and in valued activities to be the most often mentioned contributors to resilience in these older survivors of childhood maltreatment. These findings have important implications for public policy and social interventions to preserve the well-being of older individuals who have experienced adversity.
Introduction
Resilience, or the ability to maintain or regain mental health, despite significant adversity (Cicchetti & Garmezy, 1993), has thus far been studied primarily in children and adolescents. Many types of adversity can be experienced by children, including physical, emotional, and sexual abuse, as well as neglect and exposure to family violence. All of these types are subsumed under the general term of child maltreatment (CM). CM has been shown to be a significant health determinant, leading to increased mortality and morbidity, including physical health problems, mental disorders, poor academic performance, aggression, crime, suicidal behavior, and decreased quality of life (Gilbert et al., 2009). Most research conducted thus far on CM has been cross-sectional in nature or has had follow-up of only a few years after the time of CM. Little is known about the long-term effects of CM or the factors that contribute to resilience in later life in those with a history of CM.
The concept of resilience is not new, although there has been a recent burgeoning of research interest in this area. In fact, more than 85% of all research publications on resilience have appeared in the last decade (Hjemdal, 2007). Early research on resilience focused on the identification of particular qualities and personality traits, such as hardiness and self-efficacy, which help people to overcome adversity (Cicchetti & Garmezy, 1993). More recent research has focused on the process by which the qualities of resilience are acquired over time and on the natural fluctuations that occur across the life span. The latter may depend on the balance of stressors and protective, compensatory, or resilience factors. This recent research has led to a shift in the predominant view of resilience from that of an innate or inherited quality to one that is more dynamic, contextual, and acquired. A recent conference of resilience researchers defined resilience as “a dynamic process in which psychological, social, environmental, and biological factors interact to make an individual, at any stage of life, to develop, maintain or regain their mental health despite exposure to adversity” (PreVAiL, 2011).
The more recent conceptualizations of resilience view it as an interactive dynamic process that develops through a repetitive process of disruption and reintegration in response to adverse events (Richardson, 2002). Through this process, it is postulated that psychological protective factors that facilitate positive adaptation to subsequent adverse life events develop, thereby promoting positive mental health, which may wax and wane across the life span. Successful adaptation to later life requires this resilience to face the multiple and almost inevitable challenges of this life stage, such as those related to health, socioeconomic circumstances, relationships, and employment status.
Previous research suggests that many elderly people view themselves as having aged successfully, despite the presence of chronic disease and disability (Depp, Vahia, & Jeste, 2010). These findings suggest that resilience may persist or emerge in the elderly, despite the multiple stressors associated with illness and health limitations (Montross et al., 2006). With the demographic shift toward older age in developed countries, it becomes particularly important to understand those factors that contribute to successful aging. Those who have been exposed to early life adversity, such as CM, may have acquired resilience and/or may still be suffering from its sequelae in later life (Widom, Dumont, & Czaja, 2007), thereby affecting their adjustment to the losses of old age.
Successful Aging
The World Health Organization (WHO) describes active aging as “the process of optimizing opportunities for health, participation, and security in order to enhance quality of life as people age” (WHO, 2002, p. 12). This refers to the adaptive process that allows individuals to achieve their own life goals and to maintain competence as they age. The challenges of old age pass through what has been conceptualized as the “lens” (Hochhalter, Smith, & Ory, 2011) of an individual’s personal resources, values, and attitudes, all of which affect the outcome of adaptation. Successful aging may depend on the preservation of the “building blocks” of identity (Kaufman, 1986) as well as the capacity to adapt flexibly to the challenges that threaten competence, well-being, and social engagement.
The concepts of resiliency and survivorship have been used in understanding the successful recovery from traumatic events, but have not been widely explored in elderly survivors of CM. In one study of elderly Holocaust survivors, a paradigm shift was identified as these individuals aged, with their primary focus shifting from rebuilding their lives to maintaining their competence (Greene & Graham, 2009). Other quantitative studies in different populations of older people have identified characteristics that may contribute to resilience. These include sociodemographic factors (Beutel, Glaesmer, Decker, Fischbeck, & Brahler, 2009; Fiske, Wetherell, & Gatz, 2009), health and well-being (Reichstadt, Depp, Palinkas, Folsom, & Jeste, 2007; Wells 2009), positive attitudes (Lamond et al., 2008), self-esteem (Windle, Markland, & Woods, 2008), and a sense of mastery (Low, Keating, & Gao, 2009; Montross et al., 2006). Furthermore, embeddedness in a social community (Hildon, Montgomery, Blane, Wiggins, & Netuveli, 2010), religious affiliation (Costanzo, Ryff, & Singer, 2009; June, Segal, Coolidge, & Klebe, 2009), and the presence of supportive relationships (Beutel et al., 2009; Gergen, 2009) may contribute to resilience in older individuals.
Gender differences in resilience in the elderly have received only a small amount of research attention. A longitudinal study of Israeli Jews aged 75 to 94 found that men were more physically active, had better cognition, gave more help to children, relied less on paid caretakers, and attended synagogue more than women (Walter-Girtzburg, Shmotkin, Blumstein, & Shorek, 2005). However, it is not known if their lesser reliance on paid caregivers was a result of the care they received from their wives and daughters, which may have been less available to elderly women, many of whom are widows. In a later study of rural Americans aged 65 and older, women reported fewer health problems that interfered with daily functioning and were more likely than men to report that relationships, frame of mind, participation in activities and religion, and spiritual activities were important contributions to successful aging (Stark-Wroblewski, Edelbaum, & Bello, 2008).
Current Study
CM has been associated with a wide range of subsequent psychological disturbances and psychiatric disorders in childhood. These include attention deficit hyperactivity disorder, oppositional disorder, anxiety, mood, and substance use disorders, and disturbances in affect regulation and attachment (Affifi, Boman, Fleisher, & Sareen, 2009; Affifi et al., 2008; Cicchetti & Toth, 2005; Fergusson, Boden, & Horwood, 2008; Gilbert et al., 2009). CM is also associated with an increased risk in adulthood of depression, anxiety, substance abuse, personality disorders, and antisocial behavior (Johnson et al., 2001; MacMillan et al., 2001; Widom et al., 2007). In adults who experienced CM, resilience was found in those who reported better perceived parental care, adolescent peer relationships, and quality of adult love relationships (Collishaw et al., 2007).
Resilience research has the potential to elucidate the mechanisms that contribute to successful adaptation, psychological growth, and adverse mental health outcomes. Some research has been conducted regarding the effects of CM in childhood, but little has been known about their long-term consequences in older adults. In particular, little is known about the characteristics of older adults who have achieved and maintained resilience, despite exposure to CM. Such information may be of value to educators, health care providers, and policy makers to promote resilience across the life span. Greater understanding of individual and contextual risk factors, and of the social determinants of health may lead to more effective prevention and treatment interventions.
The present study will explore resilience in older individuals who have coped well with previous trauma, specifically CM, to gain an understanding of the factors contributing to their resilience. Focusing on individuals with past adversity who have demonstrated resilience may enhance our understanding of this phenomenon and how it is altered by the transformations of old age.
Method
Research Design
A qualitative research design was employed to explore what factors or circumstances throughout their lives are considered by older individuals, who had coped successfully with prior CM, to have contributed to their resilience. A qualitative approach was considered to be most useful in this context to understand the experience and perceptions of such individuals with regard to aging, and the factors they attributed to their resiliency. Interview methodology of this kind generates undiluted, in-depth narratives (McKague & Verhoef, 2003), which may reveal novel information about the study variables, which could not be elicited by predetermined qualitative measures. Interviews also allow researchers to probe for clarifications on unique perspectives and experiences on potentially sensitive issues. All interviews were digitally recorded and transcribed. This project received ethics approval from the University Health Network Research Ethics Board (Toronto, Ontario, Canada).
Research Methods
Purposive and homogeneous sampling criteria were used to recruit men and women above the age of 65 living in Toronto, Canada, with a past history of CM, and who were judged by their health care professionals to be remarkably resilient. As the frequency of exposure to CM is comparable in both sexes, (Canadian Centre for Justice Statistics, 2007), we sought to include men and women in our sample. Exclusion criteria included a history of any psychiatric illness. Ten health care workers (physicians and social workers) at a large university teaching hospital were approached to recommend patients in their practice who met study criteria and who could be invited to participate. Most elderly people have fairly regular contact with the health care system and have built relationships with their health care providers over many years. The health care workers may be aware of their past history of abuse and, being aware of their physical and mental functioning, could assess their patients’ resilience. Although resilience has been defined differently throughout the literature, this article adopted the definition of resilience suggested by Cicchetti and Garmezy (1993) as positive adaptation, despite exposure to adversity.
Health care professionals contacted potential participants to request participation in the study and their willingness to allow their contact information to be shared with the study investigator. Recruitment was continued until saturation of the themes was achieved. In qualitative data, it has been noted that “five to eight data sources of sampling units will often suffice for a homogenous sample” (Kuzel, 1999, p. 42).
All participants who granted permission to their health care professional to be identified were contacted by the first author and explained the purpose, methodology, and requirements of the study. Participants provided written, informed consent to participate in the study and to audiotape the interview. All potential participants who agreed to be contacted regarding participation in the study provided such consent and completed the interviews.
Measurement Tools
In-depth, semistructured interviews of 60 to 90 min in duration focused on the meaning, perception, and experience of resilience and resilient processes throughout their lives following exposure to CM. Specific strategies were used to enhance the rigor of data collection, including the use of an interview guide with probes to elucidate emerging themes and concepts, digital recording, and field notes.
Analysis
Qualitative data were organized and analyzed in iterative phases of discovery, coding, and discounting using NVivo. The analytic technique of constant comparison was applied within and between interviews to refine the analysis (Taylor & Bogdan, 1998). This technique involves open coding of transcripts and field notes and grouping segments of text into categories and subcategories.
Statements by participants were compared for similarities under a theme and/or a concept within and between interviews. Constant comparison led to collapse and/or expansion of the earlier categories. Analytic induction through an emphasis on the search for negative cases allowed for testing of emergent hypotheses. This methodology enhanced the transferability of the findings, despite the small number of studied cases, and helped to move the analysis from description to interpretation.
Results
A total of five women and four men were recruited for this study, which allowed for a clear saturation level of the themes to emerge. The demographics of the study population are presented in Table 1, with pseudonyms used to refer to the participants in the remainder of this article.
Sample Characteristics
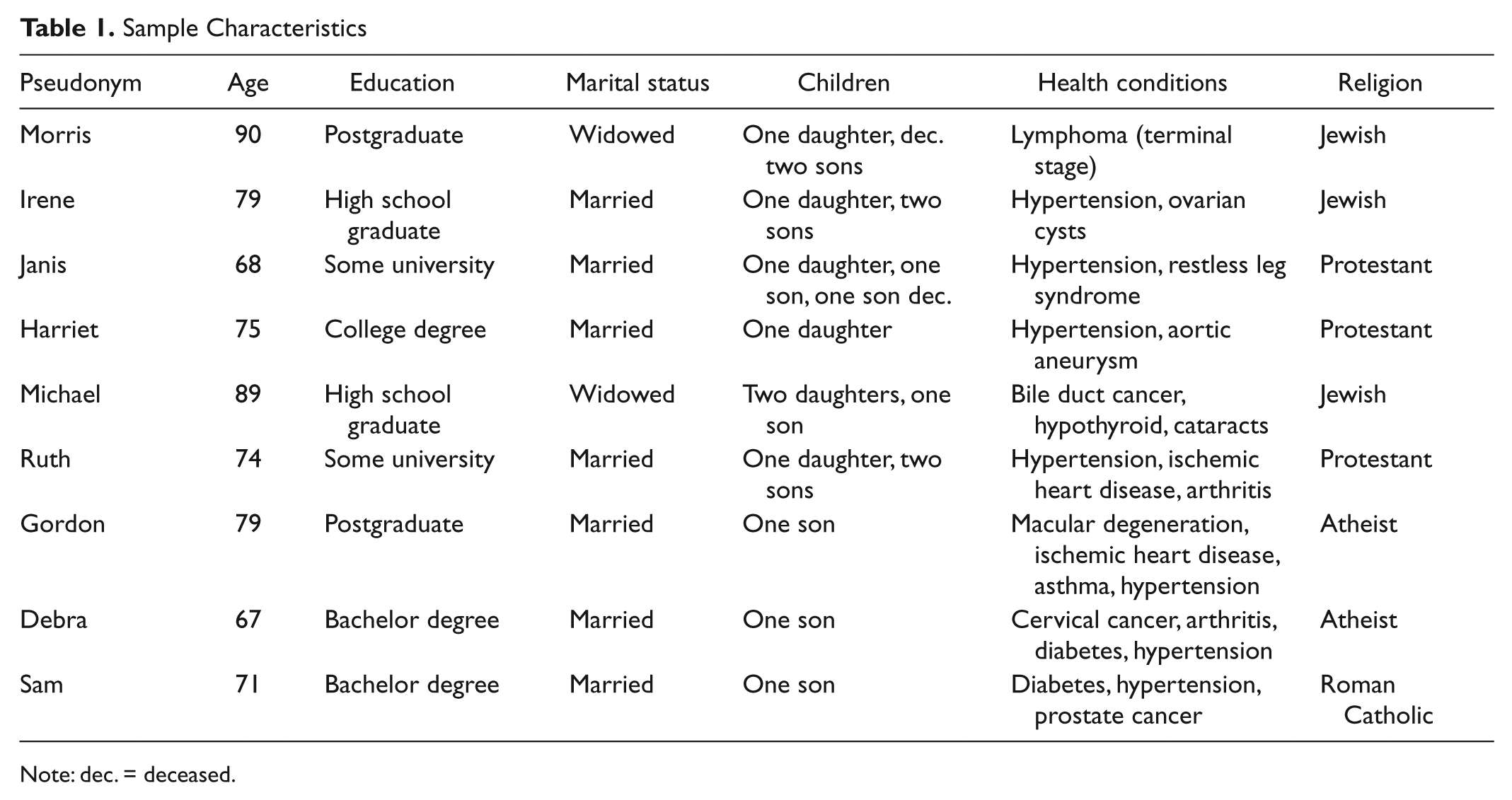
Note: dec. = deceased.
The interviews elicited rich histories of the lives of nine remarkable individuals who have successfully overcome CM and flourished in old age. These individuals varied in age (ranging from 67 to 90 years old), education level, and religion. They all experienced CM, although it varied in nature and included physical abuse, emotional abuse, neglect, and exposure to violence between their parents. None of the respondents reported sexual abuse. In addition, more than half of the respondents shared the experience of living through hardships associated with World War II, in which they lost loved ones, experienced scarcity and hunger, and lived in fear for their safety. This additional trauma, which we had not anticipated on recruitment, added to the remarkable history of this group.
Each participant became emotionally distraught when describing his or her CM maltreatment and how he or she believed it affected him or her. However, they were all able to reflect on their childhood with insight and describe how they traversed and survived this difficult period. Participants retained a sense of perspective and even humor about their past and present situations. They also often displayed playfulness in their responses to questions. When Michael, who had advanced lymphoma, was asked whether he found it helpful to make future plans, he chuckled and said, “I don’t plan anymore, they’re planning for me!”
This article will focus on the most prominent contributors to resilience that were identified as these individuals moved through the life cycle to old age. Certain gender differences were notable, in that the women emphasized relationships and social interactions, whereas the men tended to place greater emphasis on solitary activities. The participants themselves also commented on the differences in resilience that they perceived between men and women. Janis said that she believed that, “probably the majority of women look to other women for support, whereas men are not supposed to look outside for help.” Sam seemed to agree with Janis’s line of thinking when he said:
Women are too emotional. Gets ’em into trouble, like my wife. Too much talk, talk, talk. Guys play sports or take a hike, walk the dog. It’s better. Action oriented.
Despite some gender differences, respondents identified six broad themes as major contributors to resilience in the face of prior trauma and in coping with the new challenges of old age: social support, psychological attributes, financial security, health, spirituality, and engagement. Most participants referred to these themes in their responses, but the theme of engagement in their present life was most consistently identified as important by the study participants.
All participants reported the experience of meaningful social support during their childhood and in their adult life, even during the period of CM. The theme of social support emerged in their description of their relationships with their own parents, romantic relationships and partnerships, teachers, social networks and interactions, community integration, and in a sense of belonging. Many described childhood support as molding their sense of resilience in adulthood. Harriet, whose mother died when she was aged 4, describes the perceived effect of her mother’s nurturing:
I think the reason that I survived and that I seem to be comparatively normal and stable and I managed to not have any mental problems and to try and deal with my background is that my mother, she was an orphan herself, was very beautiful and a very loving mother. She always, apparently from what I hear, took wonderful care of us. She sewed clothes for us and knitted and was very, very attentive, so I think being loved like that until the age of about three and a half was a tremendous thing. I think it’s something that . . . if a child had this at a young age, it can carry them through life.
Because people experience more losses of loved ones as they age, the sources of support can take different forms. Sam identified his dogs as his major source of comfort and resilience:
I’ve always had a dog, usually a German shepherd, ever since I was a kid. I talk to my dog and he, or sometimes it was a she, always understood. You know they love you no matter what, and that counts for a lot. They sense feelings, know when you’re upset and comfort you. You know I have a wife who is supportive, but not as supportive as my dog—don’t tell her that!
Many of the participants described psychological attributes that they believed allowed them to be more resilient than many of their peers, as they entered old age. These included adaptive coping styles, inner strength, a positive attitude, self-esteem, optimism, and acceptance of aging. Harriet described the importance of inner strength and being able to maintain a satisfying “inner life.” She described what resilience meant and continues to mean to her:
I think what resilience means to me is inner strength and the ability to stand on your own two feet and deal with things, not to lean on other people for support all the time, not to be helpless. I’ve always been very independent, I do all my own gardening, my husband is very busy, so I sort of do all the mending and repair things and fix things. I do the sort of man’s work around the house and I’m a woman, so I am sort of independent.
Financial security was vital for many of the participants. For example, Ruth, a housewife turned medical historian in her later life, discussed how her financial security allows her to concentrate her energies in areas that give her personal satisfaction. For the past 8 years, Ruth had been writing a medical biography, which involved extensive travel. Referring to the support that her husband is able to provide, she explained,
As long as we keep putting one foot in front of the other and we have enough money to pay the mortgage, we (can) be supportive of one another’s projects. I don’t mean million dollar projects, but the fact is that it cost money to do the book I did because I had to go to Africa.
The participants in this study were still relatively healthy and were able to successfully carry out most of their activities of daily living without assistance. However, many of the participants expressed wariness regarding the possibility of future physical limitations. Gordon, a retired physician who experienced abandonment as a child, described his concerns as follows:
Well my eyesight is going and that worries me because so many of the things I enjoy doing I need my eyes for and I’ve only got one of them now. So I do worry about if the other one goes. I go out of my way to be reasonably good with electronic gadgets and things, so that I would be able to move onto portable books and things like this . . . But that scares me. I would find it difficult if I really lose my eyesight. And, you know, my eye doctors can’t tell me.
Some of the other participants had already experienced significant health challenges. However, many explained that this gave them a greater appreciation for the time they have left. Harriet had already suffered from breast cancer and, more recently, an acute dissecting aortic aneurysm. She described her feelings surrounding these events:
Miraculously, absolutely miraculously, I survived with all my mental faculties intact . . . And I’m at a pretty wonderful stage in my life and I’m so thankful for every day that I have with my husband and children and grandchildren . . . I have great hope and faith that I will live for another 5 or more years, so I still have great hope for the future.
The importance of organized religion was dismissed by many of the participants. However, the idea of spirituality and maintaining a belief in a higher power was identified as important for some. Harriet discussed the importance of faith in maintaining resilience as she aged: “I think I’ve often prayed and found my prayers were answered, which is amazing.” Others, who conveyed a more ambiguous view of the form that faith should take, still found it valuable. When asked whether faith helped him cope, Michael, a Holocaust survivor who spent his teenage years in Auschwitz, replied, “Yes, you have to believe in something. Whether it’s true or not. If you don’t believe in anything, you’re a lost person. You have to believe in something.”
Engagement in relationships and valued activities was a theme that most strongly emerged throughout the interviews as the most salient factor in maintaining and promoting resilience in this group of individuals. Engagement in meaningful or challenging activities was emphasized by all of the participants as vital to their sense of resilience as they aged. As this theme has received little previous attention in the literature, we explored it in further detail in our analysis. This theme was expanded and reorganized as the interviews progressed and the subthemes began to take form. Engagement was conceptualized through the following five domains: (a) engagement in valued activities, (b) generative identity, (c) maintaining competence, (d) personal life investment, and (e) desire to learn.
Engagement in Valued Activities
As they entered old age, many individuals struggled with the loss of loved ones, most often friends or a partner. One participant, Janis, who was emotionally abused and abandoned by her mother as a child, lost a much loved son when she was middle-aged. She had built a new life with her husband and raised her children, but was devastated when one of her sons died tragically as a young adult in a hit-and-run accident caused by a drunk driver. Janis found that engagement in valued activities was a vital way for her to channel her emotions into energy that could benefit others and maintain her resilience in the face of this new traumatic experience. She talked about many of the resilient women whom she met at Mothers Against Drunk Driving (MADD), but it was apparent that Janis is most certainly one of these women herself:
Well I’ve been volunteering for MADD for many years and if you want a group of people who are resilient, there are just so many who have had to deal with losing family members and doing something about it. I know a lot of people who have gone on to do really amazing things after losing a child. You know, like I have, become involved in MADD.
Generative Identity
Debra was a successful health administrator throughout her adult life. She talked about how success in her career played a large role in her resilience throughout her adult life. As she has grown older, however, she discussed how she derived significant satisfaction and strength from mentoring others in her field, particularly women:
I was very good at what I did and became internationally known. I felt I was really contributing and people liked me. Now that I’m pretty much retired, I still keep active in my profession—it feels good. I sit on advisory boards, advise junior people and research widely in my field. I enjoy seeing so many successful woman as it was very sexist in my day. We prevailed against tremendous odds.
Janis also talked about how it was important for her own resilience to be able to continue to teach others about issues to which she has dedicated much of her adult life. She spent much of her working life on advocacy surrounding drunk driving, and described how she believes it continues to help her deal with tragedies in her past and to feel engaged in the future. She explains, “I go and talk to high school students. It’s a tough thing to do, but it’s very cathartic, being able to do that.”
Maintaining Competence
Michael arrived in Canada penniless with his young family. He talked about the pressures he felt to start working immediately and earn a living. He had spent some time working with a tailor as an afterschool job when he lived in Eastern Europe, so he decided to open up a tailoring business. He described the importance that maintaining his competence has had for his happiness and resilience as he aged. Like many of the participants, he has faced some limitations in his functioning as he has grown older, but has learned to adapt to many of these challenges. To this point, Michael explained,
I was in the tailoring business and, not to brag about it, but I had a partner and we were the best tailors in town. I couldn’t make a whole garment anymore, but I can do an alteration, shorten a pair of pants or put on a button. Now I do my profession as a hobby.
Michael also stressed the importance of knowing when to ask for help as he aged and to continue to be able to care for himself. He said, “I have confidence in myself. If I get help, it’s even better, but if not, I have confidence that I can help myself.” He talked about how it was important for him to continue living in his house and to take care of maintenance work around the house and the garden, as long as he is able to do so.
Personal Life Investment
Irene is a Jewish Polish woman who survived the Holocaust by escaping to Russia with her family. She immigrated to North America in her early 20s with her husband and twin infant sons. She described the determination that she and her husband had to carve out a life for themselves and for their children, which they were deprived of in Europe. This became a major goal for Irene through much of her adult life. She explained,
I look now at what we went through and I can’t believe we survived. I worked hard here, plus my husband worked, so that my kids have a good education, so that they have what we missed out on.
When Irene was in her 50s, her husband suffered a major stroke. Caring for her husband and maintaining their home became a personal life investment for Irene that gave her a sense of meaning and purpose throughout her old age, even after her children left the home. She boasted that when she goes to her family doctor, he says to her, “Irene, you’re amazing. If not for you, your husband wouldn’t be here anymore.” “It means a lot to me,” she explained.
Gordon discussed how it has been important to develop himself in different and more creative ways since his retirement. He led a busy practice as a physician and now, in his later life, has spent time on other hobbies and personal passions. He described how setting firm goals for himself has helped him to remain resilient as he aged:
You know, whatever, whether it’s studying medicine, or whether it’s writing a book, or building a house, or at the moment, doing my family tree and learning Spanish. I like setting myself a fairly concrete kind of goal and I’m a bit rigid about it.
Desire to Learn
Morris worked as a medical sociologist and a professor for many years, and described how he found his continued involvement in academic work to be very therapeutic. He discussed how his early life was profoundly transformed by his access to books and institutions of higher learning:
At the end of the war, I was very fortunate in getting access to university, which quite surprised me. So when I found myself in university, it opened up a whole world . . . it was really quite a different world. It was a world of learning and scholarship and I flourished. I don’t think I would have done as well if I hadn’t gone to university . . . It gave me new perspectives, new opportunities, new friendships, access to values and ideas that had never occurred to me.
Morris talked at length about his career as a professor and his research. When asked about how his retirement from university life had affected him, he exclaimed, “No, I’m really blessed because now I don’t have to mark papers!” He explained how he still maintained a voracious appetite for learning and scholarship and that this has kept him fulfilled throughout his old age. He found that his desire to learn continued to give him an outlet for intellectual development, despite the challenges inherent in growing older:
I wake up in the morning and feel a great joy that I can spend a whole day on whatever the project is that I’m working on. I feel incredibly fortunate. My wife died about 14 years ago of cancer, but before she died, she said something interesting that surprised me. She said she was glad she was going first. She didn’t really want to be a widow for years and years and years. And I thought, that’s very interesting. The notion of ending up as a widow was a bother to her. She was a Scot and a very independent woman. Now I didn’t feel that because I still have a tremendous joy in getting up in the morning and reading and arguing and writing. If you had said to me 50 years ago that I won’t have to go to work, I can read any book I want, I can get any document I want from the library, I would have thought that was absolutely crazy. But that’s what I do. And I can’t tell you what a tremendous joy that is.
Discussion
Although most of the previous resilience literature has focused on children and adolescents, our findings demonstrate that resilience may be very evident in later life, despite earlier life trauma and the subsequent challenges of old age. The positive outlook, strong will, and effective coping abilities of these individuals were pervasive throughout the interviews.
It is clear from the resilience literature and the data of our study that psychological factors, economic stability, and social support play major roles in enhancing resilience in older individuals. All of our participants reported significant social support in their developmental years that may have contributed to their self-esteem and capacity for engagement in later life. Although all valued the support of others, they regarded their own competence and mastery as central to their resilience. Religion or spirituality also was considered by some but not all of the participants in this study to play an important role in their resilience.
What stood out in our interviews with these exceptionally resilient individuals was the importance that they gave to their intellectual life and valued activities, many of which related to their previous work and interests. Their desire to learn and potential for growth remained very strong and integral to their resilience as they aged. They were fully engaged in social, community, and intellectual life and remained psychologically optimistic, despite sometimes life-threatening medical problems. These participants responded to their difficult childhoods of abuse, maltreatment, and deprivation, and to the subsequent challenges inherent in old age by engaging in life more fully and pursuing goals, hobbies, and activities.
These findings reinforce and add to earlier work on resilience in the elderly and are consistent with Erikson’s suggestion that continuing psychological development across the life span provides the basis for a resilient self and the accrual of wisdom by later life (Erikson, 1963). He also emphasized “generativity” or a concern for establishing and guiding the next generation as a central step in the successful transition in life to the final stage of integrity, consistent with the observations of several of our participants. Masten (1994) suggested that resilience be viewed as the ability to maintain competence across the life span.
We found that specific psychological characteristics, particularly those associated with self-reliance and the flexible use of supportive relationships, were emphasized by the participants in our study as contributing to their resilience. These findings are consistent with an empirical analysis of a large representative sample of older individuals in the United Kingdom. That study led to the elucidation of a higher order model that incorporates interpersonal control, self-esteem, and personal competence as most useful in understanding psychological resilience in old age (Windle et al., 2008). More recently, a study of elderly Holocaust survivors found that taking up a purpose and maintaining competence was essential to resilience in old age in individuals who had earlier experienced adversity (Greene & Graham, 2009).
Limitations
There are some limitations to our study. The sample, which consisted of middle- to upper income Caucasians of European origin who were all recruited from a university teaching hospital in a large urban center, is not fully representative of the population of survivors of CM. Therefore, our findings may not be generalizable to other racial or cultural groups, or other settings. The sample was specifically selected for “remarkable resilience” and thus may not be representative of resilience in the general population of older individuals who have been exposed to CM.
Conclusion
Our findings point to the importance of inner strength, social relatedness, and the ongoing motivation to engage and to learn as important contributors to resilience. Supporting these qualities in elderly individuals in the community may help to bolster their resilience and capacity to function autonomously. Retirement homes, nursing homes, and community centers could help their clients flourish or at least maintain their functioning by supporting their capacity for independent functioning and by promoting creative engagement in valued activities. These activities not only reflect resilience, but also reinforce it socially, psychologically, and physically. Creative expression promotes heightened sense of personal control, and encourages individual expression as well as social connectedness. It may even promote the preservation of cognitive functioning (McFadden & Basting, 2010).
The “paradox of well-being,” in which elderly individuals feel satisfaction with their lives, despite the loss of loved ones, the discomforts of illness, and the growing limitations in physical functioning, was elegantly demonstrated by the participants in this study. Their perspectives and insights about their experience with successful aging are inspiring and encourage us to consider whether the possibilities and benefits from creative engagement in older age can contribute to a shift in our understanding and expectations of individuals at this life stage.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article.