
Abstract
Cholesterol Granulomas of the Maxillary Sinus, considered an unusual presentation at this anatomical site. Over last 2 decades, only few cases are reported in the literature (English) and no available comprehensive reviews or studies on this entity. Herein in this article we present a comprehensive literature review of the available reports of 16 cases along with reporting a new case which we managed, aided with its histopathological pictures. This review article can be a reference for practitioners in the field of otorhinolaryngology who may encounter these cases. Also, it attracts the attention to consider this pathology among the differential diagnoses of nasal masses. Moreover, including a described pathological imaging may help young pathologist to identify this pathology.
Introduction
Cholesterol Granulomas are usually seen within the petrous apex and middle ear with rare occurrence within the maxillary sinus. Both clinically and radiologically they share similarities with Maxillary Sinusitis. Histopathologically, they represent an inflammatory process with foreign body giant cell reaction accompanied with cholesterol cleft formation. In this case report, the authors present a middle-aged female patient presenting with Cholesterol Granuloma in the Maxillary Sinus with a comprehensive review of all reported cases in the literature. This review may represent a reference for clinician to approach these cases.
Case Report
A 58-year old Saudi female presented to the clinic for her routine follow-up appointment. The patient possessed a medical history of Bronchial Asthma and Chronic Rhinosinusitis with nasal polyps, for which she underwent Functional Endoscopic Sinus Surgery (FESS) on three separate occasions, the last of which was 7 years prior to the time of her current visit to the clinic. She had been prescribed Pulmicort nasal irrigations.
Her chief complaint was a progressive left nasal obstruction and a noticeable mass in the left nostril over a duration of 2 months, which was associated with nasal discharge, facial fullness, and hyposmia.
On examination there was a Grade IV Nasal polyp in the left nasal cavity, while the right nasal cavity was patent and the sinuses were clear. On further advancement of the nasal endoscope within the left nasal cavity, between the polyp and the septum, clear ethmoid and sphenoid sinuses were seen, and it was determined that the polyp was originating out of the left maxillary sinus.
The treatment plan comprised of the excision of the polyp in entirety, in order to regain patency of the nasal airway. During the polypectomy under local anesthesia, a granulation tissue was found at the attachment of the polyp at the level of the Natural Ostium. The polyp along with the granulation tissue was completely removed and sent for histopathological assessment. Interestingly, the results showed an inflamed and ulcerated benign polyp with focal granulation tissue formation along with foreign body giant cell reaction around cholesterol clefts (Figure 1). This established the definitive diagnosis of Cholesterol Granuloma of the left Maxillary Sinus. Based on this finding, a Computed Tomography (CT) scan of the paranasal sinuses was requested, which revealed mucosal thickening of only the maxillary sinuses and ruled out any residual lesion or bony destruction (Figure 2).

Histopathological section shows cholesterol clefts surrounded by multinucleated giant cells (hematoxylin and eosin stain x20).
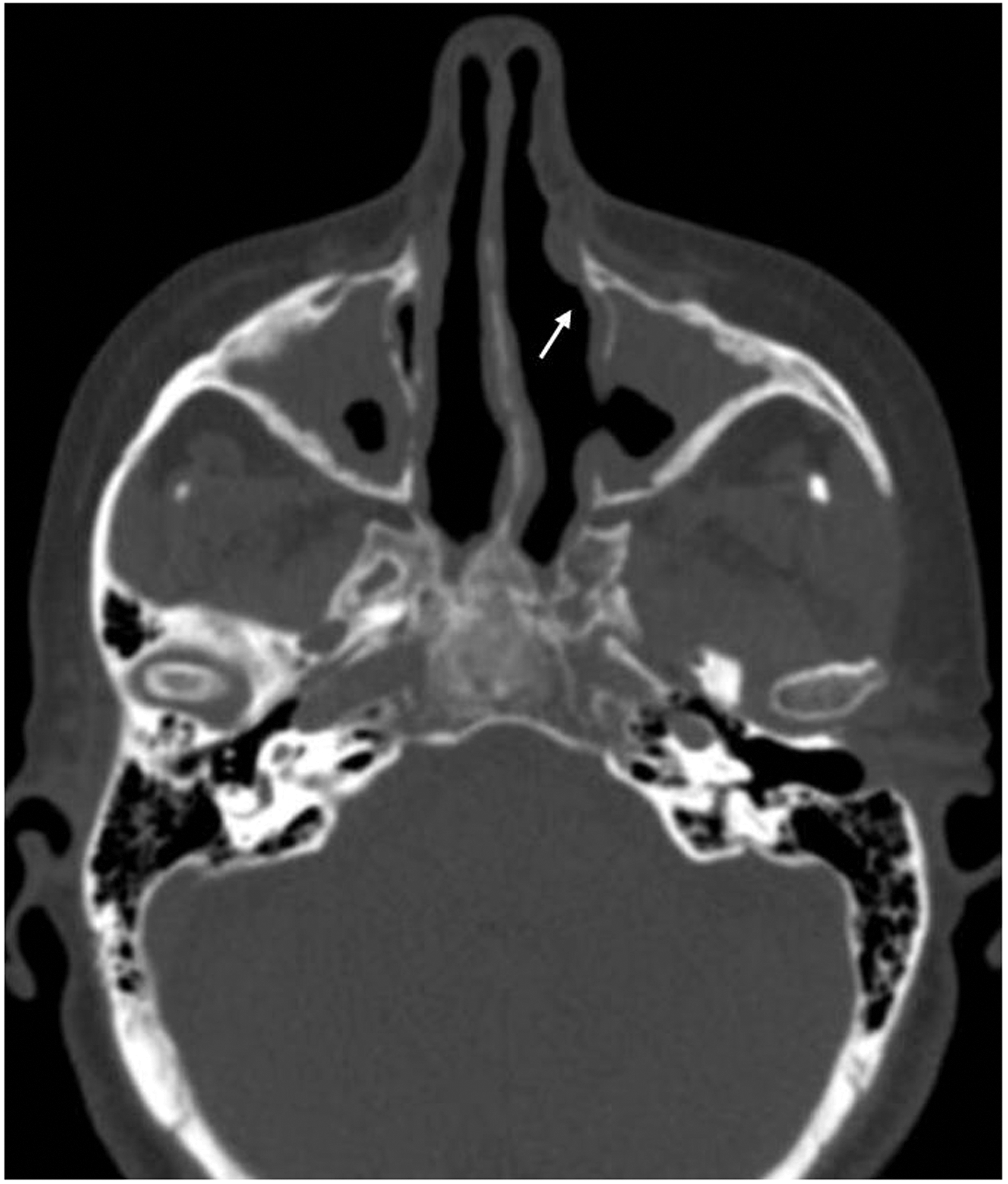
Paranasal sinus Computed Tomography coronal image shows operated maxillary sinuses with edematous mucosa corresponding to the clinical diagnosis with no erosion of maxillary sinus wall. The granuloma was removed from the attachment of the uncinate process at the level of the natural ostium, possibly related to the nasolacrimal duct (arrow).
The patient was recalled for 3 subsequent visits over a span of 6 months and was deemed to be doing very well with no recurrence of the granuloma or the polyp.
Literature Search Strategy
A comprehensive literature search including PubMed, EMBASE, and the Cochrane Library was conducted. The electronic database search combined disease-specific terms (Cholesterol Granulomas) with specific terms (maxillary sinus) with adjunct-specific terms (post-operative). Relevant articles and abstracts were selected and reviewed. Reference lists from these sources and recent review articles were searched for additional publications. All studies written in the English language were considered for inclusion.
Discussion
Cholesterol Granuloma of the Maxillary Sinus was first described by Graham and Micheal in 1978.1,2 It’s considered an unusual presentation at this anatomical site. Only few cases being well reported in the literature (English) and no available studies or comprehensive review articles on this entity (see Table 1).
Literature Review for Cholesterol Granuloma in Maxillary Sinus (2001–2019).
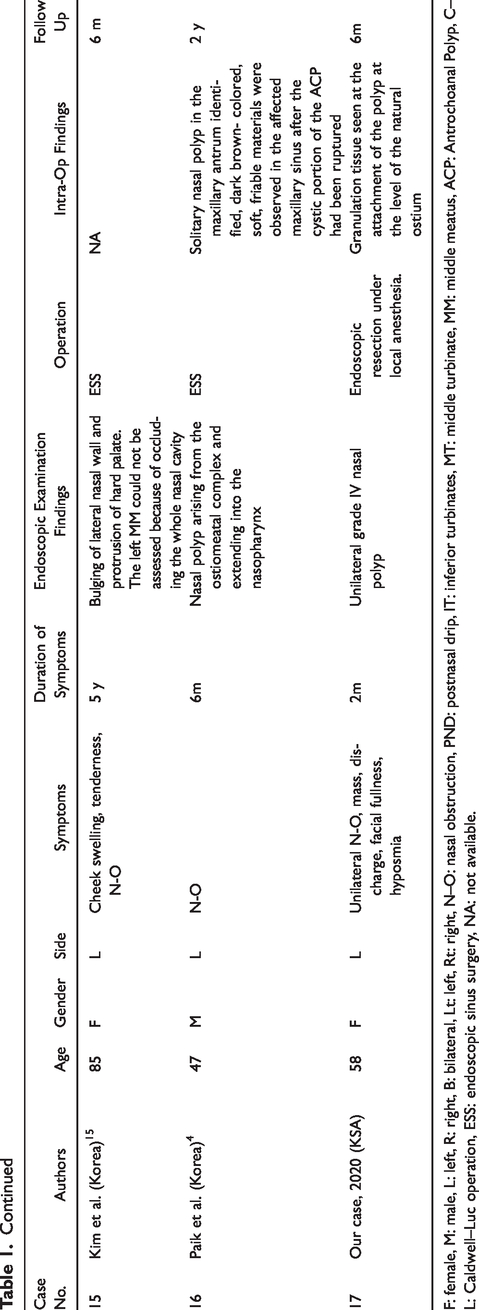
F: female, M: male, L: left, R: right, B: bilateral, Lt: left, Rt: right, N–O: nasal obstruction, PND: postnasal drip, IT: inferior turbinates, MT: middle turbinate, MM: middle meatus, ACP: Antrochoanal Polyp, C–L: Caldwell–Luc operation, ESS: endoscopic sinus surgery, NA: not available.
Patients with Cholesterol Granuloma are usually middle-age males presenting with the complaints of unilateral nasal obstruction, anterior nasal discharge, and pain. 3 Due to the rarity of Sinonasal Cholesterol Granuloma in the literature, it is suggested that the pathophysiology is similar to the one usually found in temporal bone, and is the granulomatous reaction to cholesterol crystals being formed from the outer membrane of erythrocytes, wherein the cholesterol forms a crystalline precipitate which accumulates in the sinus and subsequently initiates the reaction of macrophages and leukocytes.4,5
The obstruction of the sinus is due to any pathology that leads to hemorrhage, poor aeration, and decreased lymphatic drainage.1,4,6 Direct trauma or surgery might account for the initial insult, resulting in a Cholesterol Granuloma forming in the sinus. 2
During radiological examination, it frequently appears as a cystic mass and sinus opacification on a Computed Tomography Scan. 2 The presence of a unilateral calcification in the maxillary sinus on the CT scan pre-operatively, should raise a suspicion of the presence of Cholesterol Granuloma, which can thereafter be confirmed by the histopathological interpretation postoperatively. 4
The management of such lesions is similar to other isolated maxillary sinus masses, either open by Caldwell-Luc or via an endoscopic approach. With the latest advancements in endoscopic instruments and different scope angles, a complete removal of such masses can be carried out endoscopically. 3
A literature review was performed for all reported maxillary sinus CG cases (2001-2019) and is summarized along with our case in Table 1. This was done to identify the age, gender, presenting symptoms, duration of symptoms, endoscopic findings, surgical procedures, intraoperative findings, and follow-up for recurrence. Accordingly, it was found that the age of these patients ranged between 22 to 85 year (mean of 53.5 years) and there was no significant difference for gender predominance; males (9/17) compared to females (8/17). Regarding laterality, it was equally seen on both the right and left (7/17); few recognized to exist bilaterally (3/17).
Majority of patients were presenting with nasal obstruction, headache, or rhinorrhea, and painful maxillary swelling was the presenting symptoms in three cases.2,5,15 An episode of yellowish rhinorrhea that was confirmed with endoscopic examination was seen in one case. 10 Duration of symptoms ranged between 1 month to 5 years. Endoscopic examination wasn’t performed in all the cases; those which did reported either nasal polyp or obstructed middle meatus.
It is well-established that surgery is the appropriate treatment for CG of the maxillary sinus and, as mentioned earlier, it can be done by the older Caldwell–Luc approach or the more recent endoscopic sinus surgery, performed in 6 and 8 cases respectively from our literature search.
With regards to the prognosis for all 17 patients, with available data and follow-up periods varying from 2 months to 76 months, there was no recurrence at all, thereby requiring no further intervention.
In our case, the interesting and distinctive finding was the rapid progression of the symptoms over a short period of only 2 months. The background of multiple sinus surgeries was exclusive for our case and it was not mentioned clearly in the literature as being a possible cause for the formation of this granuloma. It has, however, been proposed that one of the pathogenesis is hemorrhage and subsequent hemolysis along with accumulation of cholesterol granules 6 which could be linked with surgical trauma. It is worthy of note that in our case the duration between the presentation of the granuloma and the prior surgery was 7 years. This, along with the short course of symptoms, can be indicative of another etiology, possibly an acute sinusitis.
The management was optimal with the first complete resection of the polyp along with granulation tissue under local anesthesia and yielded no residual at the time or recurrence during a six-month follow-up.
In conclusion, we presented the first case in our region and an updated comprehensive literature review for CG of maxillary sinus which is considered a rare entity. Furthermore, we recommend that CG should be listed as one of the differential diagnosis of sinonasal masses, to be removed surgically and investigated histologically.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by our institutional review board.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.