
Abstract
Significance Statement: Pregnancy-related giant nasal masses often present a diagnostic challenge and clinical dilemma due to the obvious restrictions in utilizing imaging and general anesthesia during pregnancy. Therefore, we highlight the importance of clinical judgment, especially during pregnancy, and should not disregard certain clinical cues. In addition, we recommend an in-office polypectomy for giant nasal polyps worsening during pregnancy and nasal steroids to optimize their quality of life while avoiding systemic medications or further interventions.
A 36-year-old, 16 weeks pregnant woman with an unremarkable medical and surgical history was referred to the otolaryngology service from the emergency room presenting with a large, fast-growing left sided nasal mass within 4 d. It was accompanied by bilateral nasal obstruction, hyposmia, and facial pressure. She also reported intermittent mild epistaxis that spontaneously ceased. She also had a history of upper respiratory tract infection 1 week prior to her presentation to the emergency department. The patient did not report any visual or neurological symptoms. She had a family history similar to that of her father, who had extensive nasal polyposis. Interestingly, the patient had a similar picture of the nasal mass but smaller in size during her first pregnancy, which regressed spontaneously after delivery.
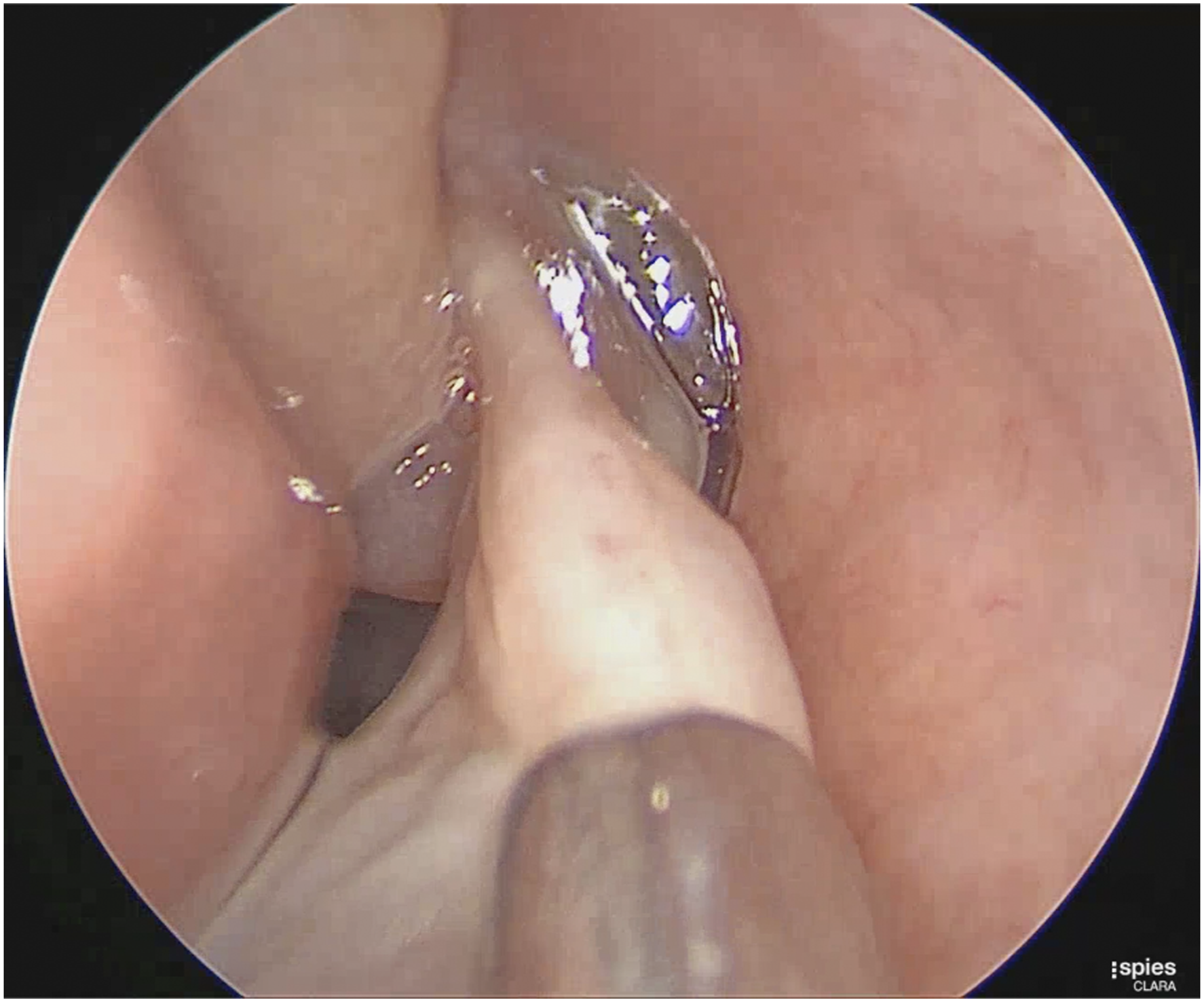
Subsequently, she underwent a complete examination with bilateral inspection of the nostrils, which revealed a left nasal mass extruding from the nostril with hyperemic features and purulent discharge. In addition, the mass was painless to touch and reached the vermilion border of the upper lip (Figure 1). The contralateral nasal cavity also showed a nasal mass at the tip of the nostril that seemed polypoidal in context, was pale in color, and was accompanied by mucoid non-purulent discharge. Endoscopic examination revealed a giant left nasal mass that appeared to originate from the middle meatus, with a high septal deviation to the left side of the nasal cavity. A polypoidal middle turbinate was also observed (Figures 2 and 3). The most likely clinical diagnosis was that of nasal polyps but a synchronous lobular capillary hemangioma or other neoplasms cannot be excluded. On complete examination, a left hyperemic nasal mass extruding from the left nostril with evident purulent secretions is observed. An endoscopic examination reveals a left nasal polyp originating from the middle meatus with high septal deviation to the left side and polypoidal middle turbinate. An endoscopic examination reveals a patent airway and nasopharynx in the left nasal cavity post polypectomy.
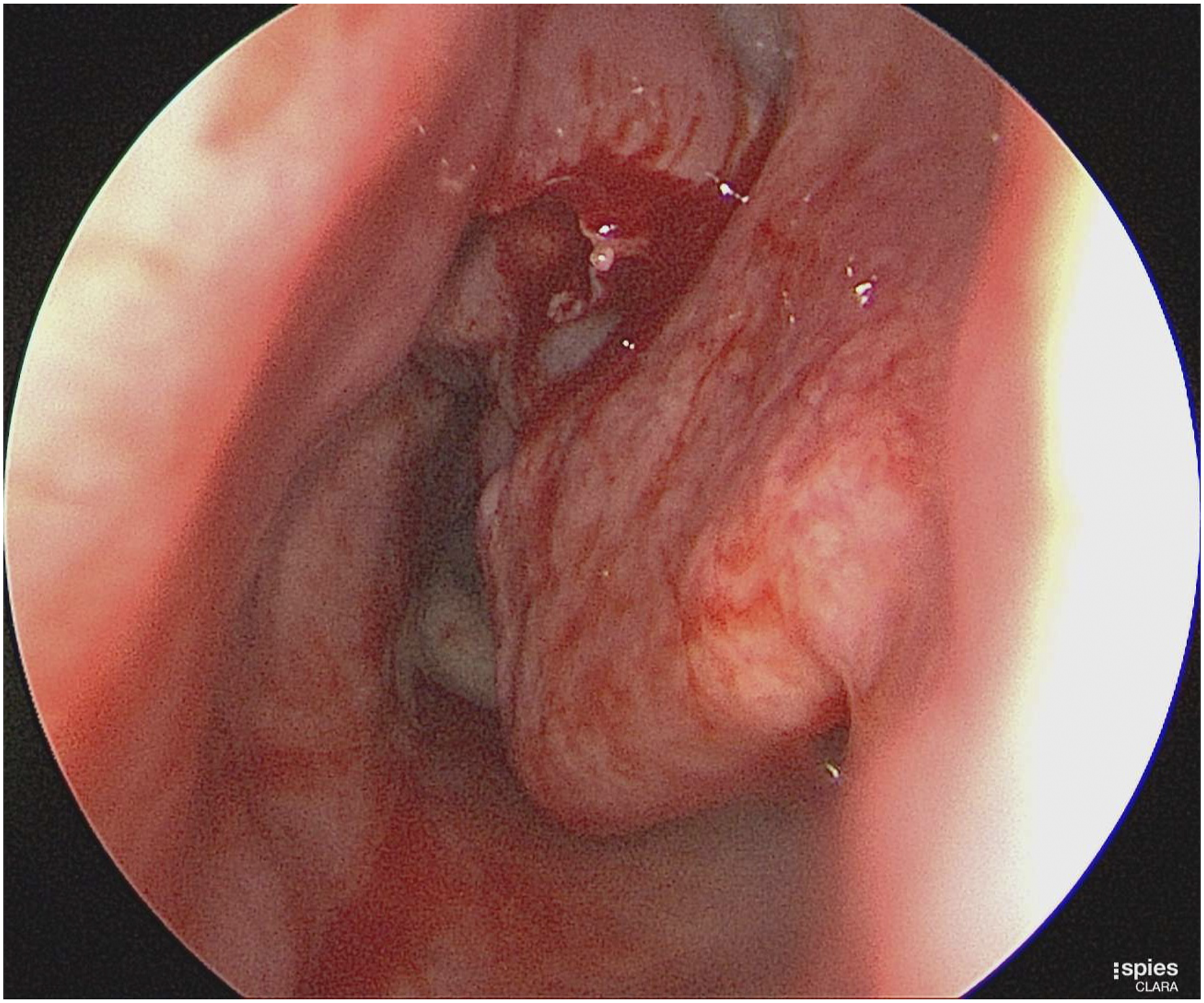
Furthermore, computed tomography scan examination of the paranasal sinuses is not feasible during pregnancy because of the risk of ionizing radiation. Owing to uncertainty regarding the diagnosis and the lack of similar presentations in the literature, we weighed the benefits and risks of the possible management choices. The patient was offered options including oral corticosteroids or to undergo a polypectomy and the patient preferred the latter option. So, a non–powered in-office polypectomy was done under local anesthesia with minimal bleeding and no packing required. It was done to relieve the nasal obstruction and to obtain a histopathological diagnosis (Figure 3). The patient reported complete resolution of the symptoms of nasal obstruction. Histopathological evaluation revealed an inflammatory nasal polyp. The patient was prescribed budesonide irrigation as one ampule (0.5 mg) in 250 mL normal saline twice daily. In addition, the post-polypectomy period was uneventful for the patient. After 2 weeks, an endoscopic examination in the clinic revealed that the polyps were stable in size and did not extend beyond the middle meatus. Laboratory investigations were unremarkable except for an IgE level of 50.50 IU/mL.
Pregnancy presents unique physiological changes that could develop because of hormonal changes, such as masses known as lobular capillary hemangioma, which is a rare type of benign lesion composed of fibroepithelial tissue with a high association with pregnancy and regression after delivery. 1 Lobular capillary hemangioma or pyogenic granuloma is diagnosed clinically by the rapid growth of a fleshy mass, symptoms of epistaxis or ulceration, and the presence of associated risk factors such as hormonal stimulation during pregnancy or oral contraceptive use. 2 History and clinical examination are crucial for the unusual presentation of a nasal mass. It should alert the physician to differential diagnoses, including lobular capillary hemangioma, sino-nasal malignancy, and nasal polyposis. 3 Unfortunately, the current literature on the management of nasal polyposis in pregnancy remains insufficient. 4
The management of nasal polyps as an office-based procedure by performing polypectomy is a more favorable method to manage patients without general anesthesia, with a target of faster symptom alleviation. 5 Generally, intranasal corticosteroids are recommended as a safe option for chronic rhinosinusitis during pregnancy. Furthermore, Budesonide is considered the safest choice among others by category B.6,7
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.