
Abstract
Antrochoanal polyp is usually a benign solitary mass lesion originated from maxillary sinus mucosa and emerging through maxillary ostium. We report a rare case of antrochoanal polyp and migrated dental implant in the ipsilateral maxillary sinus. Clinicians should be aware that ACP may have other concomitant conditions such as migrated dental implants.
Introduction
Antrochoanal polyp (ACP) is usually found as a unilateral solitary mass lesion which originated from maxillary sinus and emerging through accessory ostium. Children are more likely to experience ACP. 1 Also, it is believed to be caused by mucous gland obstruction in maxillary sinus mucosa after chronic inflammation. 2 However, there is no known clear mechanism for the occurrence of ACP. Herein, we report a case of antrochoanal polyp which is believed to be caused by maxillary sinus mucosal irritation caused by migrated dental implant.
Case Report
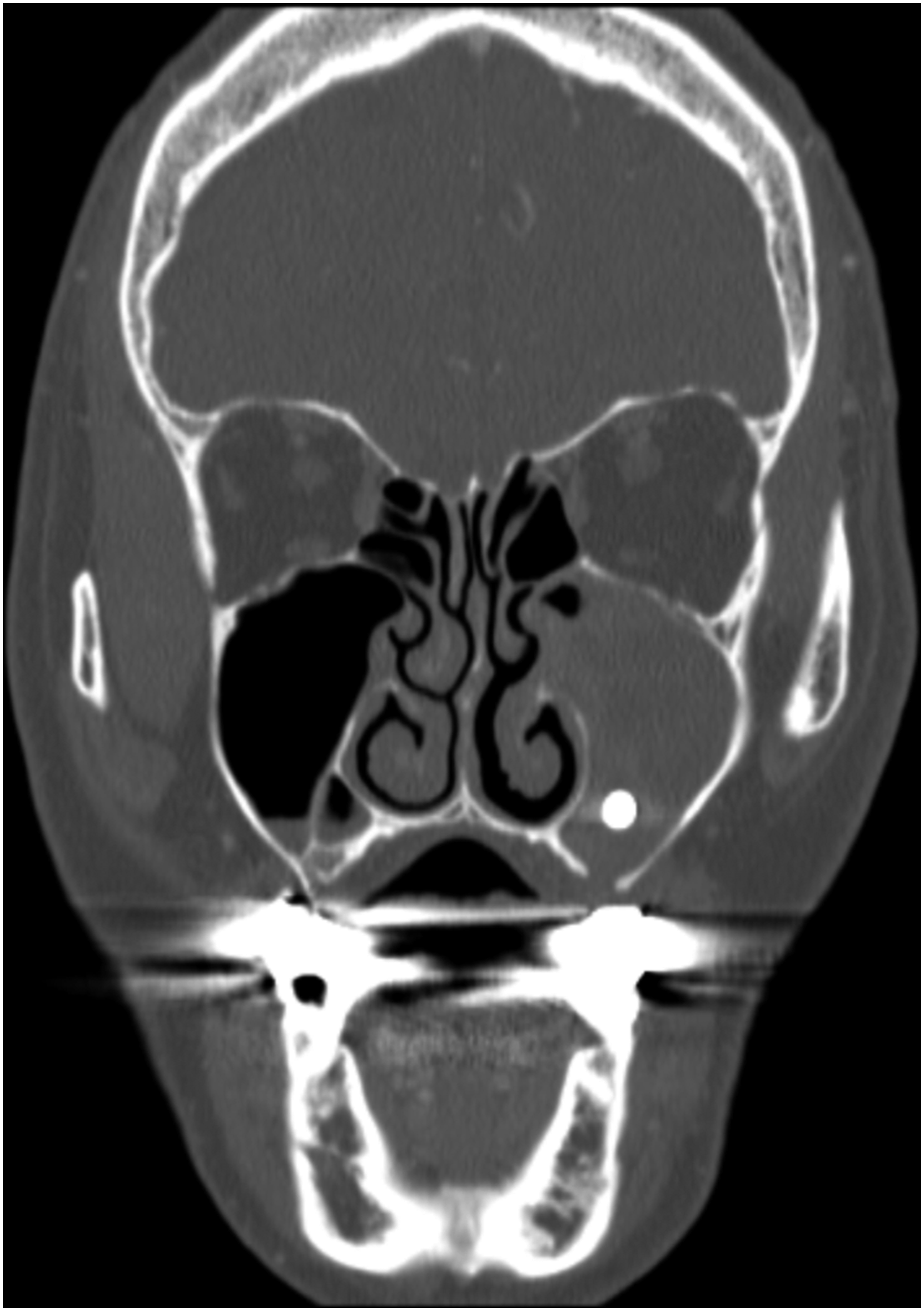
A 77-year-old woman was referred to our department, complaining of left nasal obstruction for the past five months. She also complained of purulent rhinorrhea, anosmia from left nose, and postnasal drip sensation. In history taking, she underwent dental implantation 6 months ago and complained of nasal obstruction one month after the procedure. She had no medical problems and no history of nasal surgery. In physical examination, pale polypoid mass emerging from left maxillary accessory ostium was observed in left nasal cavity and extended to the nasopharynx (Figure 1). On computed tomography (CT) scans, a 4 cm mass was seen occupying the maxillary sinus and extending into the nasopharynx through the maxillary accessory ostium, and sinusitis was present in the maxillary sinus (Figure 2). Also, metallic density lesion, suspected to be dental implant, was observed in the lower part of maxillary sinus (Figure 3). Antrochoanal polyp is elongated through left maxillary sinus accessory ostium. In the CT scan, soft tissue density fulfill left maxillary sinus and is continued to left posterior choana through maxillary sinus ostium. In the CT scan, metallic density is seen at inferior portion of the left maxillary sinus.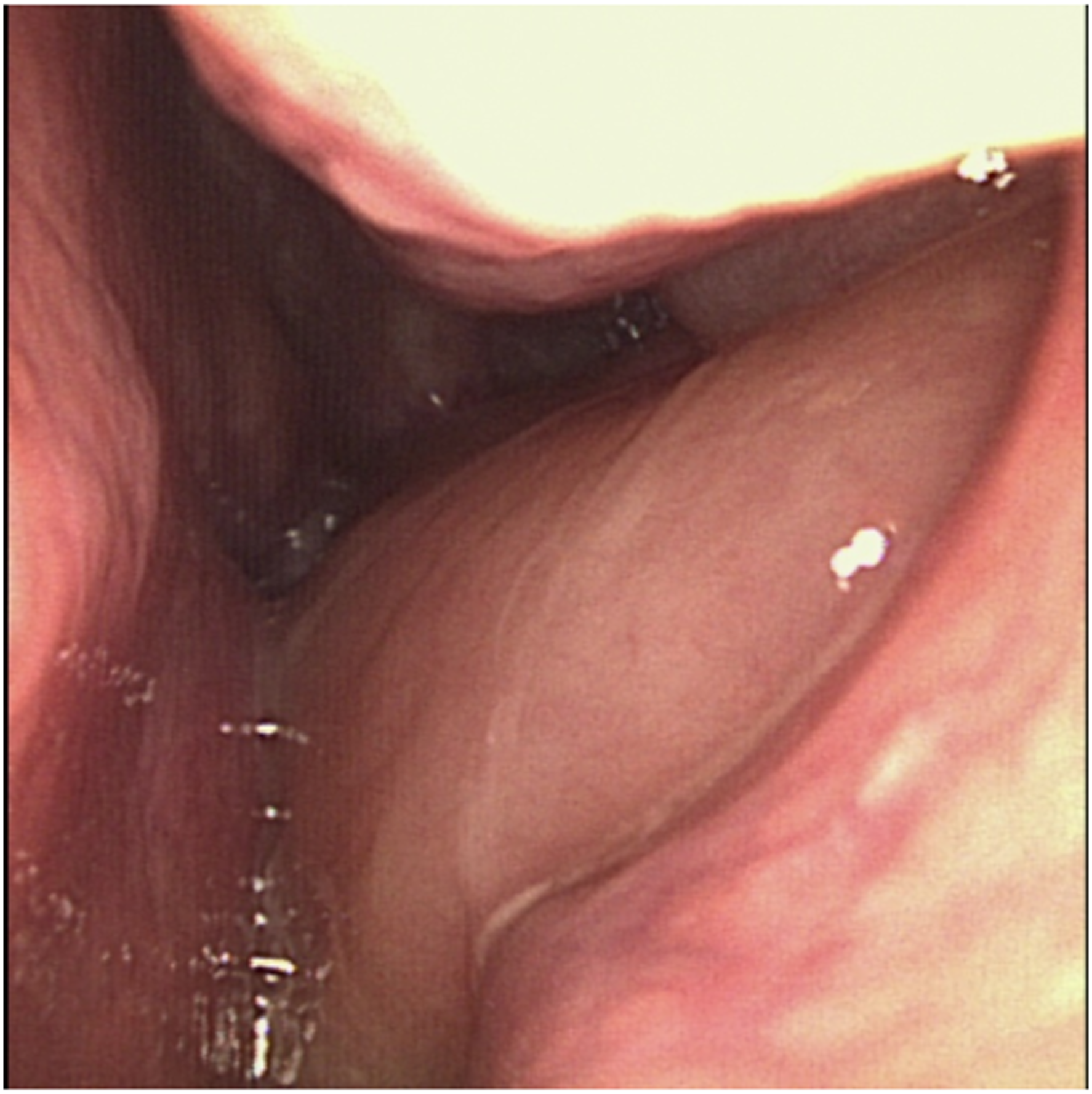

The patient underwent endoscopic sinus surgery. Polyp originated from maxillary sinus posterior wall elongated to left choana through left maxillary sinus ostium. Also, dental implant was found around the polyp in the maxillary sinus. To avoid recurrence, the polyp and dental implant were removed, and the base of the polyp in the maxillary sinus posterior was debrided (Figure 4). The histopathological result of polyp was sinonasal inflammatory polyp. At 2 years postoperatively, there was no recurrence of the polyp and the patient was being followed up periodically. Photo taken after the removal of the migrated dental implant.
Discussion
ACP is believed to be caused by acinar mucous gland obstruction after chronic irritation or infection in maxillary sinus.1-4 Mucus gland obstruction causes a hyperplastic alteration in the maxillary sinus mucosa, which has a cystic part. After a polyp fills the maxillary sinus, a solid part emerges via the maxillary ostium, causing a variety of symptoms. Mucus gland blockage can be caused by a variety of factors, including chronic sinusitis, although the exact cause is unknown. 2 In this case, patient’s symptoms occurred one month after implantation and migrated dental implant was found in the maxillary sinus near a polyp. Therefore, it can be said that mucosal irritation due to the migrated dental implant may have caused the ACP.
The most common presenting symptom of ACP is unilateral nasal obstruction.1-4 In addition, recurrent epistaxis, purulent rhinorrhea, polyp strangulation, dyspnea, dysphagia, falling into hypopharynx, and speech disturbance can occur. 2 In this case, patient complained of persistent unilateral nasal obstruction with anosmia, purulent rhinorrhea, and postnasal drip sensation.
The best diagnostic tool for ACP is CT.1-4 ACP showed a hypo attenuated lesion on CT scanning, occupying the maxillary sinus and continuing to the posterior choana or nasopharynx. Magnetic resonance imaging (MRI) can also be a good diagnostic tool. ACP showed T1 hypointense and T2 hyperintense lesion filling maxillary sinus. In gadolinium enhancing view, intrasinusal cystic part of the polyp can be peripherally enhanced and the nasal and choanal part of the polyp has hyperintense lesion. 2 Nasal endoscopy can be a basic diagnostic tool. Polyp emerging from maxillary sinus ostium continued to posterior choana or nasopharynx is observed in endoscopic view. Occasionally, polyp is elongated to oropharynx so that polyp can be seen through oral cavity. In this case, patient had undergone nasal endoscopy at first visit and performed CT scan.
The treatment of choice for ACP is surgery.1-5 Surgical technique varies from Caldwell-Luc technique to functional endoscopic sinus surgery. Currently, functional endoscopic sinus surgery is gold standard technique.2,4,5 The aim of functional endoscopic sinus surgery is the complete removal of ACP including origin site mucosa. To prevent recurrence, it is important to remove origin site of ACP. Therefore, an additional combined approach using a canine fossa approach may be necessary in some cases to ensure optimal visualization within the maxillary sinus. 5
Conclusion
We report a rare case of antrochoanal polyp and migrated dental implant in the ipsilateral maxillary sinus. Clinicians should be aware that ACP may have other concomitant conditions such as migrated dental implants.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.