
Abstract
Introduction
Femoral head specimens are often sent for histopathology after geriatric femoral neck fractures in patients with past history of malignancies. However, the cost-effectiveness of this practice is unclear and the clinical impact and effect on patient management has yet to be ascertained.
Methods
This is a retrospective review of all femoral head histopathology specimens registered in our center from 2003 to 2023. Patients <65 years of age were excluded from the study. Patient demographics were analyzed. Clinical notes and radiographic information were retrieved for all cases with positive histopathological findings to delineate any history of (1) atraumatic fractures, (2) prodromal pain and (3) radiological suspicion of pathological fractures. Any changes in subsequent management were also identified and analyzed.
Result
From the 1431 cases, the average age was 81.9 ± 7.91 years-old, with 986 females (68.9%). There has been a rising trend of femoral head biopsies over the past 20 years. Only 45 cases had a positive histological diagnosis (3.14%). Among which, 37 of them had radiological features of malignancy (82.2%). Thirty-five cases did not have a history of trauma prior to the fracture (77.8%) and 29 out of 44 cases had documented prodromal pain (64.4%). For the positive cases, just over half (26/45) experienced a change in the subsequent management plan. Majority of cases were managed by palliative intent with adjunctive radiotherapy or bisphosphonate therapy alone. Cost analysis showed the direct cost of pathological examination to be $395.78 USD per case, with an average of $12,585 per positive case. Only 1.8% of femoral neck biopsies were of clinical significance with change in management plans.
Conclusion
There is a low positive yield of femoral head biopsies with minimal change in management. Clinical history and radiological features can guide clinicians on the need for femoral head histopathology examinations.
Keywords
Introduction
In the realm of geriatric healthcare, hip fractures represent a significant clinical issue with approximately 10 million cases occurring globally each year (World Health Organization, 2021). 1 These fractures are not only prevalent but also coupled with high morbidity and mortality rates associated with an elderly population. The economic burden on the healthcare system is immense; on average, each hip fracture amounts to $43,669 in costs after 12 months of the injury. 2 Femoral head biopsies have been traditionally employed to ascertain any underlying pathology leading to hip fractures, particularly in cases with an active or past medical history of malignancy. However, recent data suggest that the incidence of positive biopsy findings is remarkably low, prompting concerns over the necessity and financial implications of this routine practice. 3
The healthcare system is increasingly under pressure to optimize resource allocation, especially in the face of an aging population with complex medical needs. This study aims to explore the cost-effectiveness of femoral head biopsies in geriatric patients with femoral neck fractures, hypothesizing that the procedure may be redundant and contribute to unnecessary healthcare expenditures. Previous literature indicates minimal alterations in treatment plans following biopsy results, suggesting that the financial costs may outweigh the clinical benefits.4,5 Furthermore, we sought to evaluate how clinical features such as atraumatic fractures, prodromal pain, and radiographic suspicion can be used to help guide clinicians in making histopathology requests.
Materials and Methods
Study Design and Setting
This study is a retrospective cost-benefit analysis conducted at The University of Hong Kong focusing on geriatric patients with femoral head sent for histopathology examination between 2003 and 2023 for treatment of displaced geriatric femoral neck fractures.
Ethical Statement
This study was conducted in accordance with the ethical standards of the Declaration of Helsinki and was approved by the center’s institutional review board. All data utilized was anonymized to ensure patient confidentiality.
Participants
Eligibility criteria included all patients who underwent total hip arthroplasty or hemiarthroplasty surgery for displaced femoral neck fracture and had their femoral heads sent for histopathological examination. Patients who were <65 years of age, with incomplete medical records such as transfer to other institutions post-operatively or those who underwent image guided core biopsies were excluded. Participant flow chart is shown in Figure 1. Patient selection flow chart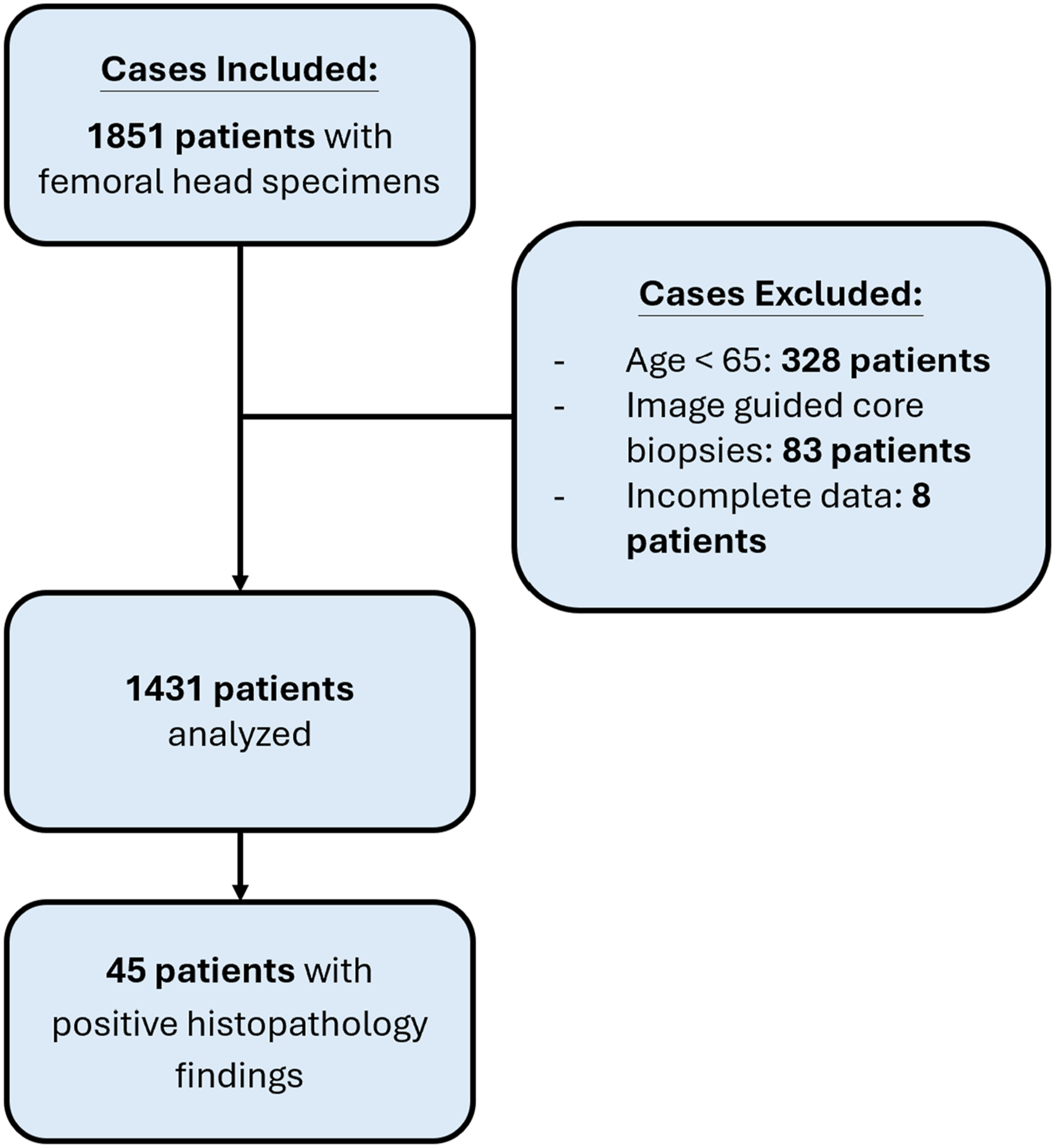
Data Collection
Data was collected retrospectively from electronic medical records. Variables included patient demographics (age, gender), comorbidities, biopsy results, treatment plans, and healthcare costs associated with the biopsy procedure. Clinical notes were analyzed for prodromal pain, atraumatic history and any radiographic suspicion of pathological lesions.
Cost Analysis
The cost analysis was performed using micro-costing methods, where each component of the biopsy procedure was itemized and aggregated. Costs were calculated in US Dollars. The costs for paraffin block preparation requiring decalcification (per block) were calculated to be $67.57 (USD). Breakdown direct micro-costs are as follows: $37.86 for medical technologist test handling, $9.38 for reagents and consumables, $19.93 administration charge, utilities, facilities maintenance and supplies, $0.40 for tissue processor depreciation and maintenance fees. An average of four blocks are taken per specimen. Anatomical Pathologist unit pay for specimen handling, examination and reporting was taken as the Hospital Authority of Hong Kong average specialist hourly rate of $125.50. Total costs for specimen were calculated as $395.78.
Outcome Measures
The primary outcome measure was the change in treatment plans post-biopsy. Secondary outcomes included the direct medical costs of the biopsy procedure and the incidence of positive biopsy findings. All positive biopsy cases were analyzed for clinical history of prodromal pain, atraumatic fracture and/or suspicious lesion on radiographic imaging. Statistical correlation of clinical and radiological findings with positive biopsy findings was performed using Spearman Rank correlation.
Results
Patient Demographics and Clinical Characteristics
A total of 1851 patients met the inclusion criteria. After exclusion of young hip fractures and core biopsies - a total of 1431 cases were analyzed. The average patient population age was 81.9 years old. The majority were females accounting for 68.9% of the patients (986/1431).
Incidence of Positive Biopsy Findings
Out of the 1431 arthroplasty surgeries for femoral neck fractures with femoral head biopsy specimens sent for tissue histopathology examination, only 45 (3.1%) yielded positive findings for malignancy or other pathological diagnoses. The number of positive biopsies per total biopsies for each year is shown in Figure 2. The average positive yield percentage is 3.72% (range: 0% to 10.7%) per year. There was a rising number of specimens sent up until 2019 when the COVID-19 pandemic occurred. In 2019, there were a total of 118 specimens sent from geriatric hip fracture surgeries with only one positive biopsy that year. Since then, change in clinical practice was implemented in our institution reflecting the need to reduce unnecessary histopathology examinations. Annual femoral head specimen numbers and number of positive cases
Out of the positive biopsy cases, 21 histopathology examinations found metastatic carcinoma (CA) of the lungs (47%), ten CA prostate metastases (22%), seven haemato-proliferative disease including multiple myeloma, lymphoma and leukemia (16%). Renal cell carcinoma metastases had two cases (4%) while CA breast, CA colon, CA thyroid, endometrial CA, cholangiocarcinoma, hepatocellular CA, squamous cell carcinoma and metastatic leiyomyosarcoma each accounted for one case (2%). There was one case of unknown primary with poorly differentiated carcinoma (2%). Apart from metastatic disease, there was also one case of known amyloidosis with evidence of the systemic disease seen on bone biopsy and one case of newly diagnosed tuberculosis of the bone.
Impact on Treatment Plans
Among the total biopsy cohort, treatment plans were altered in only 26 cases (1.8%) as a result of the positive biopsy results. The majority of adjunctive management from positive biopsy results came in the form of additional palliative radiotherapy to the affected femur (21 cases). Five cases had additional chemotherapy or immunotherapy regimen changes for progressive disease (11%) and four cases had additional Zoledronic acid infusion or Denosumab injection for metastatic bone disease (9%). There was one case confirmed to be tuberculosis (TB) with anti-TB drugs given for nine months duration (2%). There was no survivorship benefit from having a positive biopsy case with the mortality rate for positive and negative biopsies as 91.1% and 65.4% respectively. Average time from operation to death was 4.27 ± 8.38 years with negative biopsies and 3.64 ± 16.7 years in positive biopsy case.
Cost-Benefit Analysis
The cost-benefit analysis revealed that the additional expense incurred by performing femoral head biopsies did not correlate with improved patient outcomes. The total direct costs of histopathological examination were $566,361 over these years. Cost per positive case detected was calculated to be $12,585. An average $27,427 of health care expenditure was wasted on femoral head biopsies per year. There was no survivorship benefit with positive biopsy cases and no net monetary benefit was perceived.
Clinical Radiological Correlation to Positive Biopsy Cases
Number of Patients With Positive Clinical History And/or Radiological Features (N = 45)

Discussion
Our findings revealed a very low incidence of positive biopsy results and even less leading to changes in treatment plans — only 1.8% of all biopsy cases. This supports the hypothesis that these biopsies are often unnecessary. The low incidence of biopsy-driven changes in treatment plans underscores the potential for healthcare cost savings through the adoption of alternative diagnostic approaches. Clinical history of prodromal pain, atraumatic fractures and suspicious lesion on radiographs had high correlation to positive biopsy results. If none of these are present – histopathological examination of femoral head biopsy can be omitted. Changes in clinical practice to stop routine sending femoral head for histopathology because of past history of malignancy without relevant clinical and radiological findings can save hospitals upward of $25,000 per year. Additionally, it would help reduce workload for anatomical pathologists and laboratory technicians. Femoral head bone specimens require decalcification and the average time for histology report after receiving specimen was 8.5 ± 4.9 days in our center. Patients and their families have an additional psychological burden waiting for test results with the worry of cancer recurrence or progressive disease.
These findings align with previous studies by Karuppia et al (2019) and Davis (2019), which highlighted similar inefficiencies in biopsy use in this patient population.3,4 Femoral head biopsies in geriatric patients with femoral neck fractures may not provide sufficient clinical benefit to justify the associated costs. Another study looking at routine evaluation of donated bone has been studied in a population of hip arthroplasty cases for various conditions and found a positive malignancy detection of 1 per 770 cases. 6 Suggestion of careful detailed clinical history and physical examination is important. A study in the United Kingdom found that history of malignancy and bone metastases had a positive biopsy rate of 0.44%. 7 From Davis et al 3 apart from history of malignancy, 75% of cases with positive biopsy had prodromal hip pain. While additional radiographic suspicion also provided an additional positive predictive value of 0.62 for positive biopsy results. 4 Similar to our results, in this study the additional combining of radiographic and clinical history of atraumatic history, prodromal pain had a sensitivity 1.0 and specificity of 0.35. 4
Changes in clinical management were even less prevalent. For routine examination of hip arthroplasty cases a study of 6745 cases yielded only two requiring changes in treatment plans. 8 No changes in clinical treatment was found in another study out of 466 femoral head specimens. 3 Metastatic and pathological fractures of the proximal femur have been managed operatively with good survivorships. 9 In a systematic review there was lack of clear evidence for post-operative radiotherapy after surgical stabilization of pathological fractures. 10 Some studies in the review noted possible complications from radiotherapy including poor bone healing and the negative effects of radiotherapy on quality of life may outweigh the risk of local progression or implant failure. There is also an increase in the use of pharmacological management in bone metastases. Ultimately, the oncological treatment adjuncts are subject to individual patients, expected prognosis, quality of life and risks of complications.
Weaknesses and Limitations
This is a single-center study retrospective analysis and cost calculations may vary across different centers and regions. False positive for clinical history of atraumatic fracture, prodromal pain and/or radiological features of malignancy were not analyzed in this study. Follow-up on the outcome of patients receiving additional treatment for positive histopathological study was not carried out to review the extended quality-adjusted life year (QALY) attained. Quality of life after additional treatment cannot be measured objectively limited by retrospective study. Sample size calculations were not performed as QALY was not measured. Further studies on number needed to treat for sending femoral head biopsy and assessing its cost-effectiveness may further support our conclusions. The single-center setting may limit the generalizability of the findings to other healthcare and laboratory environments.
Conclusion
Routine femoral head biopsies may not provide sufficient benefit to justify their cost. Histopathology examination of femoral heads frequently results in minimal changes to treatment plans, with a notably low incidence of positive biopsy results. This study suggests a potential shift in clinical guidelines, advocating for a more selective approach to femoral head biopsies for femoral neck fracture cases - reserving it for cases with a higher index of suspicion for malignancy based on clinical and radiological assessment. Surgeons can help drive down healthcare costs and pathologist workload.
Footnotes
Ethical Considerations
This study was performed in line with the principles of the Declaration of Helsinki. This is an observational study. The HKWC/The University of Hong Kong Institutional Review Board has confirmed that no ethical approval is required.
Author Contributions
CSYY and CF contributed to the study conception and design. Material preparation, data collection and analysis were performed by TWSL and HMC. The first draft of the manuscript was written by CSYY and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.