
Abstract
Introduction
This study’s purpose was to use a postoperative ICU geriatric prediction score (PIGS) to determine the appropriateness of postoperative ICU/SDU admission or unnecessary use of advanced care services in geriatric femur fracture patients at our Level III trauma center.
Methods
This is a retrospective review of 142 patients, age 65 years or older, at a level III trauma center from 3/2021-9/2022 that required surgical fixation of a femur fracture. Collected data included demographics, injury characteristics, postoperative complications, hospital charges, and admission to ICU or SDU.
Results
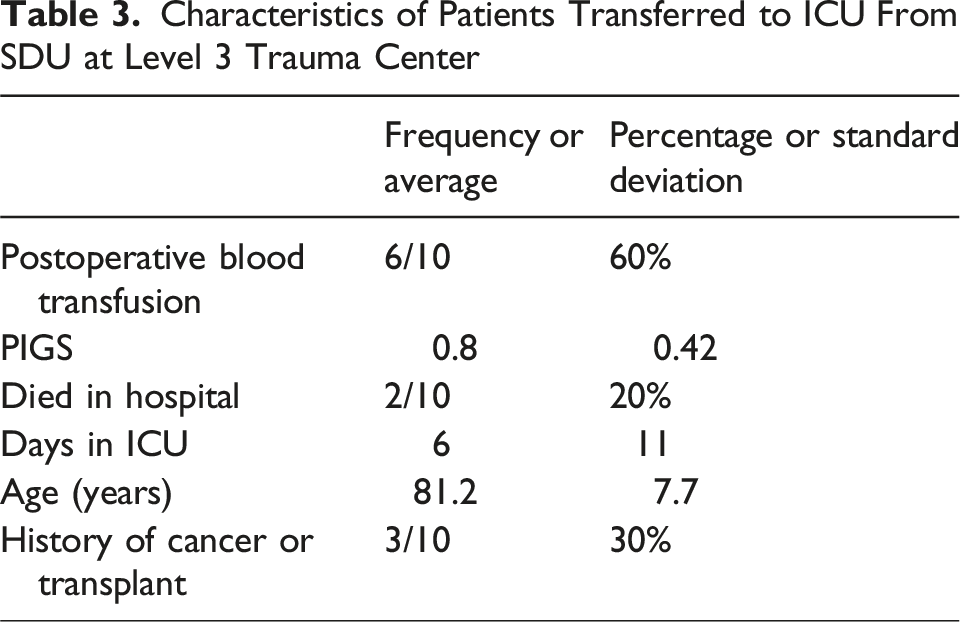
Average age was 81.5 years. 32% of patients were male and 40% were femoral neck fractures. The average PIGS score was 7.1. 17% of patients admitted to the SDU met the PIGS threshold for ICU transfer. 7% were transferred to the ICU after being admitted to the SDU postoperatively, 0% of whom met criteria for ICU admission at the level 1 trauma center. Predictive factors for their transfer to the ICU at the level 3 trauma center was postoperative blood transfusion (OR:4.11;CI 1.09,15.45;P = 0.036) and history of cancer or organ transplant (OR:5.86;CI 1.2926.58; P = 0.022). Predictive factor of postoperative death (aside from transfer to ICU) was a history of cancer or organ transplant (OR:13.90;CI 7.65,25.25;P = 0.007). Average gross charges per patient admitted to the floor and the SDU were $80,383 and $82,590, respectively,P = 0.372.
Conclusion
The geriatric population with a femur fracture is often unnecessarily admitted to advanced care units postoperatively. The PIGS system has been validated for use in a level 1 trauma center in the geriatric population undergoing hip fracture surgery. Here, we validate its use in the geriatric population undergoing femur fracture surgery at a level III trauma center, where majority of patients may not meet the criteria for advanced care and could be cared for more cost-effectively.
Introduction
Hip fractures are the second most common type of fracture in adults among both men and women. 1 They are even more prevalent within the geriatric population 2 and are associated with significant financial burden, loss of independence, morbidity, and mortality,2-8 with a 1-year mortality estimated to be as high as 22%. 9 After sustaining a hip fracture, it is estimated that only about 30% of patients will return to their pre-injury levels of mobility and independence. 10 With an aging US population, 11 hip fractures will continue to increase, so it is essential to understand the specific risk factors in this demographic to fully optimize their care. Also, the occupancy of inpatient hospital beds continues to rise 12 as the number of hip fractures increases, with 1.3 million reported globally in 1990 and models predicting a rise to 7-21 million reported in 2050. 13
An important consideration in the care of geriatric hip fracture patients is their postoperative course – in particular, whether patients are admitted to the intensive care unit (ICU), a stepdown unit (SDU), or the medical/surgical units. The definition of a stepdown (sometimes a “step-up”) unit varies by geographic location, 14 but the unifying feature is the provision of an intermediate level of care between that which can be provided in the ICU and the medical/surgical units. This level of care is largely determined by the nurse-to-patient ratio and the ability to provide specific organ support. 15 Nurse-to-patient ratio for SDU ranges from 1:2 to 1:4, while ICU ranges from 1:1 to 1:2, and medical/surgical units can be as high as 1:10. 11 Large studies have demonstrated that up to 20% of patients are admitted to either an ICU or SDU following inpatient orthopedic surgeries. 16 Admission to such advanced care units (eg, ICUs, SDUs) is known to be associated with increased costs and longer hospital stays when compared to the medical/surgical units.16,17 It is also associated with more complications, 18 a lower prevalence of home discharge,15,16 and a higher mortality,19-21 especially among elderly patients 22 ; though sicker patients go to higher levels of care so their complications and LOS will often be greater as well.
Proper triage of surgical patients relies most heavily on the assessment of specific pre- and intraoperative risk factors. Delays in surgery, increased length of stay, preoperative neurological comorbidities, and intraoperative hypotension are known risk factors for ICU admission.
23
ICU admission that is unplanned tends to have worse outcomes,21,23 and is associated with increased age and BMI, ASA score 3 or greater, use of intraoperative vasopressors, intraoperative blood transfusion, lower preoperative hemoglobin levels, renal disease, history of smoking, and severity of injury.20,24-28 The National Surgical Quality Improvement Program (NSQIP) has developed a risk calculator tool for determining risk of morbidity, mortality, and 6 other postoperative complications of surgery, but this tool assesses the risk of a broad range of procedures across all surgical subspecialties except for transplant and trauma.
29
Another risk calculator exists that is specifically for unplanned ICU admission after elective THA,
30
but this includes patients younger than 65 years old. A previous study created a scoring system after analysis of unplanned postoperative ICU transfers at our Level I trauma center. The scoring system, Postoperative ICU Geriatric Score (PIGS), determined a threshold value at which at-risk patients would benefit from immediate postoperative ICU transfer to minimize the risk of unplanned ICU transfer and later complications (Figure 1). It was determined that the score of 13 was the threshold at which patients should be admitted to the ICU postoperatively. In their cohort of 92 patients, 63.6% of patients with a score ≥13 and 100% of patients with a score >15 experienced an unplanned ICU admission, whereas only 8.6% of patients with a score <7 were transferred to the ICU.
31
Calculating Postoperative ICU Geriatric Score (PIGS)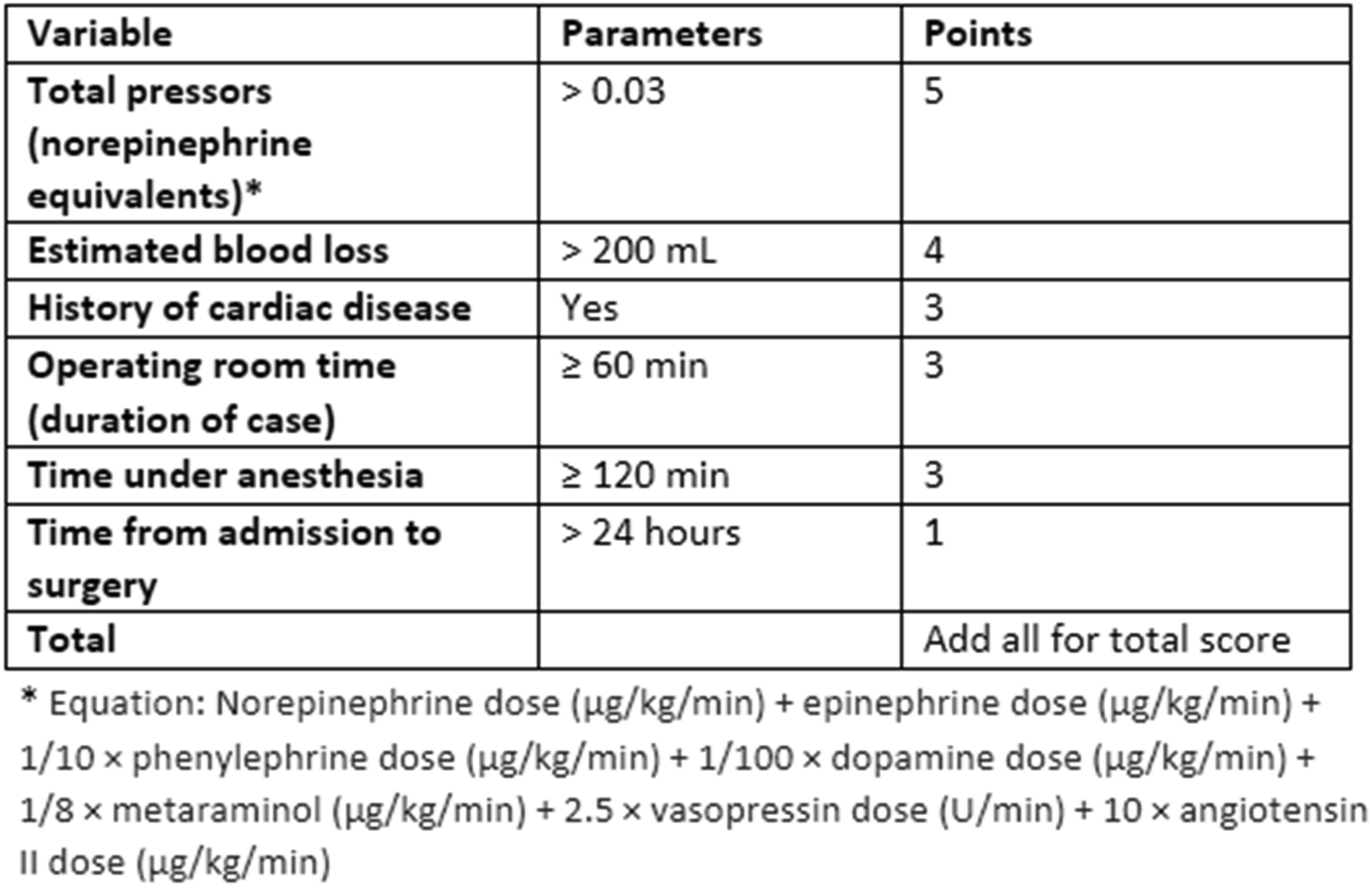
This study’s purpose was to use the PIGS system to determine the appropriateness of postoperative admission or unnecessary use of advanced care services (eg, ICU or SDU) in geriatric hip fracture patients at our Level III trauma center. We hypothesize that most of the cohort are unnecessarily transferred to advanced care units as determined by the PIGS system.
Methods
This study is a retrospective chart review of 142 geriatric patients at a level III trauma center from 3/2021-9/2022, where regardless of other factors all geriatric femur fractures are admitted to the SDU postoperatively. Inclusion criteria included surgical fixation of a femur fracture of any type, age of 65 years or older, and admission to the stepdown unit postoperatively. Exclusion criteria included age less than 65 years or absence of femur fracture. All 142 patients met these criteria.
Data collected from chart review included demographics (age, race, ethnicity, height, weight, body mass index), medical comorbidities, home oxygen use, home anticoagulant use, mechanism of injury, concomitant injuries, location of femoral fracture, injury severity score (ISS), Charlson comorbidity index (CCI), timing of care (time from admission to surgery, time from admission to discharge, time from surgery to discharge), surgical information (American Society of Anesthesiology score, fixation and operative treatment of fracture, duration of anesthesia (from time of induction to emergence), duration of procedure (from time of incision to closure), duration in post-anesthesia care unit (PACU)), estimated blood loss (EBL), intraoperative complications, hospitalization course (complications during stay, need for blood transfusion, hypoxia, hypotension), and discharge status (weightbearing status, disposition). Timing of care was calculated based on the date and time entered into the patient’s medical records. Time and date of admission was taken from first presentation to the emergency room, discharge time and date was based on what was recorded in the electronic medical record. Time and date of surgery was based on procedure start time as recorded by the operating room circulatory nurse. Procedure end time, anesthesia end and start time, and PACU start and end time were also based on the times recorded by the nursing staff. EBL and intraoperative complications were recorded from the surgeon’s and anesthesia provider’s operative notes. Hospitalization course and discharge status details were recorded from provider notes in the electronic medical record. Additionally, the PIGS value (as referenced previously and detailed in Figure 1) was calculated for each patient and noted if the scoring threshold of 13 was reached. The chart review was conducted over a 3-month period.
Gross charges were calculated for a set of patients admitted to the floor unit and for those admitted to the SDU post-surgery during the same 3-month time period. Fifteen patients were in the floor group (at the Level I trauma center) and 32 patients were in the SDU group (at the Level III trauma center).
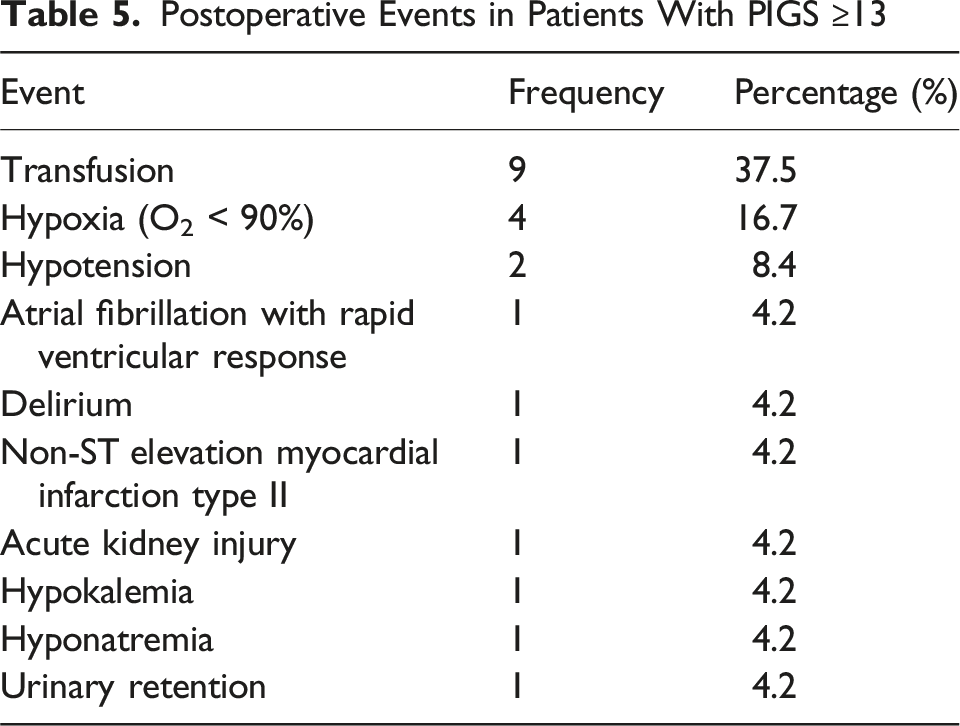
Data was compiled to determine frequencies of each variable and the percentage of femur fracture patients that were at or above the PIGS threshold value of 13 at the level III trauma center. The patients who scored a 13 or higher were further investigated for significant adverse events postoperatively that would have led to an ICU transfer at the level 1 trauma center. During the same period, 3 patients were transferred from the level III trauma center to the level I trauma center.
Results
Patient Characteristics and Admission Course Details

Frequency of Patients at or Above PIGS Threshold for ICU Transfer

Characteristics of Patients Transferred to ICU From SDU at Level 3 Trauma Center
Predictive Factors for Transfer to ICU and Death

Postoperative Events in Patients With PIGS ≥13
Cost Differences Between Floor and Stepdown Units

Discussion
As risk factors for unplanned ICU and SDU transfers are determined in the current literature, more focus is being placed on identifying patients preoperatively of being at high risk for a postoperative ICU transfer. This preoperative prediction is important as patients who have an unplanned ICU transfer have poorer outcomes when compared to those with a planned ICU transfer.16-19 With these risks being even more prevalent in the geriatric population, 22 some level III trauma hospitals may opt for automatic admission to an SDU or ICU after surgery.
However, the overuse of advanced levels of care increases the costs to the patient and potentially leads to overcrowding of the ICU or SDU. PIGS is implemented within our level I trauma center and is used to determine whether a patient will be taken to the ICU or general floor unit postoperatively. Most of our cohort (83.1%), had they been admitted to the level I trauma center, would have been taken to the medical/surgical unit postoperatively and 16.9% would have been admitted to the ICU immediately postoperatively. Interestingly, the PIGS system was not predictive of unplanned ICU transfer or death in our level III trauma center’s population. However, upon further review, the use of postoperative transfusion and if the patient had a history of cancer/organ transplant were predictive of unplanned ICU admission. Additionally, history of cancer/organ transplant was present in 100% of patients that died postoperatively and 30% of patients transferred from SDU to ICU.
In a retrospective analysis of over 3 million hospital admissions, unplanned ICU admissions for surgical patients increased their medical costs by $21,448. 32 This is a significant cost burden to patients. Similarly, through our cost analysis, the revenue stream can be increased by not admitting patients to the SDU that are stable for the floor (medical/surgical unit). Recent studies assessing ICU transfers after hip fracture surgery in the geriatric population have shown that when a postoperative screening intervention (carried out in the postoperative anesthesia care unit) is implemented, there is a decrease in the number of unplanned ICU transfers. One study’s postoperative screening protocol included laboratory tests, chest X-ray, and electrocardiogram which totaled to a $282 charge to the patient. 33 However, our implementation of the PIGS system and noting if they required postoperative transfusion or had a history or cancer/organ transplant added $0 to the patient’s hospital admission costs as it uses patient data that is already recorded and standard of care (Figure 1).
Advanced levels of care (ICU and SDU) should be used when appropriate for the patient’s medical and/or surgical needs. Immediate postoperative assessment of the patient should include the use of the PIGS system, noting whether postoperative transfusion was needed, and if the patient has a history of cancer/organ transplant to determine if the patient necessitates ICU or SDU transfer. These measures aim to decrease the financial burden on patients and minimize the excessive utilization of higher levels of care. By implementing this approach, advanced medical units can optimize their resources and prioritize patients who genuinely require intensive care, ensuring a more cost-effective, efficient, and equitable healthcare system.
Conclusion
The geriatric population that sustains a femur fracture is often unnecessarily admitted to advanced care units postoperatively. Though they are more at risk for postoperative complications, a screening tool should be used to assess if there is a need for ICU or SDU admission. The PIGS system has been validated for use in a level 1 trauma center in the geriatric population undergoing hip fracture surgery. Here, we validate its use in the geriatric population undergoing femur fracture surgery at a level III trauma center, where 83.1% of these patients may not meet the criteria for advanced care and could be cared for in a more cost-effective manner.
Footnotes
Ethical Consideration
The study was conducted in accordance with the Declaration of Helsinki and was approved by the University of Cincinnati Institutional Review Board, IRB #2020-0116 on June 2023, with the need for written informed consent waived.
Consent to Participate
This was a retrospective study and did not require patient consent for medical record review per the IRB.
Author Contributions
Sarah Kurkowski (data collection, manuscript writing), Jacob Meyer (data collection, manuscript writing), Quinn Retzloff (manuscript revising, data collection), Jonathan Harley (data collection), H. Claude Sagi (topic creation, manuscript revising/writing, senior author), Richard Laughlin (manuscript revising/writing, senior author).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available upon request.