
Abstract
The objective of this 3-year retrospective, controlled, cohort study is to characterize an interdisciplinary method of managing geriatric patients with hip fracture. All patients aged 65 years or older admitted to a single academic level I trauma center during a 3-year period with an isolated hip fracture were included as participants for this study. Thirty-one geriatric patients with hip fracture were treated with historical methods of care (cohort 1). The comparison group of 115 similar patients was treated under a newly developed, institutional comanagement hip fracture protocol (cohort 2). There were no differences in age, sex distribution, or comorbidity distribution between the 2 cohorts. Patients requiring intensive care unit (ICU) admission decreased significantly from 48% in cohort 1 to 23% in cohort 2 (P = .0091). Length of ICU stay for patients requiring ICU admission also decreased significantly, from a mean of 8.1 days in cohort 1 to 1.8 days in cohort 2 (P = .024). Total hospital stay decreased significantly, from a mean of 9.9 days in cohort 1 to 7.1 days in cohort 2 (P = .021). Although no decrease in in-hospital mortality rates was noted from cohort 1 to cohort 2, a trend toward decreased 1-year mortality rates was seen after implementation of the hip fracture protocol. Hospital charges decreased significantly, from US$52 323 per patient in cohort 1 to US$38 586 in cohort 2 (P = .0183). Implementation of a comanagement protocol for care of geriatric patients with hip fracture, consisting of admission to a geriatric primary care service, standardized perioperative assessment regimens, expeditious surgical treatment, and continued primary geriatric care postoperatively, resulted in reductions in lengths of stay, ICU admissions, and hospital costs per patient. On an annualized basis, this represented a savings of over US$700 000 for our institution.
Introduction
Hip fractures represent one of the most common orthopedic diagnoses leading to hospital admission, morbidity, and mortality in the elderly population, 1 with a current number of annual hip fractures occurring in the US Medicare population estimated at 418 000 in 2002. 2 As the number of older adults increases, the number of elderly individuals sustaining hip fractures is expected to increase concordantly annually, 3 despite some recent investigations demonstrating a slight decrease in hip fracture incidence. 4 –6 There is considerable cost associated with hospitalization and subsequent rehabilitation for each of these patients. Both in the United States 7 and in foreign countries, 8,9 the medical-economic impact of hip fractures on national health care costs is substantial. The annual cost of treating hip fractures in all age-groups in the United States was estimated at US$9 billion in 2004. 10 It has been estimated that total annual costs may escalate to US$240 billion by the year 2040. 7
Standardized management protocols have been demonstrated to be beneficial for management of patients with hip fracture in some recently published reports. 10 –14 In light of these reports, an interdisciplinary team of physicians and allied health professionals at our institution has developed a “hip fracture protocol” for the management of geriatric patients with hip fractures. Prior to development of the hip fracture protocol, care was provided for geriatric patients with hip fracture by hospital admission to the orthopedic surgery service, followed by medical consultation only as deemed necessary by the admitting surgeon. The hip fracture protocol provided for admission of geriatric patients with hip fracture to generalist (not orthopedic) services, with comanagement of these patients by the orthopedic surgery service. The purpose of this study was to examine the effectiveness of this hip fracture protocol in improving outcomes of geriatric patients with hip fracture. We hypothesized that the hip fracture protocol would result in improvements in the hospital process (eg, time from admission to the operating room [OR]), hospital course (eg, decreased intensive care unit [ICU] stays and hospital lengths of stay), and decreases in hospital charges.
Materials and Methods
In January 2005, we developed a hip fracture protocol intended for management of patients aged 65 years or older presenting to our emergency department or via transfer from an outside facility with hip (femoral neck or intertrochanteric femur) fractures. Our hip fracture team was comprised of clinical faculty from the departments of orthopedic surgery, community and family medicine (geriatrics division), internal medicine, anesthesiology, physical medicine and rehabilitation, and emergency medicine. Other members of the team included representatives from the nursing staff, therapy services, and the Office of Clinical Effectiveness (OCE, a quality management team established by our hospital system). As our institution is an academic medical center, orthopedic, medical, and family medical resident physicians of all levels of training were involved in the care of every patient with hip fracture.
As traditional standards of care for geriatric patients with hip fracture have resulted in disappointing outcomes, 15 our center developed an interdisciplinary protocol for the care of elderly patients with hip fracture. Development of the protocol was a collaborative effort between the Departments of Community and Family Medicine, Internal Medicine, and Orthopedic Surgery at our institution. When patients arrive at the emergency department, the protocol is activated, resulting in admission of the patient to a primary care medical service with orthopedic consultation. The goal of the protocol is expeditious but safe care of these patients with hip fractures and multiple comorbidities. 16 –18 A standardized order set was developed and is utilized in the emergency department as well as for admission to the hospital, postoperatively, and for discharge. Particular attention was paid to avoidance of contraindicated medications 19 –21 that have been demonstrated to increase the risk of delirium in the elderly patient and often increase hospital length of stay.
Admission of elderly patients with hip fracture is evenly distributed between the geriatric services of the University of Missouri’s Department of Community and Family Medicine and Department of Internal Medicine. A prearranged hip fracture protocol call schedule, which alternates between the two departments on a weekly basis, determines the admitting service. All faculty members in both departments who have nightly admitting responsibilities are included in this hip fracture protocol call schedule. When the patient with hip fracture arrives in the emergency department, the appropriate service’s admitting resident physician is paged. Mid-level providers (eg, physician assistants and nurse practitioners) are not involved in the delivery of care for these patients. The orthopedic resident physician on call is also automatically paged for consultation regarding the hip fracture. The protocol-driven process then proceeds from that point, utilizing standard order sets and with emphasis on expedited surgical management of the hip fracture.
A total of 31 elderly patients with hip fracture were admitted to the orthopedic service at our institution during the year of protocol development, and this population represented cohort 1. Cohort 2 (115 patients) represented the population of geriatric patients with hip fracture admitted to our institution during the first 2 years of hip fracture protocol implementation. After approval by our institutional review board, results of the intervention (implementation of the hip fracture protocol) were analyzed by the OCE as a continuous quality improvement (CQI) process. Outcome measures included in-hospital mortality, hospital length of stay, delay from admission to OR, ICU stays, and hospital charges per patient. This data collection was undertaken in a prospective fashion, and results were pooled for continuing review by the hip fracture team on a monthly basis. The 1-year mortality rates were obtained via review of the US Social Security Death Index.
In order to establish that cohorts 1 and 2 were similar to each other, a chi-square (χ2) analysis was undertaken to compare the cohorts regarding average age, female-to-male proportion, and the presence or absence of various medical comorbidities (eg, hypertension and diabetes). In-hospital lengths of stay, and lengths of ICU stay when required, were compared between cohorts utilizing analysis of variance (ANOVA). Chi-square analysis and ANOVA were utilized to compare times to OR from hospital admission and to compare percentage of patients requiring a stay in the ICU. In-hospital mortality rates between the cohorts were compared utilizing Fisher exact test, as the number of observed events was less than 5 in cohort 1. The 1-year mortality rates and 30-day hospital readmission rates were compared using χ2 analysis. Hospital charges were compared between cohorts utilizing a 2-tailed Student t test. Significance level was set at P < .05.
Results
A total of 31 patients comprised cohort 1, and 115 patients comprised cohort 2. Average patient age, sex distribution, and comorbidity profile (diabetes mellitus, congestive heart failure, dementia, history of stroke, and hypertension) were similar across both cohorts (χ2, P > .05 for all categories; see Table 1).
Patient Populations Were Similar in Both Cohorts (χ2, P > .05 for Each Category).
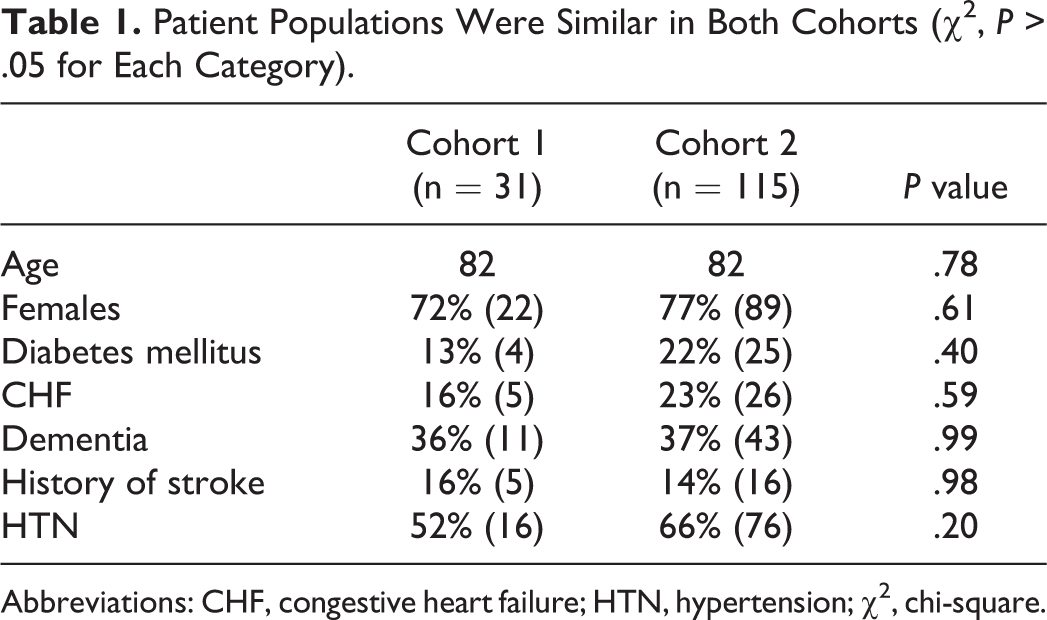
Abbreviations: CHF, congestive heart failure; HTN, hypertension; χ2, chi-square.
Total hospital length of stay decreased after implementation of the hip fracture protocol. Length of hospital admission for cohort 1 was 9.9 days (95% confidence interval [CI] 6.4-13.3 days), while length of hospital admission for cohort 2 was 7.1 days (95% CI 6.3-7.9 days; Figure 1). This decrease was significant (ANOVA, P = .021; see Table 2 for this and the following results).
Hospital Length of Stay, Number of Intensive Care Unit (ICU) Admissions, Length of ICU Stay, and Per-Patient Costs of Hospital Admission All Decreased After Implementation of the Hip Fracture Protocol.
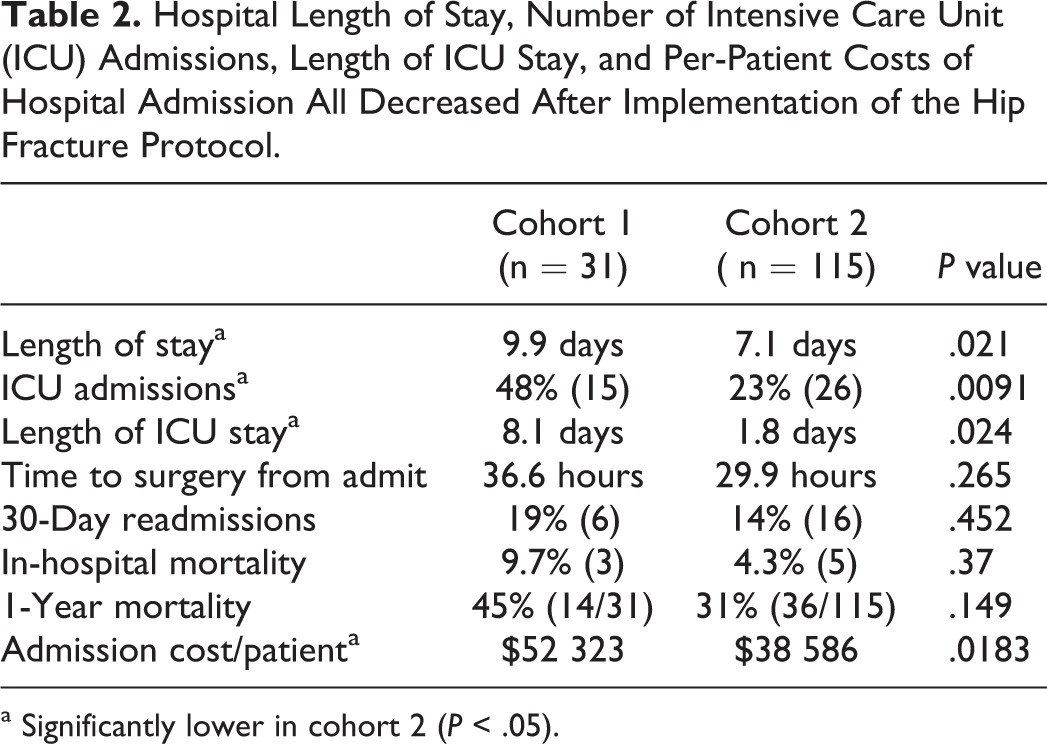
a Significantly lower in cohort 2 (P < .05).
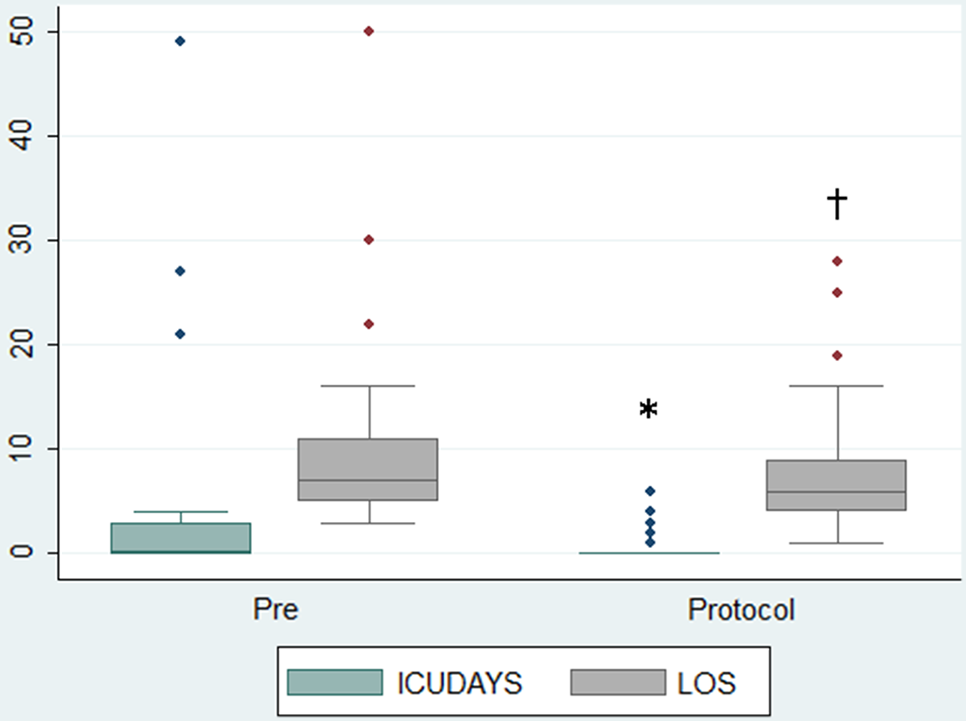
Box and whisker plot of intensive care unit (ICU) days and hospital lengths of stay (LOS, in days) for patients with hip fracture preprotocol (“pre”, cohort 1) and after protocol implementation (“protocol”, cohort 2). Median, upper median, and lower median values are plotted with standard deviation bars. Outliers are indicated by dots. Hospital ICU stays and total LOS decreased significantly after implementation of protocol. Analysis of variance,*P = .024, †P = .021.
The number of patients requiring admission to the ICU decreased significantly from 48% (15 of 31) in cohort 1 to 23% (26 of 115) in cohort 2 (χ2, P = .0091). For those patients requiring ICU admission, the average length of stay in the ICU decreased significantly from 8.1 days (95% CI 0.5-15.7 days) in cohort 1 to 1.8 days (95% CI 1.3-2.3 days) in cohort 2 (ANOVA, P = .024; Figure 1).
In-hospital mortality declined slightly from 9.7% (3 of 31) in cohort 1 to 4.3% (5 of 115) in cohort 2. However, this did not reach statistical significance with the numbers available (Fisher exact test, P = .37). One-year mortality trended downward, from 45% (14 of 31) in cohort 1 to 31% (36 of 115) in cohort 2 (χ2, P = .149). The 30-day readmission rates to our institution did not appear to change between cohorts (cohort 1: 6 of 31 [19%]; cohort 2: 16 of 115 [14%], χ2, P = .452).
Time from admission to the OR was tracked but did not vary significantly between cohorts 1 and 2. In cohort 1, 72% of the patients arrived to the OR within 48 hours of hospital admission. This increased to 87% for cohort 2. However, this difference did not reach statistical significance (χ2, P = .1875). Average time from patient admission to surgical repair decreased from 36.6 hours (95% CI 22.9-50.4 hours) for cohort 1 patients to 29.5 hours (95% CI 23.93-34.97 hours) for cohort 2 patients, although this also did not reach statistical significance (ANOVA, P = .265).
Per-patient hospital charges decreased significantly after implementation of the hip fracture protocol, from US$52 323 per patient (95% CI US$31 641-US$77 006) in cohort 1 to US$38 586 (95% CI US$35 210-US$41 963) in cohort 2 (t test, P = .0183). On an annualized basis, with 57.5 hip fracture admissions per year to our institution (the mean for cohort 2), this represents a decrease in total hospital charges of nearly US$780 000.
Discussion
Our institution has successfully implemented an interdisciplinary protocol for elderly patients with hip fracture. We were able to demonstrate a trend toward decreased time between admission and surgery as well as significant decreases in hospital lengths of stay, ICU admissions, ICU lengths of stay for patients requiring ICU admission, and costs of hospitalization after implementation of the hip fracture protocol. The 1-year mortality rates for elderly patients with hip fracture were also noted to trend downward with the numbers available.
An additional advantage of the interdisciplinary approach to management of geriatric patient with hip fracture at our institution was a large degree of cooperation and communication between multiple medical services. The hip fracture protocol team meets on a monthly basis to discuss and improve implementation of the protocol. The team, currently directed by a geriatrician in the Department of Community and Family Medicine (D.R.M.), meets on a monthly basis and includes members of the Departments of Community and Family Medicine, Internal Medicine, Orthopedic Surgery, Anesthesia, Emergency Medicine, Nursing, Rehabilitation Services, and the OCE. Unlike some other published models of geriatric hip fracture care, 15,22 our institution had the participation of family practitioners in the direct delivery of care to the patients with hip fracture; we have noted that participation of family practitioners appears to be as effective as that of internists in this model of care delivery. Interestingly, as the hip fracture protocol continued, it was anecdotally noted that requests for preoperative dobutamine stress echocardiography (which rose in frequency after protocol implementation) decreased in frequency substantially once it was recognized that optimization of patients for transportation to the OR was a priority. Stress echocardiography is now only ordered if a change in patient management was expected based upon the test results. 23
Models of interdisciplinary care of geriatric patients with hip fracture already exist in some locations. 24,25 In Australia, one group noted that interdisciplinary care of patients with hip fractures had reduced hospital lengths of stay without an increase in the complication rate. 11 In Great Britain, another group noted that a care pathway for elderly patients with femoral neck fracture resulted in improved clinical outcomes. 12 In the United States, few publications have focused upon the effectiveness of an interdisciplinary geriatric hip fracture protocol. The report of a clinical pathway and experience from the Hospital for Joint Diseases in New York revealed improvements in patient outcomes. 10 A more recent study from Johns Hopkins noted that an interdisciplinary hip fracture service resulted in shorter hospital stays, fewer complications, and more expeditious surgery for a cohort of geriatric patients with hip fracture as compared to a cohort of patients treated prior to implementation of the service. 22
The University of Rochester (New York) has been very successful with a comanagement program for elderly patients with hip fractures and has demonstrated that protocol-driven care decreases hospital lengths of stay, readmission rates, complications, hospital costs, and mortality rates for these patients. 15,23,26,27 At our institution, after protocol implementation, we demonstrated a reduction in average hospital charges to 73.6% of that seen preimplementation; this is similar to that published by the University of Rochester group which demonstrated costs of 66.7% of the national average for care of elderly patients with hip fracture after establishment of their protocol. 27
Although this study illustrates the effectiveness of an interdisciplinary protocol for the management of geriatric patients with hip fracture, there are some weaknesses. First, the retrospective nature of the data collection is a weakness. However, this project was initiated as a quality improvement project at our institution, and therefore comparison to historical controls is of great interest. Second, the implementation date of the hip fracture protocol (July 1, 2005) also coincided with the arrival at our institution of 2 fellowship-trained orthopedic trauma surgeons (G.J.D.R. and B.D.C., September 1, 2005), after a period of time when orthopedic trauma surgical coverage was provided by orthopedic surgeons whose primary interests were outside of fracture care. Prior to hip fracture protocol implementation, hip fracture surgery was performed by the on call surgeon who had admitting responsibility for the patient, while after protocol implementation, the 2 orthopedic trauma surgeons performed the bulk of hip fracture surgeries. This may have resulted in increased numbers of referrals to our institution and perhaps would have resulted in more aggressive care of patients with hip fracture, even had the hip fracture protocol never been developed or implemented, and may partially explain the dramatic increase in hip fracture admissions per year (31 in the first year, average of 57.5 per year in the subsequent 2 years). Also, the small sample size (31 in the first group and 115 in the comparison group) has resulted in a study that is underpowered for the detection of differences or similarities between the groups. A power analysis of the primary outcome measures (hospital length of stay and 1-year mortality) revealed power of 0.36 and 0.25, respectively, to accept the conclusions drawn. As we have multiple outliers in these patient cohorts, we believe that the 95% CIs provided may give a better indication of similarities and differences between the cohorts.
We were unable to show a decrease in 30-day readmission rates to our institution. However, as our institution is a regional trauma center, and we receive referrals from a large rural area, it is possible that patients with hip fracture who required readmission to the hospital within 30 days of discharge were admitted to a different institution. Therefore, we potentially have not captured all 30-day readmission events for these cohorts of patients.
The 1-year mortality rates after hip fracture trended lower after implementation of the hip fracture protocol at our institution, although the difference was not statistically significant. It is possible that a larger patient cohort size would have revealed a significant difference between the cohorts. Nevertheless, even after protocol implementation, nearly 1 in 3 elderly patients with hip fracture died within 1 year of injury. Although this mortality rate is consistent with published rates in the literature, 6,28 it is still rather high. One factor that may play a causative role in this statistic is that our institution serves as a regional trauma center. The bulk of our patients with fracture are referred from outside facilities. Many of our patients with hip fracture are from outside of the immediate vicinity of our center. Perhaps these patients are sicker at baseline than other elderly patients with hip fracture who remain at the initial centers to which they presented. It is possible that our patients are transferred to us because they are “too sick” for care at smaller, surrounding medical centers and therefore have a higher risk of early mortality secondary to their baseline frailties. Our in-hospital mortality rate of 4.3% after protocol implementation is comparable to rates in other published reports of in-hospital mortality for elderly patients with hip fracture after implementation of a hip fracture protocol (3%-17.6%). 29 –31
Although the hospital course for our patients with hip fracture protocol was shorter, time to surgery was shorter, and costs were lower, substantial improvements in 1-year mortality rates were not realized and are still desirable. Perhaps this points to a need for protocol-driven postdischarge care for frail elderly patients with hip fractures. This could involve evaluation and management protocols for osteoporosis and more careful interdisciplinary collaboration in the community for these patients.
In conclusion, development of the hip fracture protocol at our institution resulted in the establishment of an interdisciplinary care protocol for elderly patients with hip fracture. It resulted in a reduced requirement for patient admission to the intensive care unit, decreased lengths of stay for patients in the hospital and in the ICU, and decreased hospital charges per patient.
Footnotes
Authors’ Note
This research was presented in podium format at the 2012 AO North America Challenges in Fracture Care Across Disciplines meeting, Orlando, Florida, February 2012, the annual meeting of the American Academy of Orthopaedic Surgeons, San Diego, California, February 2011, and in poster format at the annual meeting of the Orthopaedic Trauma Association, Baltimore, Maryland, October 2010.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Della Rocca has received research support from Synthes, Sonoma, Stryker, Smith & Nephew, Kinetic Concepts Inc, Medtronic, and Wound Care Technologies, is a paid consultant for Synthes, and is a minority shareholder at Amedica and The Orthopaedic Implant Company. Dr Crist has received research support from Synthes, Sonoma, Medtronic, and Wound Care Technologies, is a paid consultant for Synthes, and is a minority shareholder at Amedica and The Orthopaedic Implant Company. Dr Stannard has received research support from Synthes, royalties from Thieme, is a member of the speakers’ board for Kinetic Concepts Inc and Medtronic, and is a paid consultant for Kinetic Concepts Inc and Medtronic.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Donald W. Reynolds Foundation.