
Abstract
The objective of this study was to compare a cohort of geriatric patients with operatively managed isolated fractures below the hip to a cohort of geriatric patients with operatively managed isolated hip fractures. All patients greater than 59 years of age admitted to our institution for surgical care of an isolated lower extremity fracture during a 3-year period were included. Patients were divided into 2 cohorts: BTH (fracture below the subtrochanteric region of the femur) and HIP (proximal femoral fracture at subtrochanteric region or proximal). We identified 141 patients included in cohort BTH and 205 patients included in cohort HIP. HIP patients were older (P < .01) and less obese (P < .01) but were otherwise very similar. An extensive comorbidity review revealed that the 2 cohorts were similar, with the exception of an increased incidence of dementia (P = .012) or glaucoma (P = .04) in HIP patients and of peripheral neuropathy (P = .014) in BTH patients. HIP patients were more likely to be under active antiosteoporotic medication management and were more likely to be receiving pharmacological anticoagulation at the time of admission. HIP patients and BTH patients were similar with regard to necessity of assistance with ambulation preinjury, but HIP patients were less likely to reside independently at home than were BTH patients (P < .001). HIP patients were also less likely to be discharged directly home from the hospital (P < .001). Geriatric patients with fractures below the hip are medically similar to geriatric patients with hip fracture. Medical comanagement protocols have been extensively published that improve care of geriatric patients with hip fracture; consideration should be given to similar protocol-driven medical comanagement programs for geriatric patients with fractures below the hip.
Introduction
Lower extremity fractures below the hip region are a major, yet understudied, cause of morbidity and disability for geriatric patients. Osteoporosis, common in geriatric individuals, affects all bones in the body. 1,2 Fractures of the hip, vertebrae, and distal radius (wrist) are commonly referred to as “fractures of fragility.” 3 However, patients with osteoporosis also sustain other fractures of the arms, legs, and pelvis. 4 -7 It could be said that fractures of the legs may be more disabling to the geriatric patient than hip fractures, due to the fact that rehabilitation of such “below-the-hip” fractures often requires weight-bearing restriction on the injured lower extremity (unlike after hip fracture repair); patients therefore require assistive devices, such as a walker or crutches, for ambulation. 8,9 Since many geriatric patients may lack sufficient upper body strength for routine use of walker or crutches, their mobility may be dramatically curtailed by a weight-bearing restriction on 1 or both legs. 8 Fractures below the hip are common in patients with osteoporosis and may represent an important and growing problem for the elderly population.
Geriatric patients with fractures below the hip face numerous challenges. Often, geriatric patients with lower extremity fractures have preexisting comorbidities that may have predisposed them to the fall that caused the fracture: dehydration, chronic urinary tract infection, dementia, and disequilibrium due to polypharmacy or other factors. 10,11 These comorbidities need optimization prior to and after surgical repair of the fractures, and may increase the risk of morbidity and mortality associated with the surgical repair.
Substantial attention has been given to treatment of geriatric patients with hip fractures. It is recognized that these patients have substantial preexisting comorbid conditions, and early involvement of geriatric services in their care has proven beneficial. Comanagement protocols have been developed at multiple centers internationally, which have resulted in expeditious hip fracture care and improved short- and long-term outcomes for the geriatric patient with hip fracture. 12 -15 At our institution, we have successfully implemented a hip fracture comanagement protocol, which has resulted in decreased times to the operating room from patient admission, decreased hospital lengths of stay, decreased requirement for postoperative intensive care unit admission, and decreased costs associated with hospitalization for geriatric patients with hip fracture. 16
The objectives of this study were (1) to characterize a population of geriatric patients with lower extremity fractures below the hip region and (2) to compare them with an age-matched population of geriatric patients with hip fracture. Our hypothesis was that the cohorts would be very similar with regard to comorbidities, preinjury ambulatory status, and preinjury living status.
Materials and Methods
After approval by our institutional review board, we performed a review of hospital diagnosis records to identify all patients 60 years of age or older who were admitted with an isolated, operatively managed hip fracture or an isolated, operatively managed lower extremity fracture below the hip (femoral shaft down to and including foot) during a 3-year period (September 1, 2005 to August 31, 2008). An age cutoff of 60 years was chosen based upon our institution’s hip fracture protocol inclusion criteria, the results of which have been previously published. 16 These records were then cross-referenced with departmental billing records using Current Procedural Terminology codes. Hip fractures were defined as any fracture of the proximal femur, and below-the-hip fractures were defined as fractures below the subtrochanteric region of the femur. Patients were excluded if they had concomitant head, neck, chest, abdominal, pelvic, or upper extremity injuries (besides simple contusions or lacerations). Patients were also excluded if they were admitted to our hospital’s acute care surgery service, normally reserved for patients sustaining injuries via high-energy mechanisms (such as motor vehicle crashes or falls from a ladder). Cohort HIP represented patients with isolated hip fractures, and cohort BTH represented patients with isolated below-the-hip fractures.
We performed a medical record review for all patients in both cohorts. Two authors (HSU and MEC) collected basic demographic information (sex, age, and body mass index [BMI]). All preexisting comorbidities, as specified in the patient’s electronic medical record, were recorded for each patient. A Charlson comorbidity index was calculated for each patient. 17 The mechanism of injury for each patient was also recorded. Other data points recorded included preinjury ambulatory status (ie, use of ambulatory aids), preinjury domicile (ie, assisted vs unassisted living), discharge destination and use of ambulatory aids, and preinjury use of anticoagulants or antiosteoporosis medications.
Both cohorts were individually pooled. Differences in proportions of comorbidity profiles and sex distribution between cohorts were compared using a chi-square (χ2) test. Continuous data (eg, age, BMI, and Charlson comorbidity index) for both cohorts were compared using a 2-tailed Student t test. Proportions for categorical data (eg, preinjury ambulatory status and hospital discharge destination) were compared between cohorts utilizing a Pearson χ2 test. Significance level was set at P < .05. A prestudy power analysis was performed to determine sample size for each cohort based on data for Charlson comorbidity index in similar patient cohorts and resulted in a requirement of n = 112 per cohort. Medical record review using a priori inclusion and exclusion criteria resulted in cohort populations that exceeded this requirement.
Results
We identified 141 patients with below-the-hip fractures, which represented cohort BTH, and 205 patients with hip fractures, which represented cohort HIP. In cohort BTH, patients sustained fractures of the femoral shaft (24), distal femur (23), patella (4), tibia (35), ankle (48), or foot (7). In cohort HIP, patients sustained fractures of the femoral neck (96), intertrochanteric region of the femur (95), or subtrochanteric region of the femur (13). In all, 20 BTH patients and 7 HIP patients were found down with unknown injury mechanisms, and the remaining patients were injured in falls. Female patients predominated and represented similar percentages of both cohorts: 94 (67%) of the 141 in the BTH group and 144 (70%; P = .48) of the 205 in the HIP group. Patients in the HIP cohort (mean 80.0 years, range 62-99) were older than BTH patients (mean 72.3 years, range 60-101; P < .01). Patients in the BTH cohort (mean BMI 30.5, σ = 7.9) were more obese than those in the HIP cohort (mean BMI 25.8, σ = 6.8; P < .01).
Patients with hip fracture were more likely to have dementia (P = .012) or glaucoma (P = .04) than BTH patients, but BTH patients were more likely to have peripheral neuropathy (P = .014) than HIP patients. The cohorts were similar (P > .05) for all other comorbidities examined. The mean Charlson comorbidity index for the BTH cohort (5.34) was lower than the mean for the HIP cohort (6.19; P < .01). These results are shown in Table 1. Patients with hip fracture were also more likely to be on various medications for treatment of osteoporosis than were BTH patients: alendronate (P < .01), vitamin D (P < .01), risedronate (P = .01), ibandronate (P = .02), and/or calcium supplementation (P < .01). Patients with hip fracture were also more likely to be on chronic anticoagulation with warfarin prior to injury than were BTH patients (P < .01). These results are shown in Table 2.
Patient Populations Were Medically Similar in Both Cohorts.
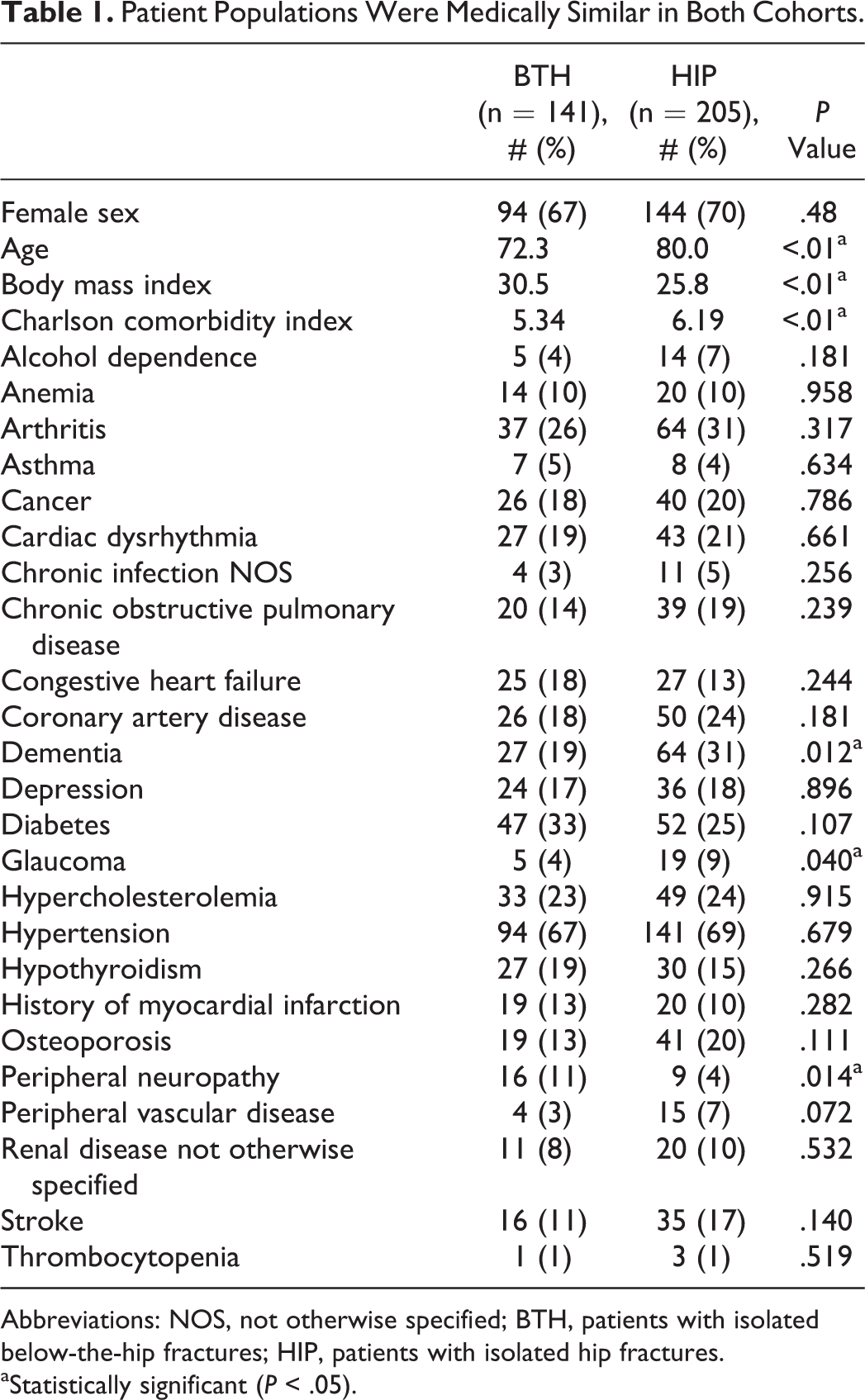
Abbreviations: NOS, not otherwise specified; BTH, patients with isolated below-the-hip fractures; HIP, patients with isolated hip fractures.
aStatistically significant (P < .05).
HIP Patients Were More Likely Than BTH Patients to be Receiving Medications to Treat Osteoporosis or for Anticoagulation at the Time of Hospital Admission (χ2 Analysis).

Abbreviations: χ2, chi-square; BTH, patients with isolated below-the-hip fractures; HIP, patients with isolated hip fractures.
aStatistically significant (P < .05).
bAntiosteoporosis therapy total does not include estrogen replacement, calcium supplementation, or vitamin D supplementation, as it could not be determined whether these agents were specifically prescribed for osteoporosis management.
Patients with hip fracture (98 of 205, 48%) were as likely as BTH patients (61 of 141, 43%) to have used ambulatory assistance (wheelchair, cane, walker, or crutches) prior to their injuries (P = .39). Patients with hip fracture (52 of 205, 25%) were also as likely to require personal assistance for ambulation prior to their injuries as were BTH patients (26 of 141, 18%; P = .123). However, HIP patients were less likely to reside independently at home (128 of 205, 62%) than were BTH patients (114 of 141, 80%) prior to injury (P < .001), and HIP patients (26 of 205, 13%) were less likely to be discharged to home than BTH patients (55 of 141, 39%; P < .001). Upon discharge, both populations had substantial increases in their requirements for ambulatory assistive devices (wheelchair, cane, walker, or crutches), although HIP patients were more likely than BTH patients to require them: 91% of BTH patients (99 of 109 recorded) and 97% of HIP patients (187 of 192 recorded; P = .024). However, discharge weight-bearing restrictions on the operative limb were ordered significantly more often for BTH patients (94%, 132 of 141) than for HIP patients (18%, 37 of 205; P < .001).
Discussion
The data that we present demonstrate that geriatric patients with isolated lower extremity fractures below the hip are similar to geriatric patients who sustain isolated hip fractures. The patients have multiple preexisting medical comorbidities and often do not live or ambulate independently. Although the Charlson comorbidity index is approximately 1 point higher in the hip fracture patient cohort, that cohort is also approximately 8 years older than the BTH cohort (each decade of life past the age of 40 equals 1 point on the Charlson scale). Traditionally, nonhip lower extremity fractures are not routinely thought of as “fractures of fragility” or signs of frailty. Perhaps this needs to be reconsidered.
Perioperative mortality rates have been shown to increase after lower extremity fracture in geriatric patients with comorbidities. Geriatric patients with heart failure, dementia, metastatic disease, and renal failure have a higher mortality rate after distal femur fracture than patients without those diagnoses in a retrospective cohort study. 18 The same study revealed that the mortality rate for geriatric patients with distal femur fracture was similar to that for geriatric patients with hip fracture. Geriatric patients with periprosthetic fractures of the femur about total hip arthroplasty stems have similar 1-year mortality rates as geriatric patients with hip fracture. 19 Increased 30-day and 1-year mortality rates are associated with increasing age after isolated femur or tibia fracture in a large 4-year retrospective cohort from a busy trauma center in the United Kingdom. 20 Mortality at 120 days in geriatric (>80 years of age) and “very geriatric” (>90 years of age) patients with nonhip fractures was equal to that in patients with hip fracture of matched ages in another large cohort series. 21
Geriatric patients with fractures below the hip can expect to lose a degree of independence upon discharge from the hospital, based upon our results. There was a substantial increase in the need for ambulatory assistance in both cohorts of patients at the time of hospital discharge, relative to their prefracture conditions. This makes intuitive sense; often, weight-bearing restrictions are imposed on patients with below-the-hip fracture after surgical repair of their injuries. Patients with hip fracture, on the other hand, are often allowed to weight bear to tolerance on their repaired hips (despite their noted need for ambulatory assist devices at discharge in our cohort). 22 Geriatric and frail patients may have difficulty managing assistive devices on their own, due to lack of upper body strength, so it is unsurprising that increased assistance may be required for these individuals after a lower extremity fracture that requires a period of restricted weight bearing. Counseling of geriatric patients with lower extremity fractures (and their families) regarding this potential loss of independence would seem appropriate.
We noted a higher average BMI in the BTH group than in the HIP group. This is an interesting finding, which is similar to prior published literature comparing geriatric patients with hip and nonhip lower extremity fractures. 18 Perhaps, patients with higher BMI are simply less likely to have fractures of the proximal femur. This trend has been noted in multiple other studies. 23,24
HIP patients were noted to be more likely to be treated with antiosteoporosis medications or anticoagulants than were BTH patients. It is possible that this is due to the more advanced age (8 years greater, on average) of the HIP patient cohort, and that this results in more frequent visits for these patients to their primary care physicians and/or specialists than occurs with BTH patients, who are younger.
This study has some limitations. First, it represents a retrospective study. Nevertheless, it is difficult to know how a prospectively gathered data set would improve data collection for the questions being asked here, unless there are deficiencies in either the medical record or the billing and coding databases at our institution. Second, the study represents a review of hospital and departmental coding and billing data (as just mentioned). The material presented here, therefore, can only be as reliable as the database from which the data were culled. Third, we do not have information about long-term outcomes of these patients. However, the purpose of the study was to examine 2 different geriatric fracture patient cohorts and to compare them. Geriatric hip fractures have received tremendous amounts of attention in the literature, and it would appear that geriatric patients with other lower extremity fractures may benefit from further in-depth study. Fourth, dementia is known to correlate strongly with poor outcomes; the HIP cohort had a higher rate of dementia than the BTH cohort, and the specific effect of this dementia on ultimate outcomes for these patients was not assessed.
Comanaged care for geriatric patients with hip fracture, in which (at least) geriatric and orthopedic services work together to optimize the outcome of the patients, has been extensively studied. 12 -16 The University of Rochester (New York) has clearly demonstrated that coordinated care between multiple services, including geriatrics and orthopedics, results in expedited hip fracture patient care, reduced perioperative complications, and reduced costs of care. 12,25,26 If geriatric patients with hip fracture are similar to geriatric patients with lower extremity fractures below the hip, then perhaps coordinated care between orthopedic surgeons and geriatric services would also be beneficial for the latter group.
Our study demonstrates that geriatric patients with lower extremity fractures below the hip are medically similar to (although as not exactly the same as) geriatric patients with hip fracture. They face similar hospital discharge problems (ambulation with assistance and decreased independence). Perhaps this information can be used to improve perioperative management of geriatric patients with all lower extremity fractures and to inform patients and families about postoperative expectations. Consideration for a comanagement protocol for geriatric patients with any lower extremity fracture requiring operative intervention may be worthwhile, considering the success of said protocols for geriatric patients with hip fracture.
Footnotes
Acknowledgments
The authors acknowledge Kathryn M. Watson, MD, who participated in data collection for this project and James L. Cook, DVM, PhD, for assistance with statistical analysis.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Gregory J. Della Rocca: Research support (Sonoma, Synthes, Wound Care Technologies), consulting (Synthes, Bioventus, LifeNet), minority shareholder (The Orthopaedic Implant Company, Amedica, Mergenet). Brett D. Crist: Research support (Sonoma, Synthes, Wound Care Technologies), consulting (Kinetic Concepts, Inc.), minority shareholder (The Orthopaedic Implant Company, Amedica), speakers’ bureau (Sonoma, Medtronic).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from the Orthopaedic Trauma Association.