
Abstract
Geriatric hip fractures are a challenging clinical problem throughout the world. Hip fracture services have been shown to shorten time to surgery, decrease the cost of admissions, and improve the outcomes. We instituted a geriatric hip fracture program for comanagement of these injuries by orthopedic and internal medicine teams at our hospital in India. From January 2010 till December 2011, 119 patients with a femoral neck fracture were treated with cemented modular hemiarthroplasty under this program using a cost-effective Indian implant. The cohort included 63 males and 56 females with a mean age of 70.7 years (range 55-98 years). Hypertension (n = 42) and diabetes mellitus (n = 29) were the most common comorbidities. The follow-up period ranged from 12 to 37 months with an average of 24 months. The surgery was performed within 24 hours of admission in 60.5% (n = 72) patients. The use of antiplatelet drugs was the most common reason for delay of surgery. The mean length of hospital stay was 10.4 days (range 3-24 days) with 77% (n = 92) of patients discharged within 1 week of admission. On follow-up, good to excellent Harris hip scores were seen in 88% of patients with 76% of patients returning to the preinjury ambulatory status. The mortality rate was 6% at 6 months follow-up and 10.9% at 2 years. Our study shows that a hip fracture program can be instituted in India. The program helped us in achieving the goal of early surgery, mobilization, and discharge from hospital with decreased mortality.
Introduction
In India, the population is aging, and osteoporotic hip fractures are a growing problem. Vitamin D deficiency and hip fractures are common in patients older than 55 years. 1 -3 Treatment of hip fractures in India remains a challenge due to cost, reluctance to have surgery, and treatment by local bonesetters. These factors make surgical repair challenging especially in a timely fashion. In particular, displaced hip fractures do very poorly without surgery. 4 Time to surgical repair has been shown in the United States and England to be an important factor in decreasing surgical morbidity and mortality. 5 Standardization of perioperative protocols and the use of a hip fracture service have been shown to improve surgical quality measures and outcomes. 6
For the majority of elderly patients with displaced femoral neck fractures, a primary arthroplasty (either hemiarthroplasty [unipolar or bipolar] or total hip arthroplasty [THA]) is the preferred option of treatment. The advantages of hemiarthroplasty over THA include lower dislocation rates, less invasive surgery, and lower costs. Limited literature is available on the treatment of femoral neck fractures in the Indian population. 7 -10 In the Indian population, dislocation is of special concern due to the use of stand-up toilet that involves a high hip angle. With cost a major issue, less expensive cemented bipolar arthroplasty prostheses have been developed by local manufacturers. We have developed a comprehensive geriatric hip fracture program in order to improve the results of patients with these injuries keeping in mind the specific features and demands of our patient population. The goal of our study is to report the results of a geriatric hip fracture program instituted in India for displaced femoral neck fractures.
Materials and Methods
This study is an analysis of a cohort of patients undergoing cemented bipolar hemiarthroplasty for femoral neck fracture performed at our hospital from January 2010 to December 2011. A total of 148 elderly patients presented to our hospital with a femoral neck fracture during the study period. Of these, 9 patients had undisplaced or valgus impacted fractures, 7 patients had previous internal fixation, 4 patients had a history of tuberculosis of the hip, and 9 patients had severe cognitive impairment. These 29 patients were excluded from the study. Our final study group included 119 patients with a mean age of 70.7 years (range 55-98 years). There were 63 males and 56 females (53:47). In India, the average life expectancy is 66 years as compared with 79 years and 82 years of United States and United Kingdom, respectively. 11 The exact date of birth is often not available for many patients so we included all patients who were above the chronological or physiological age of 55 years.
Our center is a 1400-bedded tertiary care hospital attached to a medical school and is located in a city in northwest India in the Punjab province with a population of approximately 3.5 million people. With the goal of improving hip fracture care, a comprehensive geriatric hip fracture program was instituted in June 2009. The Departments of Orthopedics and Internal Medicine worked together to formulate a treatment algorithm for geriatric hip fractures for our institution. The program was modeled after the hip fracture program at the University of Rochester. 12 The Departments of Anesthesia, Physical therapy, and Nursing were sensitized to the special needs and protocols of this program. A section of a high dependency unit that is managed by internal medicine team was designated for the care of our elderly patients with hip fracture. The emphasis of our program was on the following points: (1) rapid optimization of patients before surgery, (2) early surgical stabilization, (3) combined management of patients by orthopedic surgeons and internal medicine specialists, and (4) aggressive physical therapy protocol with prophylaxis for venous thromboembolism (VTE). 13 The present study was approved by the institutional ethics committee.
Elderly patients with suspected hip fractures were admitted through the emergency department and evaluated by both the orthopedic and internal medicine teams. Following radiological confirmation of hip fracture, a detailed clinical evaluation was performed, comorbid conditions were recorded, and laboratory investigations were requested. A member of the anesthesia team evaluated the patient in the emergency area to assist with optimization of the patient. Subspecialty consult, for example, cardiology, nephrology, or neurology, was sought if requested by the internal medicine or anesthesia teams.
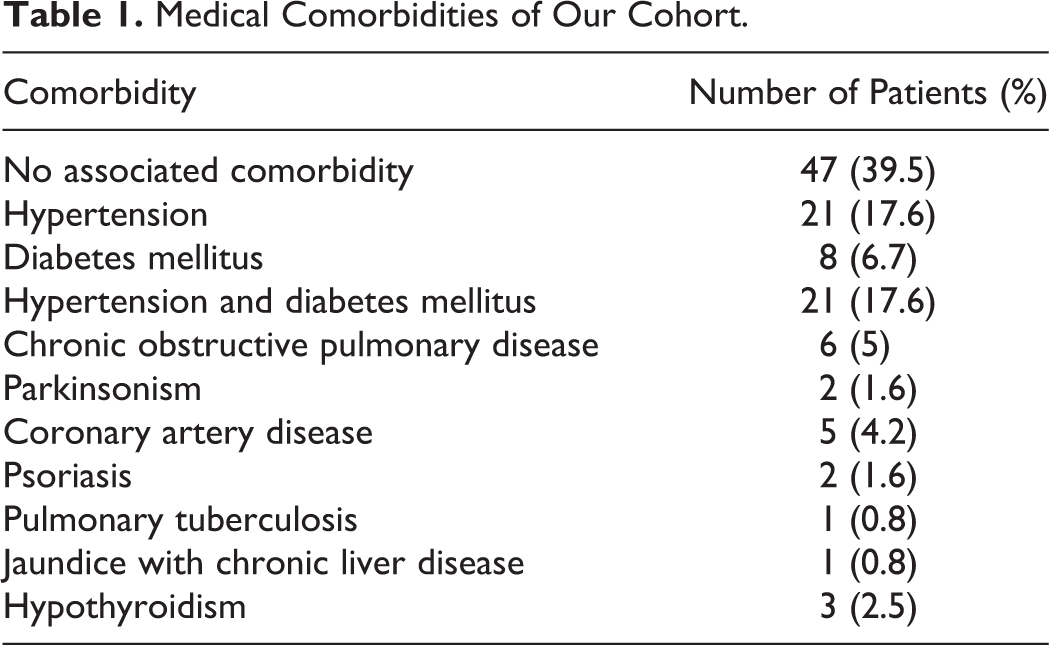
As the specialty of geriatric medicine does not exist at our institution, the internal medicine specialists are well experienced in managing the geriatric population. The team from internal medicine first optimized the patients prior to surgical repair. The common comorbid conditions resulting in delay were uncontrolled hypertension, uncontrolled diabetes mellitus, poor chest condition, and the use of antiplatelet drugs. The surgery was not delayed for intake of aspirin alone as an antiplatelet agent. In all, 94% (n = 112) of the patients had low energy trauma such as a fall at home. Hypertension (n = 42) and diabetes mellitus (n = 29) were the most common associated comorbidities, with 34 patients having more than 1 comorbid medical condition. The distribution of medical morbidities is given in Table 1. There was often delay prior to presentation at the hospital. In all, 41% (n = 49) of the patients presented to us within 24 hours of the injury and 91.5% (n = 109) patients were hospitalized within a week of the injury.
Medical Comorbidities of Our Cohort.
The surgical treatment protocol for femoral neck fractures was standardized by our team of orthopedic surgeons. Internal fixation with cannulated screws was performed for undisplaced and valgus impacted fractures as well as in the frail elderly patients with poor cognitive function (mini mental test <7) or multiple comorbidities who were considered poor candidates for hip arthroplasty. Patients with displaced femoral neck fractures were treated with cemented modular bipolar arthroplasty (Endopro-M; Ormed Medical Technology Limited, Bengaluru, India).
All surgeries were performed under spinal/epidural anesthesia by 1 of the 6 treating surgeons. The choice of approach (modified Hardinge or posterior) depended on the treating surgeon. The modified Hardinge approach was used in 81% (n = 97) of patients and the posterior approach in the other 22 patients. All cases were either performed or assisted by an attending orthopedic surgeon. Cement was prepared by hand mixing without vacuum and was pressurized with a cement gun and a cement restrictor. Preoperatively, patients received Cefuroxime (1.5 g intravenously [iv]) followed by 750 mg iv every 8 hours for 48 hours in the postoperative phase. Other antibiotics were added as advised by the physician team for comorbidities like chest infection, urinary tract infection, and so on.
The patient remained in the postoperative ward manned by the anesthesia team for the first 2 to 4 hours after the surgical procedure. Subsequently, stable patients were shifted to an orthopedic ward where they were visited daily by the internal medicine team (n = 89). The patients who required active medical management were shifted to a high dependency unit managed by internal medicine team and after stabilization, they were transferred to the orthopedic ward (n = 30). For deep venous thrombosis (DVT) prophylaxis, enoxaparin sodium 40 mg subcutaneously (Clexane; Sanofi Winthrop [Sanofi India Limited, Thane, India]) once a day was started 24 hours after the surgery and continued while the patient was hospitalized. The patients were discharged on 75 mg of oral aspirin once a day for 3 weeks. We did not use any mechanical devices for DVT prevention in our cohort; however, we did encourage ankle pump exercises. Anteroposterior (AP) radiograph of the hip was performed on the day of surgery with a portable X-ray machine. Further, AP and lateral radiographs are performed before discharge.
The patients were encouraged to mobilize as early as possible with a protocol of knee bending, static quadriceps exercises, and sitting on the bed. A physical therapist mobilized the patient with a walking frame after the patient was able to perform a straight leg raise without assistance. Patients operated by a posterior approach were educated in posterior hip precautions to prevent dislocation. All patients were discharged directly to home from the hospital, as the concept of nursing care center or rehabilitation center for elderly patients does not exist in our area. The patients were reviewed at a designated outpatient area for suture removal on postoperative day 12 and then at 6 weeks, 3 months, 6 months, and then at 6-month intervals.
The follow-up data were collected prospectively by one of the coauthors including local complications, Harris Hip Score, medical complications, readmission to the hospital, activity status, and use of a walking aid. The follow-up period ranged from 12 to 37 months with an average of 24 months. We were able to follow-up 88 patients with clinical and radiographic evaluation in our hospital. During the study, 13 patients died and the remaining 18 patients defaulted on follow-up. These patients were contacted by telephone through their family members. We were able to interview 14 patients regarding their activity status, walking aid, hip pain, walking distance, and limp. Four patients could not be contacted and were lost to follow-up.
Results
Time to Surgery
The surgery was performed within 24 hours in 60.5% (n = 72) of patients and 99% (n = 118) of patients underwent definitive treatment within 1 week of admission to the hospital. The delay in surgery was due to management and optimization of comorbid medical conditions including uncontrolled hypertension (n = 12), poor diabetic control (n = 10), chronic obstructive pulmonary disease exacerbation (n = 2), decompensated coronary artery disease (n = 5), or use of oral anticoagulants like clopidogrel (n = 18). The anesthesia team advised surgical delay for patients on clopidogrel after 5 days of last ingestion of tablet in view of the potential for bleeding.
Length of Stay
In all, 77% (n = 92) of our patients were discharged in the first week of hospital admission and another 18% (n = 22) were sent home within second week. The mean length of hospital stay was 10.4 days (range 3-24 days).
Functional Results
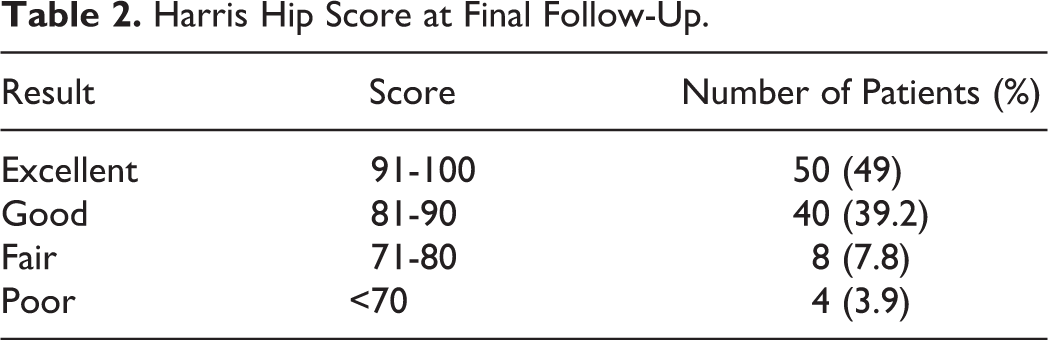
Of the 119 patients, 80% (n = 95) were community ambulators, 20 were home ambulatory, and 4 patients were bed ridden before the injury. Follow-up data were available for 102 patients of whom 76.4% (n = 78) were community ambulators with 25 patients using a cane for ambulation. Twenty patients were home bound using a walking frame and 4 were confined to bed. Postoperative Harris hip scores are shown in Table 2.
Harris Hip Score at Final Follow-Up.
Ten patients developed postoperative electrolyte imbalance of whom 3 patients had associated delirium. These were managed by internal medicine team in the high dependency unit. Three patients had posterior hip dislocation in our series, 2 following posterior approach and 1 following a lateral approach. All dislocations occurred within 3 weeks of surgery. Closed reduction under general anesthesia was successful in 2 cases. In the third patient, the modular head had disengaged from the stem so open reduction was performed and the patient had a good functional outcome. Two periprosthetic fractures (Vancouver Type B) were observed in our series and were managed by revision surgery. Two patients developed superficial surgical wound infection; both were managed with intravenous antibiotics for 2 weeks and local wound care. Decubitus ulcers were observed in 3 patients, which healed with regular dressings. We had no cases of acetabular erosion, implant loosening, or deep infection within the study period.
Mortality
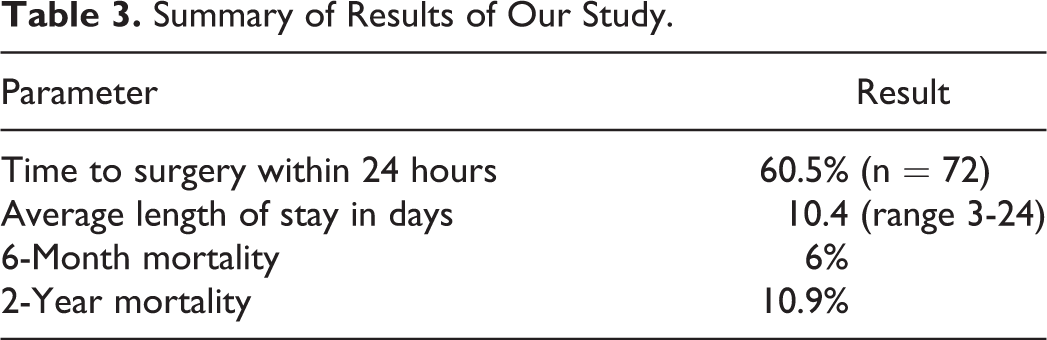
Thirteen patients died during the period of follow-up. No patients died during the index hospital admission. Three patients died within 3 weeks of surgical treatment and 4 patients within 6 months due to suspected cardiovascular events. Another 6 patients died within 2 years and the cause was not known. The results of our study are summarized in Table 3.
Summary of Results of Our Study.
Discussion
The management of femoral neck fractures in the elderly patients is improved with the use of geriatric hip fracture care protocols. We have successfully instituted these protocols in our hospital in India. In our series, 60.5% of patients were operated within 24 hours after admission and 99% were operated within 1 week. We hope to continue to improve our time to surgery in the future. One of the main reasons for delay in our study was the use of antiplatelet agents. Recent studies have shown that early surgery in patients on clopidogrel and warfarin is safe with no increase in observed complications. 14 -16 Removal of this delay would improve our time to surgery. Addition of a standardized pain management program and fracture prevention program may further improve our results.
There are many roadblocks to early surgery and shorter hospital stays in India. 9,17 About 80% of our patients were discharged from the hospital in the first week and 95% were sent home within 14 days after surgery with the length of stay being shorter as compared to other Indian studies. This is due to comprehensive geriatric care under our program and the good social support structure at home existing in our region. Marya et al and Rajak et al reported a mean length of stay of 11.9 and 15.3 days, respectively, for bipolar hemiarthroplasty in Indian patients. 7,10
Most of the elderly patients were community ambulators with low functional demands who stay with their families and are dependent upon them. These patients probably do not require the high performance of a THA. For displaced femoral neck fractures, we chose a cemented modular bipolar prosthesis, which has been widely used in India for more than 10 years. 8,9,10,18 Cemented bipolar prostheses of good quality are available from local manufacturers (eg, Ormed, INOR, etc) and are quite cost-effective as compared to THA. Moreover, there is a lack of good-quality cementless stems or THA systems manufactured locally at cheaper costs. Most of our patients do not have health insurance and have to pay for their implants directly to the hospitals. These factors make a cemented bipolar prosthesis a good choice for our patients.
The incidence of dislocation in our study is 2.5% (n = 3), which can be attributed to use of lateral approach for majority of our patients as well as exclusion of patients with severe cognitive dysfunction. A review of over 33 000 hemiarthroplasties of Swedish and Norwegian hip registries showed that posterior approach and use of uncemented stems was associated with increased reoperation rates. 19 Further, it has been suggested that bipolar prosthesis is more stable due to its self-aligning acetabular component. 20 The associated modularity also allows the surgeon to balance the soft tissues around the hip and potentially reduces the chances of hip dislocation. An interesting phenomenon noted in our study was that 50% (n = 60) of the patients started squatting to use the Indian type of water closet early after surgical repair. This was against our advice but patients have limited options regarding toilet selection and elevated toilet seats. Other Indian authors have reported the need for deep hip flexion in our population. 18 Despite the need for deep hip motion, our dislocation rate was comparable to other studies. There was no case of acetabular erosion or stem loosening in our cohort though the period of follow-up in our study is short. Other authors have documented the low rate of acetabular erosion with bipolar hemiarthroplasty. 8,9,17,21
The 6-month mortality rate in our series was 6% and 2-year mortality was 10.9% which was toward the lower end of spectrum of the rate reported by other studies (11%-27%). 22 -25 The low mortality in our series could be attributed to the relatively younger cohort with less comorbidities, early surgery with mobilization, VTE prophylaxis, and comprehensive geriatric care. Lim et al observed a raised mortality due to a delay before surgery of more than 5 days. 22
The limitations of our study include a short follow-up and lack of documentation regarding the cause of death on follow-up. Our study does not have a direct comparison group with which to compare our results.
In summary, we have instituted a pathway of care for our patients with hip fracture having femoral neck fractures. The cemented modular bipolar arthroplasty for the displaced femoral neck fractures in the elderly patients is a good choice in India as it provides early pain-free mobilization with restoration of functional status in majority of patients with minimal complications. It also helps to fulfill the functional demands and expectations of the elderly Indian population. It is cost-efficient which is of major importance to our patients. Our attempt at comprehensive geriatric fracture care helped us in achieving the goal of early surgery, mobilization, and discharge from hospital to home with added advantage of decreased mortality. We feel that institution of standardized care improved our outcomes in a health care system that is different from that in the United States or Great Britain. We hope to continue to improve our process of hip fracture care and believe that this is a viable model for other hospitals in India.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.