
Abstract
Objective
We conducted a systematic review and meta-analysis to compare post-operative rehabilitation outcomes between two common treatments in patients who have suffered an intertrochanteric hip fracture: intramedullary nails vs dynamic hip screws.
Methods
We searched MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials, and Web of Science up to August 10, 2022. The inclusion criteria were defined as Population: adults (>18 years old); Interventions/Comparators: intramedullary nails and dynamic hip screws; Outcomes: function, quality of life and survival; and Study type: randomized controlled trials and non-randomized studies. A meta-analysis was performed, and the fixed-effect model was selected to pool the data for homogeneous studies (I2 < 50%) and the random effect model was selected for heterogeneity I2>50%. The P-value of less than 0.05 was considered statistically significant. A narrative synthesis was conducted on the remaining outcomes with insufficient data (ie, missing means, or standard deviations).
Results
108 studies were included in the review. 42 studies had outcomes that were included in the meta-analysis. There were modest differences after sensitivity analysis for the Parker mobility score mean difference (MD) = 0.70, 95% CI [0.12, 1.28], T = 3.11, df = 5, P = 0.03, and Harris hip score (MD = 0.94, 95% CI [0.34, 1.54], T = 3.54, df = 9, P = 0.006) favoring the nails. There were no statistically significant differences in the Functional Independence Measure (FIM) (MD = −2.50, 95% CI [−6.46, 1.45], Z = 1.24, P = 0.22), the Barthel Index (MD = 2.66, 95% CI [−7.60, 12.92], T = 1,12, df = 2, P = 0.38), the generic quality of life (MD = 0.04, 95% CI [−0.08, 0.17], Z = 0.70, P = 0.49), the health-related quality of life (MD = −0.14, 95% CI [−3.57, 3.28], Z = 0.08, P = 0.93) or mortality (1.00, 95% CI [0.96, 1.03], Z = 0.16, P = 0.87) outcomes.
Conclusion
This review showed some differences in functional outcomes in the treatment of intertrochanteric fractures favoring intramedullary nails over dynamic hip screws. There were no differences between the groups for quality of life and mortality outcomes. The narrative synthesis showed additional outcomes that warrant further investigations.
Keywords
Background
Hip fractures are a significant medical concern worldwide, 1 with an estimated global yearly incidence of 4.5 million by 2050. 2 Intertrochanteric hip fractures typically result from trauma or falls and predominantly affect older adults because of decreased bone mineral density. 3 Currently, the most common treatment options for intertrochanteric fractures include either intramedullary nails (IMN) or a dynamic hip screw (DHS) construct. The DHS is a plate and sliding screw construct used to stabilize the fracture, which can also be referred to as a sliding hip screw or a compression hip screw. These are considered ‘dynamic’ implants as they have the capacity for sliding at the plate/screw junction to allow for collapse at the fracture site. 4 The DHS operates on the tension band principle, permitting the screw to move within the barrel, facilitating fracture compression as the patient starts to weight bear. 5 Conversely, an IMN is a metal rod inserted into the medullary cavity of a bone, spanning across the fracture to provide a more medialized construct for support of the fracture. 6 Biomechanically, the IMN is superior to the DHS. 7 Several newer IMN, including gamma nails, intramedullary hip screw, and proximal femoral nails, also facilitate dynamic movement and thus collapsing at the fracture site. 8 The DHS was considered the gold standard treatment for intertrochanteric fractures in the past,4,9 but the IMN has been a preferable form of treatment more recently. 10
Although there have been meta-analyses and systematic reviews comparing the two methods to determine the ideal implant, there have been inconsistencies in their findings. These variations may come from the diverse range of outcomes reported as studies look at parameters within perioperative outcomes and postoperative complications. Some studies have favored IMN implants when considering perioperative outcomes11–14 such as operative blood loss and operative time. Parker and Pryor’s meta-analysis showed that while many of the outcomes analyzed15–19 showed no significant difference, recipients of DHS had a reduced risk for femoral shaft fractures or reoperation rate than IMN. 20 However, no previous reviews have specifically focused on longer term (ie, 12-month post-surgery) functional outcomes, quality of life, and mortality rates for these treatment options. The overall goal was to systematically compare post-operative rehabilitation outcomes (including functional, quality of life, and survival) between two groups of IMN vs DHS fixations in the treatment of intertrochanteric fractures.
Methods
Study Design
We conducted a systematic review and meta-analysis according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines 21 and Cochrane’s Handbook for Systematic Reviews of Interventions. 22 The protocol was developed, registered in PROSPERO (CRD# CRD42022364556) and published. 23
Protocol Amendments
The review was conducted as planned, with no deviations from the registered protocol. However, due to the considerable number of outcomes found, we focused this systematic review on post-operative functional, quality of life, and survival outcomes.
Eligibility Criteria
Population
This review considered studies in adult patients (18+) with an intertrochanteric hip fracture (AO/OTA classification: type 31A).3,24–27
Interventions/Comparators
Studies comparing the effectiveness of IMN and DHS were included. IMN includes double lag screw nails, Targon nail, proximal femoral nail, long or short cephamedullary nail, gamma nail, InterTan, Profin nail, Kuntscher-Y nail, intramedullary hip screw, holland nail, and ace nail. DHS includes sliding hip screws, vari-angle hip screw, and compression hip screw. We excluded studies that evaluated uncommon methods of fixation such as ender nail, nystrom nail, Grosse-Kempf nail, Moore’s pins, transverse proximal screw, dynamic condylar screw, contralateral reverse distal femoral locking compression plate, and less invasive stabilization system. Studies that had no comparator group or that compared two nails, or two screws were also excluded.
Outcome Measures
The studies included in the review identified at least one of the following outcomes at 12-month post-surgery: functional outcomes (ie, Harris hip score, Parker mobility score, Functional Independence Measure (FIM), etc.), quality of life, and survival outcomes.
Types of Studies
We included randomized controlled trials (RCTs) and non-randomized studies (eg, cohort, case-control, controlled before-and-after, interrupted-time-series, and controlled trials not using full randomization).
Search Strategy
A systematic search strategy was conducted in MEDLINE (Ovid), EMBASE (Ovid), Cochrane Central Register of Controlled Trials (Ovid), and Web of Science from their date of inception to August 10, 2022. The search strategy was developed by an experienced health sciences librarian (MCD) and subsequently peer-reviewed by a second information specialist using the Peer Review or Electronic Search Strategies guideline. 28 The search parameters, which included terms like hip fractures, intertrochanteric fracture, dynamic, screw, bone, fixation, intramedullary, and others, were adjusted to target articles relevant to orthopedic interventions and their associated outcomes. The search strategies are described in the supplemental file #1. References were exported into Covidence (https://www.covidence.org) and duplicates were removed.
Screening and Data Extraction
Three reviewers (AL, RP and ATK) independently screened the references in a two-step approach (title and abstract, then full text) according to the eligibility criteria. Throughout the screening process, CB and SP were available to address any reviewer disagreements. This collaborative approach ensured a comprehensive evaluation of the eligibility criteria. Three reviewers (AL, RP and ATK) independently extracted and organized the data using a previously piloted data extraction sheet. The following were extracted for each included study: author, country, study design, intervention 1, intervention 2, patients (n) in each group, outcomes/results, follow-up period.
Risk of Bias Assessment
During the data extraction process, the risk of bias of the included studies was independently assessed by three authors (AL RP, ATK). The Risk of Bias 2 (RoB 2) and the Risk of Bias in Non-randomized Studies - of Interventions (ROBINS-I) were used in the assessment. RoB 2 is an updated version of the Cochrane risk-of-bias tool specifically designed for RCTs. 29 It evaluates domains such as randomization, deviations from interventions, missing outcome data, measurement of outcomes, and selection of reported results. 29 Questions are employed within each domain to determine the level of bias, classifying it as low risk, some concerns, or high risk. ROBINS-I, however, is intended for non-randomized studies comparing interventions. 30 It assesses domains such as confounding, selection bias, and measurement of interventions and outcomes. 30 Similar to RoB 2, ROBINS-I utilizes signalling questions to assign a judgment of bias within each domain such as critical risk, serious risk, moderate risk, or low risk. At the end of the quality assessment, we used Robvis, a web-based application specifically designed for visualizing risk-of-bias assessments in systematic reviews to report the findings. 31
Data Analysis
The Cochrane Review Manager 7.9.2 (RevMan Web) was used to conduct the meta-analysis.
32
For the analysis of continuous variables, we utilized the inverse variance method to calculate the mean difference (MD) along with its corresponding 95% confidence interval (CI). For the analysis of dichotomous outcomes, we employed the Mantel-Haenszel method to calculate the pooled odds ratio (OR) as well as its corresponding 95% confidence interval (CI). Heterogeneity was assessed with the I2. If, for a given outcome, there was significant heterogeneity (I2 > 50%) and the number of included studies in the analysis was
Results
Search Results
From the initial database searches, 3312 studies were identified. After duplicate records were removed by Covidence (n = 925) or manually (n = 56), the titles and abstracts were screened of the remaining studies (n = 2331) based on the inclusion criteria. A full-text review of 272 studies was completed, which identified 166 studies that did not meet the inclusion criteria and were therefore excluded. Reasons for exclusion included no comparator (n = 49), wrong outcomes (n = 39), wrong intervention (n = 30), wrong publication type (n = 23), non-English or non-French (n = 16), full text unavailable (n = 6), and wrong patient population (n = 3). All studies that did not meet the criteria are listed in Supplemental file 2 with the reason for exclusion. The remaining 106 met our inclusion criteria. Two additional studies were identified through manual citation searching, which met the inclusion criteria. Thus, 108 studies were included in the review (Figure 1). PRISMA Flowchart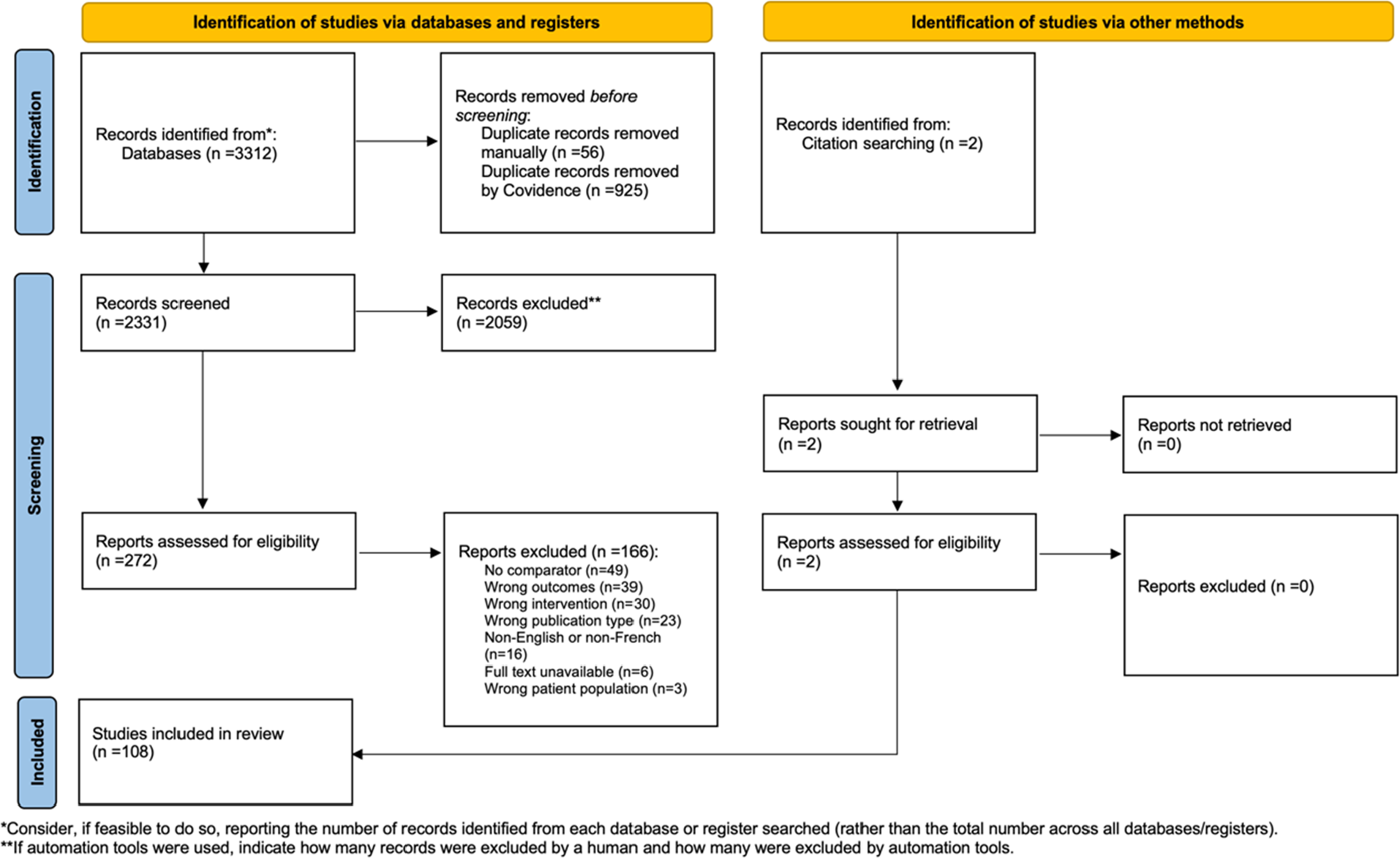
Study Characteristics
Study Characteristics (n = 108)

aStudies included in the meta-analysis (n = 42 studies).
Quality Assessment
The data bias assessment between the 52 RCTs and the 56 non-randomized studies demonstrated notable differences in methodological rigor and potential biases. In the RCTs, most of the studies (42 out of 52) were classified as having some concerns, indicating minor methodological limitations that may influence the reliability of their findings. However, a noteworthy proportion of the RCTs (8 out of 52) were deemed to have a low risk of bias, indicating robust methodological practices and providing confidence in their results’ validity. Conversely, only 2 studies were categorized as having a high risk of bias, signifying significant methodological shortcomings that may compromise the trustworthiness of their outcomes (Figure 2A). (A) Risk of Bias Summary for RCTs, (B) Risk of Bias for Non-randomized studies
The risk of bias assessment for the non-randomized studies revealed more concerning findings. Among these studies, 7 were identified as having a critical risk of bias, indicating significant methodological limitations that may affect the validity of their results. Furthermore, a notable portion of the non-randomized studies (40 out of 56) were classified as having a serious risk of bias, suggesting substantial concerns regarding the study designs and methodologies employed. Also, 9 studies were deemed to have a moderate risk of bias, indicating methodological limitations that could impact their reliability (Figure 2B).
While both RCTs and non-randomized studies were subject to risk of bias assessments, the RCTs exhibited better methodological rigor, with a lower proportion of studies categorized as having a high risk of bias. Conversely, the non-randomized studies had a higher prevalence of studies with serious and critical risk of bias, indicating more substantial methodological limitations. Most studies included in the meta-analysis presented some risk of bias.
Meta-Analysis of Outcomes at Last Follow-Up (12 Months)
In the meta-analysis, outcomes of 42 studies were included.
Functional Independence
The pooled estimate for the Functional Independence Measure (FIM), combining the results of both studies using the fixed effect model had no statistically significant difference between the two interventions (mean difference (MD) = −2.50, 95% CI [−6.46, 1.45], Z = 1.24, P = 0.22) (Figure 3A). The MD of the three studies for the Barthel Index score was 2.66, 95% CI [−7.60, 12.92], T = 1,12, df = 2, P = 0.38) using the random effect model (Figure 3B). We conducted a sensitivity analysis by excluding Tucker et al,
126
then the remaining studies were homogeneous (I2 = 23%). The results showed a MD of 4.89, 95% CI [−25.00, 34.79], T = 2.08, df = 1, P = 0.29. The MD of the seven studies for the Parker mobility score was 0.96, 95% CI [0.23, 1.69], T = 3.22, df = 6, P = 0.02 using the random effects model, indicating a slight preference for the nails (Figure 3C). The sensitivity analysis excluding Little et al,
95
shows homogeneous (I2 = 31%). Similarly, the results showed a modest preference for the nails (MD = 0.70, 95% CI [0.12, 1.28], T = 3.11, df = 5, P = 0.03). The MD for the Harris hip score was 0.70, 95% CI [−1.41, 2.80], T = 0.73, df = 11, P = 0.48. We conducted a sensitivity analysis by removing Bajpai et al
47
and Singh et al,
123
which showed homogeneous amongst the remaining studies (I2 = 0%). The results showed a slight preference for the nails (MD = 0.94, 95% CI [0.34, 1.54], T = 3.54, df = 9, P = 0.006) (Figure 3D). Forest Plots. (A) Functional Independence Measure (FIM) score, (B) Barthel Index, (C) Parker Mobility Score, (D) Harris Hip Score, (E) Generic Quality of Life (EQ-5D), (F) Health-related Quality of Life (Short Form-12 Physical Component Summary)
Quality of Life
The MD for the two studies reporting on the generic quality of life (EQ-5D) measure was 0.04, 95% CI [−0.08, 0.17], Z = 0.70, P = 0.49, using the random effect model, indicating no difference between the two intervention groups (Figure 3E). Similarly, the MD for the health-related quality of life (Short Form-12 Physical Component Summary) was −0.14, 95% CI [−3.57, 3.28], Z = 0.08, P = 0.93, showing no difference between groups (Figure 3F).
Mortality
The odds ratio (OR) for mortality at 12 months was 1.00, 95% CI [0.96, 1.03], Z = 0.16, P = 0.87, suggesting no statistically significant difference between the two intervention groups (Figure 3G).
Outcomes Not Included in Meta-Analysis
Outcomes not Included in the Meta-Analysis

Discussion
This systematic review and meta-analysis examined the effectiveness of two surgical interventions, IM nails vs DHS by comparing the outcomes of functional, quality of life, and survival during a 12-month follow-up period. The meta-analysis found no statistically significant differences in functional independence between IMN and DHS based on the FIM and the Barthel index scores. Modest significance was identified during sensitivity analyses for the Parker mobility score and the Harris hip score favoring the IMN. No significant differences were observed on the generic quality of life, health-related quality or mortality at 12 months. The outcomes excluded from the meta-analysis provided additional context. Studies reporting other functional outcomes such as movement, walking/mobility/ambulation, weightbearing status had their overall results favoring the IMN. Studies on place of care, mortality and quality of life reported no significant results.
The IMN and the DHS are both effective treatments to manage intertrochanteric fractures. For most intertrochanteric hip fractures, the DHS has an established history of successful use, demonstrates high reproducibility and is more cost-effective compared to the IMN. 143 Alternatively, the IMN is biomechanically superior 144 and inserted using less invasive surgical approaches. When comparing these two implants, the literature shows similar results with failure rates as the main outcome.145,146 There may be some advantages to the IMN when treating the “most unstable” patterns. 144
Given that the IMN is a more expensive implant, its indiscriminate use for all fractures will greatly impact the cost of treating these injuries. The use of the IMN has increased significantly over the past 20 years. 147 Despite this trend, the success rate of DHS and IMN fixation in both stable and unstable fractures have been similar in several studies.97,113 In a prospective study, Grønhaug and colleagues 76 assessed data from 17 341 patients within the Norwegian Hip Fracture Register over the period of 2013-2019 and found a significantly lower re-operation rate for IMNs, when compared to DHS for unstable fractures (31-A2 and 31-A3). However, for stable fractures (31-A1), there was no difference recorded in the re-operation rate. Although the “success” of surgery can be measured by fracture healing and/or re-operation rate, many other factors must be considered in order evaluate the overall effectiveness of these two implants. Previous research comparing the DHS and IMN for the treatment of intertrochanteric hip fractures found no significant differences in mortality,15,146,148,149 re-operation rate,145,146,148 length of stay,145,148 major complications,15,146,149 nonunion, 15 infection,15,145 mean surgical time, 145 time to healing, 145 and failure of fixation rates.145,146 However, patients with IMN fixation have demonstrated slightly less blood loss compared to those with DHS.145,146,149
This systematic review reported on functional, quality of life, and mortality outcomes found in the published literature. In addition to the meta-analysis, we included a narrative synthesis of the additional outcomes to avoid biased reporting. We found no studies looking at rehabilitation outcomes such as (eg, time to initiation of rehabilitation, rehabilitation length of stay, rehabilitation intensity/frequency, or type of rehabilitation). Further primary studies are needed to look at the effectiveness of DHS and IMN on rehabilitation outcomes for this hip fracture population.
The comparison between DHS and IMN has significant implications for policy, practice, and further research in hip fracture management. Orthopedic surgeons face the challenge of selecting the most appropriate surgical technique based on patient characteristics, fracture type, and institutional resources. While our review indicated some disparity in functional outcomes between the two methods, it is important for clinicians to weigh the comparative effectiveness data and clinical judgment when choosing between DHS and IMN for treatment. When considering research in the treatment of intertrochanteric hip fractures, it is imperative to further understand the nuances in outcomes associated with functional recovery and quality of life between DHS and IMN procedures. RCTs with larger sample sizes and longer follow-up periods, as well as prospective, multicenter studies, are needed to compare these techniques’ effectiveness in diverse patient populations. So far, research has focused more commonly on perioperative outcomes and complications and the there is a lack of research on comparing the recovery and rehabilitation needs for these patients. By ensuring that surgeons have access to the necessary equipment and training, policymakers can contribute to enhanced patient outcomes and long-term reductions in healthcare costs. 12
Strengths and Limitations
The strengths of this review include the prospective registration of the study protocol and a comprehensive search of the literature. It also incorporates a meta-analysis to assess the select outcomes. Nonetheless, it is important to acknowledge the limitations. The different 31A fractures groups and subgroups were not analyzed individually, which limited the detection of specific differences in outcomes related to fracture stability. Also, our review did not specifically exclude studies comparing IMN and DHS fixations in patients with reverse obliquity fractures (AO/OTA type A3) although some clinical guidelines150,151 recommend the specific use of IMN fixations for this more unstable pattern. Additionally, studies often did not report postoperative radiological outcomes to assess the accuracy of the surgical procedure, which may have impacted patient outcomes. Given that several studies included in our review had methodological limitations, the results should be interpreted with caution. Future studies should address these gaps and consider including postoperative radiological results to improve the comparison and evaluation of these two fixations.
Conclusion
Overall, our meta-analysis found some differences between the two fixations (IMN vs DHS) for the treatment of intertrochanteric hip fractures. Our meta-analysis revealed that IMN had modest advantages over DHS for functional outcomes. In addition, in our narrative synthesis, the IMN provided some positive results for functional outcomes. Further research on the effect of these fixations on functional rehabilitation outcomes is needed.
Supplemental Material
Supplemental Material - Comparing Intramedullary Nails versus Dynamic Hip Screws in the Treatment of Intertrochanteric Hip Fractures on Post-operative Rehabilitation Outcomes – A Systematic Review and Meta-Analysis
Supplemental Material for Comparing Intramedullary Nails versus Dynamic Hip Screws in the Treatment of Intertrochanteric Hip Fractures on Post-operative Rehabilitation Outcomes – A Systematic Review and Meta-Analysis by Chantal Backman, RN, MHA, PhD, Ashley Lam, Rosie Papp, Aurelie Tonjock Kolle, Franciely Daina Engel, Wenshan Li, Soha Shah, Colleen Webber, Peter Tanuseputro, Marie-Cecile Domecq, and Steve Papp in Geriatric Orthopaedic Surgery & Rehabilitation
Supplemental Material
Supplemental Material - Comparing Intramedullary Nails versus Dynamic Hip Screws in the Treatment of Intertrochanteric Hip Fractures on Post-operative Rehabilitation Outcomes – A Systematic Review and Meta-Analysis
Supplemental Material for Comparing Intramedullary Nails versus Dynamic Hip Screws in the Treatment of Intertrochanteric Hip Fractures on Post-operative Rehabilitation Outcomes – A Systematic Review and Meta-Analysis by Chantal Backman, RN, MHA, PhD, Ashley Lam, Rosie Papp, Aurelie Tonjock Kolle, Franciely Daina Engel, Wenshan Li, Soha Shah, Colleen Webber, Peter Tanuseputro, Marie-Cecile Domecq, and Steve Papp in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Acknowledgements
We thank Valentina Ly, MLIS (Health Sciences Library, University of Ottawa) for peer review of the MEDLINE search strategy.
Authors’ Contributions
Concept and design were done by CB, SP, PT, SS. Data acquisition and analysis were performed by MCD, AL, RB, ATK and CB. Drafting of the manuscript was done by AL, RP, ATK and CB. All authors (CB, AL, RP, ATK, FDE, CW, WL, PT, SS, MCD, SP) critically revised the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is provided within the manuscript or supplementary information files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.