
Abstract
Introduction:
The TFN-ADVANCED Proximal Femoral Nailing System (TFNA) 235 mm (DePuySynthes) and Proximal Femoral Nail Antirotation (PFNA)-II 240 mm (DePuySynthes) were developed to obtain better stability for patients with trochanteric hip fractures without increasing surgical time and amount of blood loss. However, there are currently no studies concerning clinical and radiological outcomes of patients treated using these proximal femoral nails (PFNs) that have been performed in the Japanese population. The aim of this study was to retrospectively evaluate the clinical outcomes associated with 235 to 240 mm PFNs for Japanese patients >70 years old with trochanteric hip fractures who could walk independently before the injury.
Materials and Methods:
This study involved a retrospective analysis of data on trochanteric hip fracture patients who had undergone internal fixation from March 2016 to June 2018. The inclusion criteria were patients >70 years old with trochanteric hip fractures who could walk independently before the injury and were followed up for ≥3 months after surgery. Initially, 124 patients were identified, but 33 of these were excluded because other implants were used for internal fixation. Of the remaining 91 patients in whom PFNs were used at the time of internal fixation who were included for the perioperative evaluation, 66 patients followed up for ≥3 months were included in the clinical evaluations.
Results:
The average surgical time was 56.8 ± 19.6 minutes (range, 23-123 minutes). The average blood loss was 89 ± 41 mL (range, 0-245 mL). The union rate was 98%.
Discussion:
There were no cases of nail jamming, and all nails were successfully inserted below the end of the distal isthmus without additional reaming to dilate the canal.
Conclusions:
Proximal femoral nails were a useful implant in Japanese elderly patients with trochanteric hip fractures and gave comparable clinical outcomes despite the femoral length being short and occurrence of intensive bowing.
Introduction
The frequency of hip fractures has been steadily increasing with the aging of populations in various countries around the world. 1,2 For trochanteric hip fractures, proximal femoral nails (PFNs) have been frequently used for surgical treatment. Although several reports concerning which implant yields a better clinical outcome have been published, there is currently a paucity of good supporting evidence for this. From a Cochrane systematic review, 4 trials, including a total of 910 cases, compared several PFNs and concluded that there were no significant differences among them in terms of functional outcomes, mortality, and serious fixation complications, such as the fracture of the femur, cutouts, nonunions, and reoperation rates. The limited evidence from the randomized trials currently available is insufficient to determine important differences in outcomes between the different designs of PFNs used in treating trochanteric femoral fractures. 3
When we perform internal fixation using PFNs, secondary fractures around the distal end of the nail constitute one of the most significant fracture healing complications and have been reported to lead to prolonged hospital stays, delayed recovery, and postoperative hospital stay mortality rates as high as 16.6%. 4 Although Norris et al suggested that continuing design changes had reduced the risk of these complications occurring, 5 controversy remains concerning the implant selection (eg, a short or long one) to obtain better clinical outcomes. Dunn et al conducted a systematic review to compare the clinical outcomes between long and short nails in the treatment of trochanteric hip fractures (AO Foundation/Orthopaedic Trauma Association [AO/OTA] 31A1, A2, and A3) and found that short nails had a low reoperation rate while significantly decreasing the operating time and estimated blood loss, with the additional benefit of being cost-effective. 6 Hou et al also retrospectively compared the clinical outcomes in patients with trochanteric hip fractures without subtrochanteric extension (AO/OTA 31A1 and A2) after treatment with short or long nails and reported that long nails yielded subtle increases in procedure time and blood loss despite similar clinical outcomes. 7 Especially in elderly Japanese patients, intraoperative nail jamming due to strong curvature in the femur remains a concern when long nails are used. 8 On the other hand, disadvantage of shorter nails was reported to increase a stress in the mid femur. 9 Therefore, it is still an open question what length is suitable for elderly Japanese patients.
The TFN-ADVANCED Proximal Femoral Nailing System (TFNA) 235 mm (DePuySynthes) and Proximal Femoral Nail Antirotation (PFNA)-II 240 mm (DePuySynthes) were developed to achieve better stability for patients with trochanteric hip fractures without increasing surgical time and blood loss. The morphological features of the nail are that it has a longer 35 to 40 mm nail and distal locking screw hole at the same location so that the same surgical instrument as used for the shorter nail can be used to facilitate the surgical procedure, which aims to obtain better stress distribution around the nail. However, to date, no studies concerning the clinical and radiological outcome or superiority to shorter or longer nails have been performed. Okcu et al reported that reverse oblique fractures of the trochanteric area of the femur could be treated with either 240 mm or >340 mm intramedullary nails, 10 but, to date few, studies on this issue in Asian populations have been performed.
We currently use the TFNA 235 mm and PFNA-II 240 mm as a primary option for patients with trochanteric hip fractures. Although Sawaguchi et al reported that the design of PFNAs is appropriate for the Japanese population, the rate of use of 240 mm length nails was only 2%. 11
We have hypothesized that internal fixation using the TFNA 235 mm and PFNA-II 240 mm for Japanese patients with trochanteric hip fractures can obtain good stability with acceptable operative time and blood loss. Therefore, the aim of this study was to retrospectively evaluate the clinical outcomes associated with 235 or 240 mm PFNs for Japanese patients >70 years old with trochanteric hip fractures who could walk independently before the injury.
Materials and Methods
Patient Selection
This case series study was conducted at the Department of Orthopedic Surgery of a single institution. The institutional review board of the ethics committee at our institution approved the study and waived the requirement for written informed consent because of the retrospective nature of the study.
Data on the patients with trochanteric hip fracture >70 years old who could walk independently before the injury and have undergone internal fixation from March 2016 to June 2018 were retrospectively analyzed by using an electronic medical database. During this study period, the TFNA 235 mm and PFNA-II 240 mm were mainly used for the internal fixation of all patients with trochanteric hip fractures, except for patients shorter than 140 cm or patients without a displacement trochanteric hip fracture. The inclusion criteria were patients with a trochanteric hip fracture who underwent internal fixation using the TFNA 235 mm and PFNA-II 240 mm. The exclusion criteria were patients who were lost during follow-up, died from causes unrelated to their musculoskeletal injuries, or who underwent internal fixation using shorter or longer PFNs and TFNAs.
The patient enrollment is shown in Figure 1. Initially, 124 patients were nominated, but 33 of these were excluded because other implants were used for internal fixation. The remaining 91 patients in whom the TFNA 235 mm and PFNA-II 240 mm were used at the time of internal fixation were included for the perioperative evaluation, and 66 of 91 patients followed up for ≥3 months were included in the clinical evaluations (Figure 1).

Flow of patient enrollment.
Surgical Procedure of Internal Fixation Using the TFNA 235 mm and PFNA-II 240 mm
Three board-certified orthopedic surgeons and 3 orthopedic trainees were involved in the study, and a unit of 1 board-certified surgeon and 1 trainee was in charge of surgery. Internal fixation was performed an average of 2.0 (0-11 days) days from injury. After the induction of general or regional anesthesia, closed reduction of intertrochanteric fracture using a traction table was performed to obtain a stable reduction. 12 When the anterior cortex of proximal fragment remained posterior to the distal fragment, direct open reduction via a small elevator with a small skin incision was performed. 13 After appropriate reduction was confirmed fluoroscopically, the nail of the TFNA 235 mm and PFNA-II 240 mm was attached to the aiming device and introduced through the skin incision located proximal of the larger trochanter, in accordance with the manufacturer’s instructions. The diameter of the nail was determined to be 2 mm smaller than that measured in 3-mm-thick axial computed tomography scanning. After an appropriately long blade was introduced into the femoral neck and head to ensure that the tip–apex distance was <20 mm, 14 a single distal locking screw was inserted through the static hole.
Postoperative Therapeutic Protocol
Range of motion exercises was started as early as possible after surgery. Full weight-bearing as much as tolerated was also allowed on the first day after surgery.
Clinical Evaluations
Demographic data (age, sex, height, and weight), mechanism of injury, the AO/OTA classification, duration from injury to surgery, pre- and postoperative hemoglobin (mg/dL), amount of blood transfusion (in IU), and surgical time were analyzed. Walking ability was stratified according to a 5-point scale: 5 points, walking without any aid; 4 points, walking with a cane; 3 points, walking in parallel bars; 2 points, walking with a walker; and 1 point, wheelchair-bound. 15
Results
In total, 66 (male/female, 15/51) patients were included in this study. Their mean age at the time of admission was 83.1 ± 7.0 years (range, 70-100 years). The mean height and weight of the patients were 150.8 ± 8.2 cm (range, 140-177 cm) and 47.6 ± 9.5 kg (range, 38-76 kg), respectively. The follow-up period was 10.9 ± 6.5 months (range, 3-36 months). The grades of trochanteric hip fracture were AO/OTA type A1 fracture in 17 (26%) cases, type A2 fractures in 46 (70%) cases, and type A3 fracture in 3 (5%) cases. The mechanisms of injury were same level fall for 59 (89%) cases, traffic accidents for 4 (6%) cases, falling from a height for 2 (3%) cases, and unknown for 1 (2%) case (Table 1).
Patient Demographics.
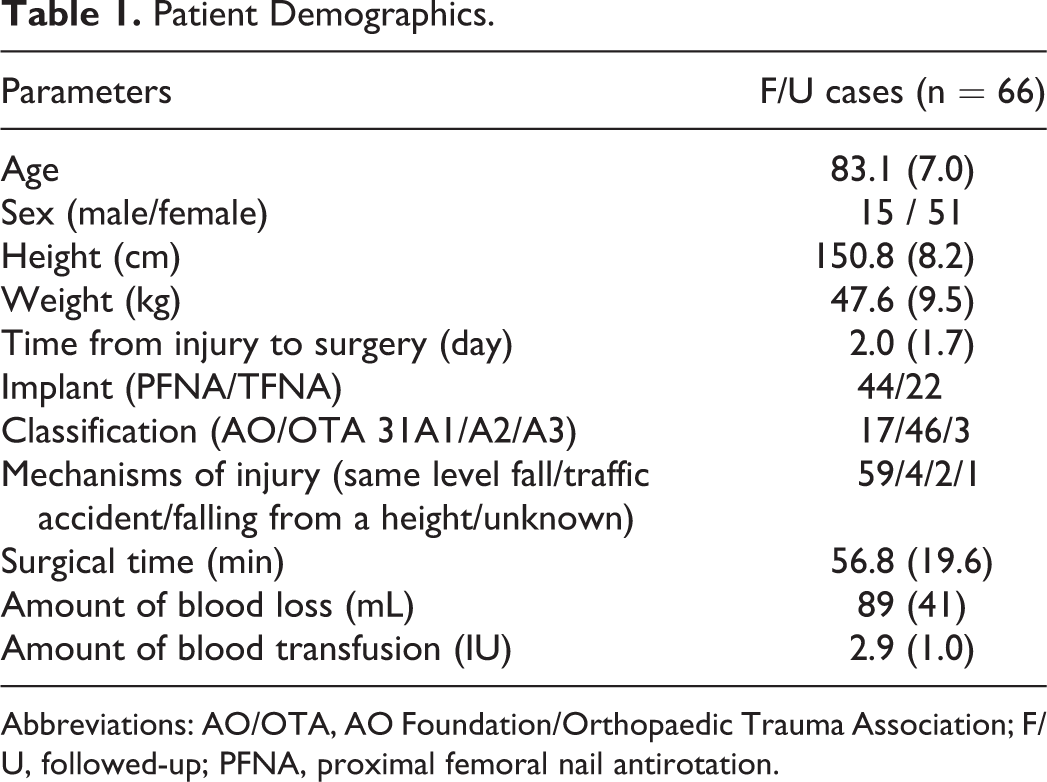
Abbreviations: AO/OTA, AO Foundation/Orthopaedic Trauma Association; F/U, followed-up; PFNA, proximal femoral nail antirotation.
Surgical Time and Amount of Blood Loss
The average surgical time was 56.8 ± 19.6 minutes (range, 23-123 minutes). The average blood loss was calculated using the numerical formula of Foss et al 16 to be 89 ± 41 mL (range, 0-245 mL). The rate and average amount of blood transfusion were 11 cases (16.7%) and 2.9 ± 1.0 IU (range, 2-4 IU), respectively (Table 1).
Radiological Evaluation of Nail Jamming During the Surgery
A PFNA-II 240 mm was used in 44 patients and TFNA 235 mm was used in the other 22 (Table 1). There were no cases in which nail jamming occurred, and all nails were successfully inserted below the end of the distal isthmus without additional reaming to dilate the canal.
Clinical Outcomes
The union rate was 98% and there was 1 case of nonunion (2%). There were no significant differences between the pre- and postoperative activities of daily living (ADL) in 26 (39%) patients, but ADL declined in 40 patients. Overall, 23 of 66 (35%) patients could not walk unaided at the time of the last follow-up visit.
Discussion
Several important findings were made in this study. First, in our Japanese patient cohort, all nails of the TFNA 235 mm and PFNA-II 240 mm were successfully inserted below the end of the distal isthmus not only without jamming but also without additional reaming to dilate the canal. Second, internal fixation using these 2 implants for Japanese patients with trochanteric hip fractures resulted in a favorable outcome with acceptable surgical time and amount of blood loss. Third, the union rate was good, the complication rate was acceptable, and no adverse effects due to the longer nail 6 were observed.
Proximal femoral nails were frequently used for internal fixation of patients with trochanteric hip fractures because they were considered to give better stability, especially for unstable cases. Crawford et al reported that 89% of patients with trochanteric hip fractures treated using PFNs healed without any complications and PFNs could be an alternative to sliding hip screws. 17 Sawaguchi et al also reported that PFNA had a large safety margin for use in Asian patients, 11 even though the femoral bones in Asian populations have several particular anatomical features such as a shorter femoral neck, a smaller neck-shaft angle, and greater anterior bowing of the femoral shaft. 18 -20
The average femur length in the Chinese population has been reported to be 428 mm, and the anterior curvature is located in the middle of the femur. 21 Additionally, the length from the most proximal point of the femoral head to the distal end of the isthmus in the Chinese population was calculated to be 221.41 mm in another study by the same group. 22 On the other hand, the average femur length in the Japanese population has been reported to be 395.7 mm. 23 Theoretically, it is thus easier for the 235 to 240 mm nails to exceed the femoral isthmus of the Japanese population. This might decrease the wiper motion, which we defined as repetitive motion of the distal nail inside the femoral canal. This phenomenon was occasionally observed when shorter nails were used, especially in cases with a stovepipe-type femur (Figure 2). Even though the longer 35 to 40 mm nail of the TFNA 235 mm and PFNA-II 240 mm is intended to obtain better stability, biomechanical experiments have shown that the nail length and position of the interlocking screw altered neither the biomechanical properties of the fixation construct nor those of the distal fracture site. 24 Additionally, there is a certain risk of nail jamming into the anterior cortex of the femur and thus preventing adequate dynamic compression of the fracture site, which could cause failure when a long nail is used. 25 However, the 235 to 240 mm length nails could be safely inserted into the femoral canal without jamming in this study, even though femoral bowing in the Japanese population is greater than that in Chinese. 26 We speculate that this is a strength of TFNA 235 mm and PFNA-II 240 mm to decrease the wiper motion of the distal nail inside the femoral canal compared with short nails without nail jamming (Figures 3 and 4). Plausible reasons for the complete avoidance of nail jamming at the time of surgery in our patient cohort are the nail design and careful creation of the proximal entry hole slightly anterior of the tip of the greater trochanter and the diameter of the nail being determined to be 2 mm smaller than the diameter of the isthmus measured by preoperative computed tomography. These factors might explain why our patients did not experience any adverse events related to the use of a longer 35 to 40 mm nail.
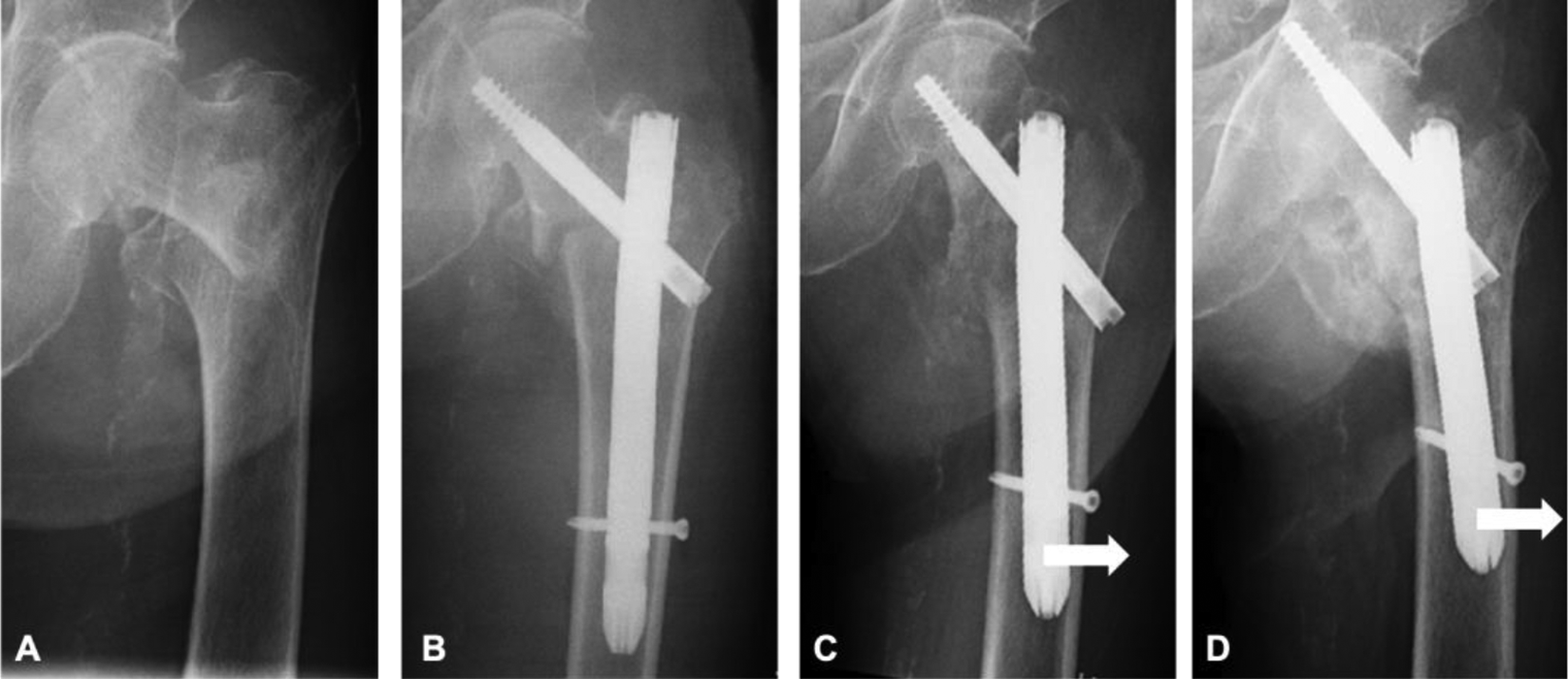
AO/OTA 31A2.2 fracture in an 82-year-old woman (height: 152 cm). A, Preoperative radiograph. The shape of the femoral canal was stovepipe-type. B, Postoperative radiograph using a Cephalomedullary Asia nail (Zimmer Biomet) 180 mm with a diameter of 13 mm. C, Postoperative radiograph at 1-month follow-up. The distal nail shifted laterally (white arrow). D, Postoperative radiograph at 4.5-month follow-up. The lateral shift of the distal nail increased (white arrow) and eventually cut through occurred. AO/OTA indicates AO Foundation/Orthopaedic Trauma Association.

AO/OTA 31A3.3 fracture in an 83-year-old woman (height: 147 cm). A and B, Preoperative radiographs. The shape of the femoral canal was stovepipe-type. B, Postoperative radiograph using a TFNA 235 mm with a diameter of 12 mm. C, Postoperative radiograph at 6-month follow-up. No lateral shift of the distal nail was observed. AO/OTA indicates AO Foundation/Orthopaedic Trauma Association.
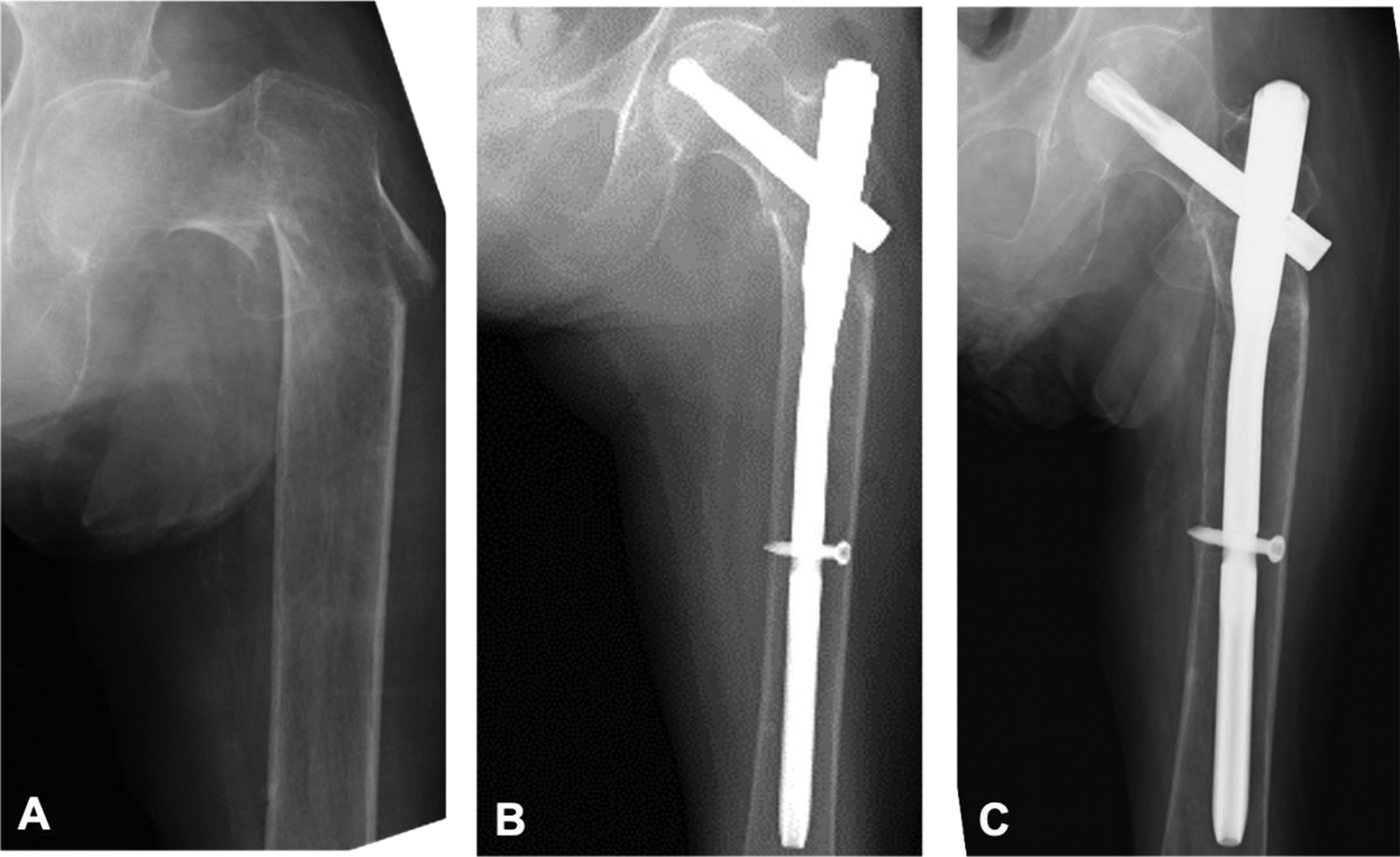
AO/OTA 31A3.1 fracture in an 87-year-old woman (height: 150 cm). A, Preoperative radiograph. The shape of the femoral canal was stovepipe-type. B, Postoperative radiograph using a PFNA-240 mm with a diameter of 9 mm. C, Postoperative radiograph at 6-month follow-up. No reduction loss was observed.
In addition, the TFNA 235 mm and PFNA-II 240 mm could be inserted by using conventional surgical instruments without any need to insert distal screws by using a radiolucent drill. The use of these fasteners facilitated insertion of the distal locking screw through the drill hole located at the same distance from the lag screw hole as that from the short nail and might have helped prevent an increase in the surgical time and thus achieve a smaller amount of blood loss. Our results showed that surgical time and blood loss were favorable compared with those associated with both long and short nails, as determined in a systematic review by Dunn et al. 6
This study had several limitations. First, it was retrospective in nature, so there was a risk of selection bias. Second, the TFNA 235 mm and PFNA-II 240 mm were used at the time of surgery and implant selection was performed in accordance with the surgeon’s preference. Although these 2 implants are fundamentally similar, the TFNA 235 mm nail has a 1000-mm radius that starts 150 mm from the proximal end and extends to 35 mm above the distal tip. On the other hand, PFNA 240 mm is a straight nail and has no radius of curvature. Therefore, in further studies of these nails, it would be preferable to analyze them separately. Third, not all cases were followed up for a minimum of 3 months, and the follow-up period was relatively short.
Despite these limitations, this was the first study to report the clinical outcomes of Japanese patients with trochanteric hip fractures treated using a TFNA 235 mm and PFNA-II 240 mm. These 2 implants are easily inserted by using a conventional surgical apparatus as well as a short femoral nail and might be of benefit by obtaining better stability comparable to that of a long nail without increasing blood loss and surgical time. In future work, we plan to clarify the risk of secondary peri-prosthetic stem fractures after a longer follow-up. A randomized study comparing the TFNA 235 mm or PFNA-II 240 mm with shorter and longer nails is needed to further assess the possible advantages and disadvantages of the various implants.
Conclusions
Internal fixation using the TFNA 235 mm and PFNA-II 240 mm for Japanese patients with trochanteric hip fractures, even for those with unstable conditions, could obtain good stability with acceptable operative time and blood loss.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.