
Abstract
Introduction
A minority of geriatric hip fracture patients pursue non-operative treatment. Compared with surgical patients, non-operative patients have higher mortality rates. However, patient satisfaction following non-operative vs operative treatment has not been investigated extensively. The purpose of this study was to compare satisfaction among non-operatively vs operatively treated hip fracture patients.
Methods
We identified patients aged 60+ years with proximal femur fractures treated over a 10-year period. Excluded were patients with isolated greater/lesser trochanteric fractures. Patients or relatives were asked to complete a 6-question survey about their treatment satisfaction.
Results
Survey responses from 56 operative and 28 non-operative patients were recorded. Overall, 91.1% of operative and 82.1% of non-operative patients were satisfied with their treatment course (P = 0.260). However, only 71.4% of non-operative patients were satisfied with treatment option explanations vs 83.9% of operative patients (P = 0.014). While only 64.3% of non-operative respondents were satisfied with the ultimate treatment outcome (vs 85.7% of operative patients, P = 0.025), 89.3% of patients in each cohort would choose the same treatment plan again.
Discussion
Our findings highlight the complexity of defining patient satisfaction, particularly in a geriatric hip fracture population. Unlike previous studies, we chose a direct approach to quantifying patient satisfaction by asking participants specifically about satisfaction with treatment outcome and the overall treatment course. Additional survey questions were then included to assess factors considered important in treatment satisfaction, such as health care provider treatment explanations, post-treatment mobility, and palliative care service involvement.
Conclusions
We identified significant differences between non-operatively and operatively treated geriatric hip fracture patients regarding satisfaction with the explanation of treatment options, and ultimate treatment outcomes. There was no significant difference in overall satisfaction with the treatment course or likelihood of choosing the same treatment again. Further research investigating patient satisfaction following geriatric hip fracture treatment is warranted.
Keywords
Introduction
Geriatric hip fractures, namely femoral neck and intertrochanteric/peritrochanteric femur fractures, are sentinel events for our aging population. Hip fractures are common in geriatric patients, with over 1.6 million hip fractures occurring worldwide annually. 1 In most cases, these hip fractures result in loss of mobility and are associated with a 1-year mortality rate that ranges from 14 to 58%. 2 The annual economic burden of treating hip fractures in the United States was estimated to be 10.3-15.2 billion dollars in 2015. 3 The incidence and costs of hip fracture management are expected to rise as the geriatric patient population is projected to nearly double by 2060. 4
Operative management is considered the standard of care for geriatric hip fracture patients, and the majority of patients or their family members elect for surgical intervention. The benefits of operative hip fracture treatment are well documented. Surgical treatment goals include pain relief, early mobilization, and prevention of complications associated with bedrest including deep venous thrombosis, pulmonary embolism, decubitus ulcers, pneumonia, and cardiopulmonary deconditioning. Nevertheless, nearly 2.6%–10.6% of geriatric hip fracture patients are treated non-operatively, often due to significant medical comorbidities or limited baseline functional status. 5 Currently, there is inconsistent reporting of the expected outcomes and mortality rates following non-operative treatment of hip fractures, with historical studies reporting 1-year mortality rates between 18%–64%.6-13 While numerous studies have evaluated morbidity and mortality following non-operative management, there are limited studies that evaluate patient satisfaction after non-operative treatment of geriatric hip fractures.
Patient satisfaction is publicly reported and often used as a subjective measure of quality of care. As quality metrics such as Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) scores are more commonly used to determine physician and hospital system reimbursement, patients’ satisfaction with their treatment plan becomes more important in their overall perceived quality of care. HCAHPS scores have been associated with objective quality and clinical outcomes in geriatric hip fracture care. 14 However, it is not clear which factors correlate with satisfaction in relation to treatment course and outcome. The purpose of this study was to compare patient satisfaction rates between a cohort of non-operatively treated geriatric hip fracture patients and a matched cohort of patients treated operatively. We hypothesized that the non-operatively treated hip fracture patients will have lower overall satisfaction with their treatment course when compared to an operative cohort.
Methods
Patient Selection
Institutional Review Board approval was waived for this study as it was deemed a quality improvement (QI) project. We conducted a retrospective review of patients 60 years of age and older who had sustained proximal femur fractures (femoral neck and intertrochanteric/peritrochanteric fractures) and were treated either operatively or non-operatively at a single, academic, level 1 trauma, tertiary-care center over a 10-year period (January 1, 2009, to December 31, 2018). Patients were identified by International Classification of Disease, ninth revision, clinical modification (ICD-9) codes (See Appendix). Excluded from this study were patients with isolated greater or lesser trochanteric fractures. Additionally, patients who were treated operatively at an outside institution but were transferred to our hospital for ongoing care were excluded.
Hip Fracture Treatment Protocols
Our institution uses a shared decision-making protocol for geriatric hip fracture patients. This process begins with a discussion between the orthopaedic consulting team (comprised of residents, advanced practice providers, and attending surgeons) and the patient and/or power of attorney detailing the significance of a geriatric hip fracture, explaining that such an injury often represents a sentinel event, marking an individual’s physiologic decline and baseline risk of mortality. The conversation then shifts to discussion of the risks, benefits, and alternatives of surgical intervention. Potential benefits of surgical treatment, including decreased pain and immediate weight-bearing, are discussed with each patient and/or power of attorney. Risks of surgical intervention are also discussed, along with the alternative option of proceeding with non-operative treatment. Particular consideration is given to specific medical comorbidities including advanced cardiovascular or pulmonary disease, chronic renal insufficiency, and advanced dementia, as these increase patients’ risks of adverse outcomes with surgical intervention. If surgical treatment is chosen, management includes one of the following operative procedures: open treatment with a sliding hip screw, cephalomedullary nail fixation, hemiarthroplasty, or cannulated screw fixation. The specific procedure recommended is determined by the particular fracture pattern and is ultimately selected at the discretion of the attending orthopaedic surgeon. If non-operative management is selected, patients are seen by the palliative care service (if that service is not already involved) and goals of care are discussed. In general, the key components of our non-operative treatment protocol include early bed-to-chair mobilization and pain control. Physical/occupational therapists and members of the palliative care and orthopaedic surgery teams remain actively involved in non-operative hip fracture management.
Data Collection and Survey Administration
The electronic medical record (EMR) was reviewed to collect demographic information, date of injury, hospital length of stay, medical comorbidities (diabetes, dementia, chronic obstructive pulmonary disease, history of cardiac arrhythmia, cerebrovascular accident/transient ischemic attack, smoking status, end-stage renal disease or chronic kidney disease), current living situation, and date of death (if deceased at the time of record review). When the EMR was not updated with the patient’s date of death, we corroborated online obituaries or publicly available death records. ASA scores were recorded from preoperative anesthesiology notes or calculated using patients’ medical comorbidities. The Charlson Comorbidity Index (CCI) was calculated using an online calculator designed by Dr Stephen Fadem. 15
Patient contact information was obtained through the EMR. We attempted to contact all patients who underwent non-operative hip fracture treatment via telephone. If successfully contacted, patients were asked to complete a 6-question telephone survey regarding their level of satisfaction with their respective treatment plan. The 6-question survey is included in Figure 1. For patients who were deceased or cognitively incompetent at the time of attempted contact, the survey was completed by a surviving family member when available. A standardized phone script was read aloud over the telephone by a study team member, and the verbal responses of the participant or surviving family member were recorded. We attempted to contact all patients in the non-operative cohort a maximum of 3 times. Once the total number of completed surveys was determined for the non-operative cohort, we attempted contacting all patients in the operative cohort using the same protocol (maximum of 3 attempts), with the goal of collecting a sufficient number of completed surveys to achieve a 2:1 ratio of operative to non-operative patients. Satisfaction after hip fracture treatment survey.
Data Analysis
Demographic and baseline characteristic variables were summarized via mean (SD), median (IQR), or N (%) based on variable distribution. Responses to survey questions were analyzed via chi-square tests to assess for associations with operative decision. All analyses were conducted using R for statistical computing version 3.3, and all tests were conducted at a two-sided 5% significance level.
Results
We identified 171 patients with hip fractures managed non-operatively who met inclusion and exclusion criteria. In total, twenty-eight patients/family members from the non-operative cohort provided responses to the telephone survey. 239 operative patients were identified who met inclusion and exclusion criteria. All 239 patients were contacted at least once. Non-responders were contacted once or twice more until a total of 56 responses from patients/family members had been recorded from the operative cohort, yielding a 2:1 ratio of operative to non-operative patients.
Summary of Demographics by Group.
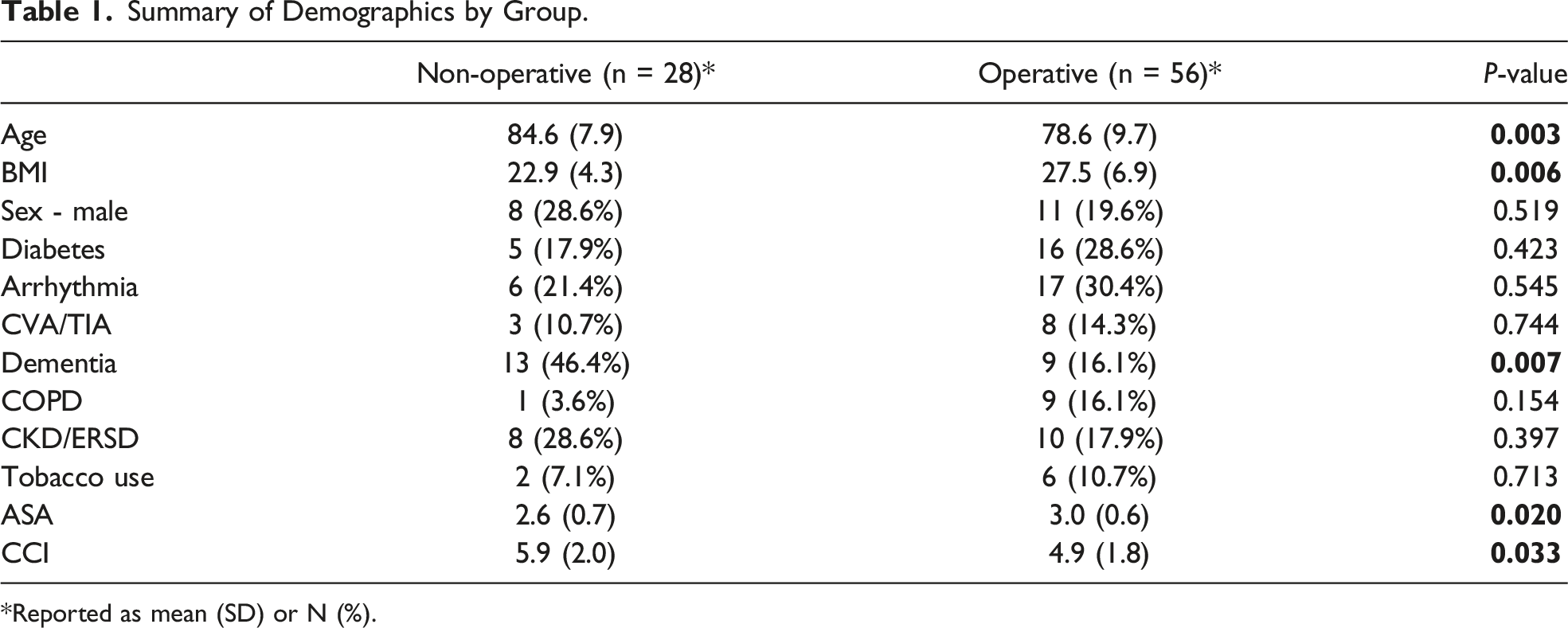
*Reported as mean (SD) or N (%).
Summary of Fracture Type and Intervention.

Summary of Survey Results Based on Management.

Survey responses indicating whether or not the patient was alive at the time of survey administration are shown in Table 4. Thirty patients were living and 54 were deceased in total; relatives of deceased patients provided survey responses. Only 5 non-operative patients (17.9%) and 25 operative patients (44.6%) were alive at the time of survey distribution (P = 0.030, Table 3.) There were no significant differences in survey responses based on living/deceased status.
Subjective mobility level after treatment was not significantly different between the 2 cohorts (P = 0.165). That said, 50% of responding non-operative patients were reportedly bedbound after treatment compared with only 25% of operative patients. Reported mobility level was more evenly distributed among the operative patients, with 35.7% able to walk moderate or short distances (16.1% and 19.6%, respectively) and 28.6% of patients being able to walk longer distances.
Results of patient/family member opinions about the relative importance of the various medical teams in the decision-making process are also shown in Table 3. Twelve patients (6 from each cohort) did not provide a response to this question. Of the patients who underwent surgery, 82.0% of respondents (41/50) believed the surgical team was more helpful than the palliative care team in choosing a treatment plan, while 18.0% (9/50) reported that the surgical and palliative care teams were both equally helpful. On the other hand, 77.3% of non-operative patients found the palliative care team to be more helpful than (27.3%, 6/22) or equally as helpful (50%, 11/22) as the surgical team in selecting the chosen treatment plan. Only 22.7% of non-operative respondents found the surgical team to be more helpful than the palliative care team in the decision making process (between group differences: P < 0.001).
Discussion
Geriatric hip fractures represent a frequent cause of morbidity and mortality in our health care system, and the incidence of these injuries is projected to increase as the population ages. Surgical treatment of hip fractures results in a heavy socioeconomic burden to the health care community. While operative and non-operative treatment outcomes following geriatric hip fractures have been well documented in the literature, 3 patient-reported outcomes with regard to treatment satisfaction are limited.16,17 The aim of our study was to provide patient-reported outcomes on the perceived satisfaction of geriatric patients following non-operative versus operative hip fracture treatment.
Summary of Survey Results Based on Living Versus Deceased Status.

In a related study, Boylan et al. determined that patient satisfaction as measured by HCAHPS scores in the geriatric hip fracture population was associated with lower 1-year mortality. However, the authors determined patient satisfaction based on 2 questions from the HCAHPS Survey, both of which assessed patients’ impressions of the quality of the hospital rather than their own treatment outcomes. 14 One key strength of the current study is the survey design. Unlike the study by Boylan et al., we chose a more direct approach to quantifying patient satisfaction by asking patients/family members specifically about satisfaction with treatment outcome and the overall treatment course. Additional survey questions were then included to assess factors considered important in treatment satisfaction, such as health care provider treatment explanations, post-treatment mobility, and palliative care service involvement.
The perceived importance of the palliative care team in selecting the chosen treatment plan was significantly different between the non-operative and operative cohorts in our study. Patients treated operatively felt that the surgical team was more helpful in determining the chosen treatment plan, whereas the majority of non-operative patients/family members believed the palliative care team was more or equally as helpful as the surgical team in the decision making process. These responses may represent a bias among patients/relatives towards the health care team that was most involved in overseeing their selected treatment regimen. In addition, not all patients who elected to proceed with operative treatment were seen by the palliative care team. At our institution, a palliative care consultation is not automatically ordered for every geriatric hip fracture patient. Nonetheless, our results indicate that the palliative care team still had a positive impact on many patients who selected operative treatment, suggesting the need for a more standardized approach to palliative care involvement in geriatric hip fracture management.
One limitation of our study is the potential for bias. Since patients and/or their family members were involved in the selection of the treatment plan, at the time of survey completion, the respondents may have been more inclined to respond favorably regarding the treatment method selected. Another potential source of bias was the completion of surveys by relatives of deceased or cognitively impaired patients. Although the family members were instructed to complete the survey based on their perception of the patient’s satisfaction following treatment, it is possible that patients and family members had differing expectations or levels of satisfaction with the overall treatment course. As such, the survey responses in these situations may more closely represent the perspectives of the relatives and not entirely those of the patients. Another limitation of our study is the fact that the non-operative cohort, which had significantly higher CCI scores than the operative cohort, may have had significantly different expectations on life expectancy and goals of care (Table 1).
One final potential limitation worth noting was the retrospective nature of the study. Since patient contact was attempted in some cases years after surgery, there is a potential for recall bias. In addition, the incidence of dementia was higher in the non-operative cohort compared with the operative cohort (46.4% vs 16.1%), and the retrospective nature of our study makes it is impossible to know whether the baseline cognitive function (ie, prior to the onset of dementia) was similar between groups. Other baseline characteristics such as socioeconomic status, occupation, and pre-injury mobility limitations were not investigated. Furthermore, despite 3 attempts at contacting each patient, we were still only able to amass a relatively small sample size compared to the number of patients initially identified by our inclusion criteria. Prospective studies would likely result in increased sample sizes and may more accurately capture patient satisfaction at various post-injury time points. In addition, there are limited standardized measures for assessing patient satisfaction following geriatric hip fracture treatment. Factors influencing treatment satisfaction for one patient may not be as important to another patient. Further research into which parameters and domains are important to geriatric hip fracture patients will aid in developing better patient-reported outcome measures.
Conclusion
Our study comparing non-operatively and operatively-treated geriatric hip fracture patients identified significantly different patient satisfaction rates with respect to ultimate treatment outcome and the explanation of treatment options, risks, and benefits. However, there was no significant difference in satisfaction with the overall treatment course or the likelihood of choosing the same treatment option again. The perceived benefit of palliative care consultation was significantly greater among the non-operative group. Further research investigating patient satisfaction following non-operative versus operative geriatric hip fracture treatment is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research support was provided by an award from the University of Wisconsin School of Medicine and Public Health, the Herman and Gwendolyn Shapiro Foundation, and the Department of Orthopedics and Rehabilitation.
Appendix
ICD-9 codes utilized: 733.82, 820.09, 820.13, 820.20, 820.21, 820.22, 820.3, 820.8, 905.3.