
Abstract
Introduction
Postoperative rehabilitation for distal femur fracture generally requires gait exercises with weight-bearing restrictions. We aimed to determine whether full weight-bearing gait exercises immediately postoperatively effectively maintain walking ability in older adult patients with distal femur fractures.
Methods
Patients diagnosed with distal femur fractures between April 2017 and March 2024 were retrospectively evaluated. Patients aged ≥75 years who had undergone surgical treatment were classified into full weight-bearing (FWB) and non-weight-bearing (NWB) groups, with FWB and NWB gait exercises starting immediately postoperatively. Patient background was evaluated in terms of age at time of surgery, sex, weight, cognitive function, and fracture type (AO classification). Postoperative outcomes were operative time, intraoperative blood loss, gait function, and postoperative complications. Two osteosynthesis conditions that allowed postoperative FWB were achievement of bony support through anatomical reduction of the medial femur and the use of adequate supplemental fixation to maintain reduction.
Results
The study comprised 21 patients (1 man, 20 women; mean age, 87.2 [79-99] years). Extra- and intra-articular fractures were identified in 16 and 5 patients, respectively. The surgical procedures were lateral plating, double plating, and one-stage total knee arthroplasty in 16, 3, and 2 patients, respectively. There were 9 and 12 patients in the FWB and NWB groups, respectively, with no significant differences in patient background. The mean decrease in the Parker mobility score was 0.11 points (range, -3-2 points) in the FWB group vs 1.92 points (range, 0-3 points) in the NWB group, indicating that gait function was maintained in the FWB group (P = 0.0063). Two and 9 patients in the FWB and NWB groups, respectively, experienced complications (P = 0.017).
Conclusion
Consideration should be given to treatment involving orthogeriatric care for older adults with distal femur fractures. Rehabilitation with FWB can preserve gait function and reduce postoperative complications.
Keywords
Introduction
In a super-aging society, the reduction in healthy life expectancy resulting from lower limb fractures is an urgent issue for consideration. 1 Early mobilization training is important for patients with geriatric trauma; however, in patients aged >75 years with proximal femur fractures, adherence to early full weight-bearing (FWB) remains challenging. Nonetheless, directives to limit weight-bearing should be abandoned.2,3 Standard treatment for proximal femur fractures with the goal of achieving early FWB has been shown to be effective in restoring walking ability and in reducing complications and mortality rates.1-3 However, for distal femur fractures, obtaining rigid internal fixation may be challenging, and the period of limiting weight-bearing is generally calculated according to fracture type and bony union status.4-8 Smith et al stated that owing to similarities between those with proximal and distal femur fractures, rehabilitation with early postoperative FWB should be indicated for patients with either fracture type, and further research is needed concerning optimal operative treatment and rehabilitation strategies. 4 Ehlinger et al reported that there is no consensus on implant selection concerning surgery for distal femoral fractures, and that the surgical technique is a major factor in achieving better radiological and clinical outcomes. 9 Recent studies have reported no increase in fracture-related complications with early FWB gait exercise following distal femur fracture fixation using a lateral femoral locking plate.5-7 Furthermore, the use of adequate supplemental fixation using either the lag screw technique or the cerclage wiring technique is effective to maintain reduction. In cases of severe comminuted fracture, the use of double plates is also effective. Among single plates, double plates, retrograde intramedullary nails, and retrograde intramedullary nails plus external plates, double plates have the strongest torsional and axial stiffnesses. 10 We considered that anatomical reduction using locking plates and supplemental fixation were important to allow early FWB exercise postoperatively.
However, no studies have investigated the effectiveness of early FWB exercises on functional outcomes in patients treated surgically in relation to distal femur fractures. Therefore, we hypothesized that early FWB exercises postoperatively in older adult patients with distal femur fractures who receive geriatric orthopedic care would be effective in maintaining walking ability. This study aimed to verify this hypothesis in patients aged >75 years with distal femur fractures.
This study was conducted in accordance with Declaration of Helsinki guidelines and comparable ethical standards. This study was reviewed and approved by the Ethics Committee of our institution. The requirement for written informed consent was waived owing to the study’s retrospective design.
Materials and Methods
In this single-center, retrospective cohort study, consecutive patients aged ≥75 years who had undergone primary surgery for distal femur fractures at our hospital between April 2017 and March 2024 were evaluated. Exclusion criteria comprised patients: (i) who had started partial weight-bearing exercises, (ii) with multiple fractures involving multiple limbs, and (iii) with serious comorbidities affecting gait-related exercises. Patients were divided into two groups: an FWB group, who started FWB gait-related exercises immediately postoperatively; and a non-weight bearing (NWB) group, who started NWB gait-related exercises postoperatively.
Background Data
Patient characteristics including age at surgery, sex, body weight, cognitive function, and fracture type (AO classification) were evaluated. Cognitive function was assessed using the Hasegawa’s dementia scale-revised (HDS-R). 11
Surgical Outcomes
Postoperative outcomes were evaluated in terms of operative time, intraoperative blood loss, gait function, and postoperative complications. Gait function was assessed using the Parker mobility score (PMS). 12 Gait function and postoperative complications were evaluated at 12 months postoperatively; however, patients whose follow-up was <12 months postoperatively were evaluated at their last follow-up.
Surgical Technique and Postoperative Rehabilitation
Four Japanese Orthopaedic Association board-certified specialist surgeons with >10 years of experience performed the surgeries. For osteosynthesis in all patients, a lateral femoral locking plate (LCP distal femoral plate; Synthes) was used (as a neutralization plate in the FWB group and as a bridging plate in the NWB group). The two necessary conditions for osteosynthesis that allowed early FWB exercise postoperatively were achievement of bony support through anatomical reduction of the medial aspect of the femur and the use of adequate supplemental fixation to maintain reduction. For supplemental fixation, either the lag screw technique or the cerclage wiring technique was selected depending on the patient. For patients with thin cortical bone owing to osteoporotic changes and concerns regarding stabilization with screws, the cerclage wiring technique was selected. In cases of comminuted fractures in which the medial bony support was disrupted and where the above conditions were not met, a medial plate was added. In cases of intra-articular fractures with osteoarthritis, cemented stem total knee arthroplasty (TKA) in combination with osteosynthesis was performed in a single stage for early FWB exercise postoperatively.
Rehabilitation was performed under the supervision of a licensed physiotherapist. One surgeon provided postoperative care with early FWB exercises, whereas the other three surgeons initiated postoperative care with NWB. The rehabilitation program varied in individual patients according to each patient’s condition. The progress of weight-bearing in the NWB group was determined individually at the discretion of each attending physician in charge.
Statistical Analysis
Pearson’s chi-square and Mann–Whitney U tests were used for comparisons between the two groups, with a significance level of 0.05. All statistical analyses were performed using JMP ver.14 (Abacus Concepts, Berkeley, CA, United States) software.
Results
Patient Background Data in the FWB Group.

Abbreviations: DVT, deep vein thrombosis; FWB, full-weight bearing; HDS-R, Hasegawa’s dementia scale; PMS, Parker mobility score; THA, total hip arthroplasty.
TKA, total knee arthroplasty.
Patient Background Data in the NWB Group.
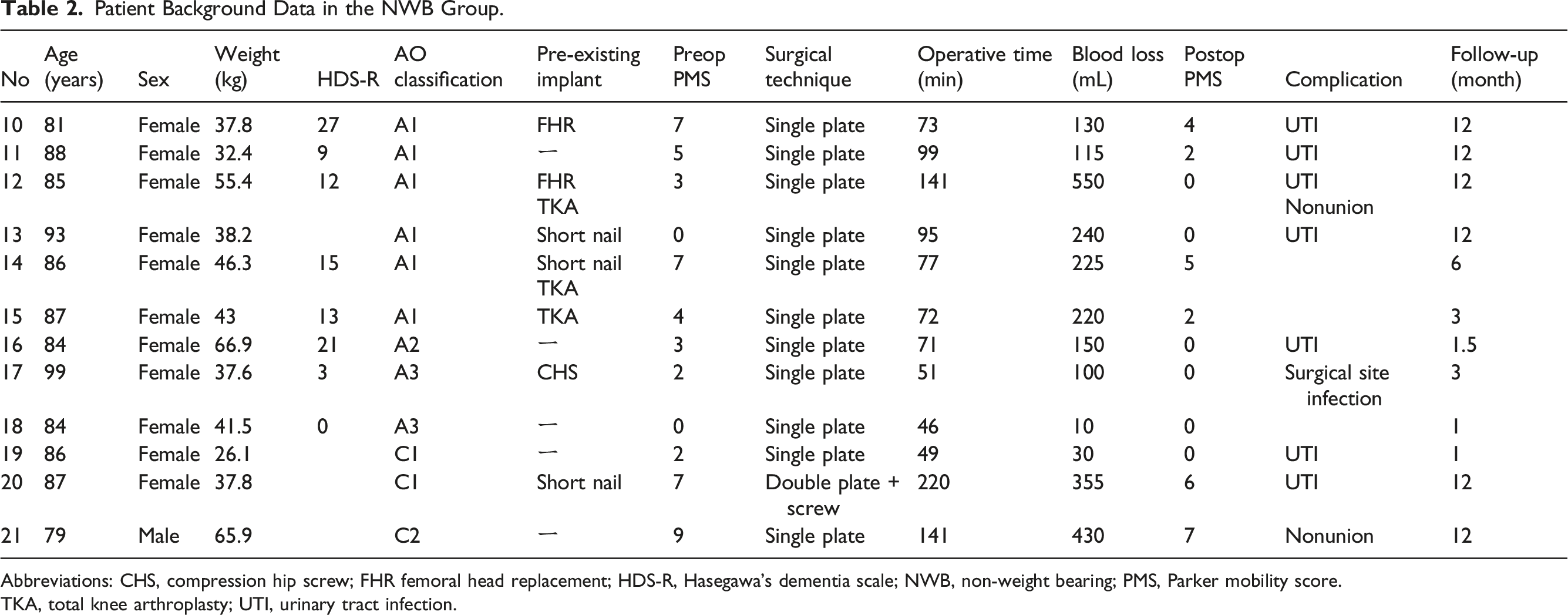
Abbreviations: CHS, compression hip screw; FHR femoral head replacement; HDS-R, Hasegawa’s dementia scale; NWB, non-weight bearing; PMS, Parker mobility score.
TKA, total knee arthroplasty; UTI, urinary tract infection.
A Comparison of Patient Background Data Between the Two Groups.
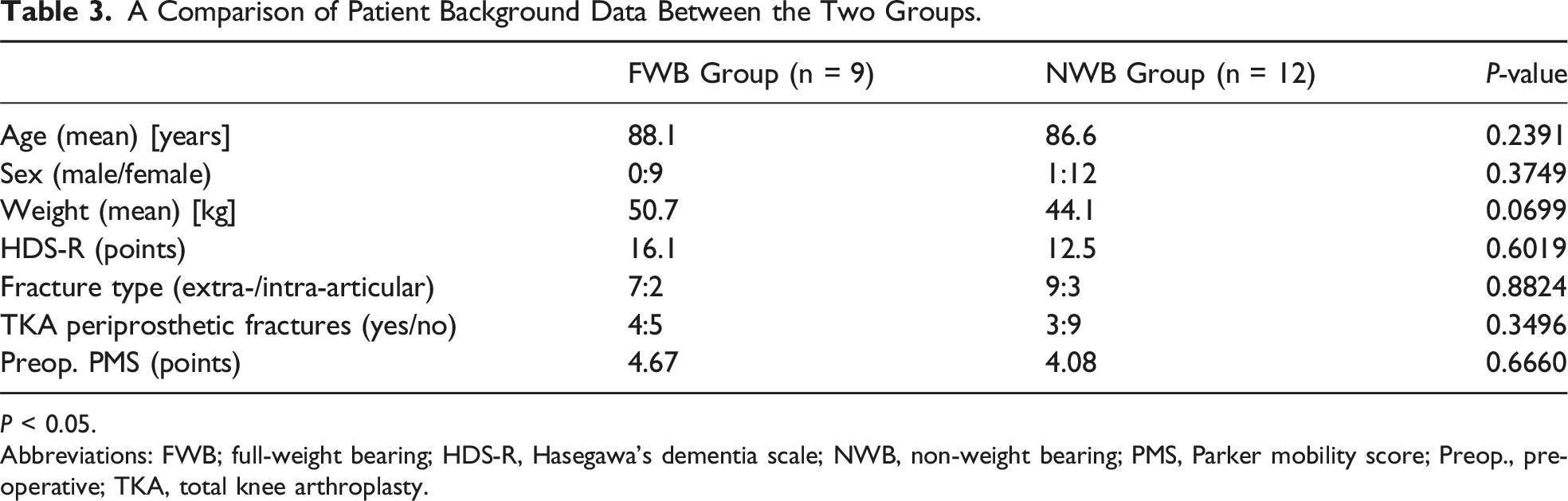
P < 0.05.
Abbreviations: FWB; full-weight bearing; HDS-R, Hasegawa’s dementia scale; NWB, non-weight bearing; PMS, Parker mobility score; Preop., preoperative; TKA, total knee arthroplasty.
A Comparison of Surgical Outcomes Between the Two Groups.

**P < 0.05.
Abbreviations: FWB; full-weight bearing; NWB, non-weight bearing; PMS, Parker mobility score; UTI, urinary tract infection; DVT, deep venous thrombosis; 95% CI, 95% confidence intervals.
aEffect size, 1.81 (95% CI 0.65-2.96); standardized effect size (effect size divided by standard deviation), 1.19 (95% CI 0.43-1.94).
Clinical Case Report
Case 2
A 91-year-old woman weighing 43.4 kg sustained a fall. Her HDS-R score was 11 points, indicating severe dementia. Prior to her injury, she had been capable of walking with the help of a wheeled walker (PMS: 4 points). Plain radiographs indicated an extra-articular simple fracture of the distal femur (AO classification type A1, Figure 1(a)). The fracture was treated surgically with open reduction and internal fixation, medial femoral anatomic reduction was obtained, and two wirings with ultra-high molecular weight polyethylene cables were added to the lateral locking plate to maintain the reduction (Figure 1(b) and (c)). Rehabilitation was initiated with FWB immediately postoperatively, and she was able to stand using parallel bars on postoperative day one. At 3 weeks postoperatively, she had regained her preoperative ability to walk with a walker. At 6 months postoperatively, she had maintained her walking ability without pain, and bony union was confirmed on plain radiographs (Figure 1(d)). A fall injury in a 91-year-old woman. (a) Plain radiographs showing a simple extra-articular fracture of the distal femur (AO classification A1). (b, c) Intraoperative and postoperative plain radiographs showing an anatomic reduction of the medial aspect of the femur and additional fixation with ultra-high molecular weight polyethylene cables. (d) Plain radiograph showing bony union at 6 months follow-up.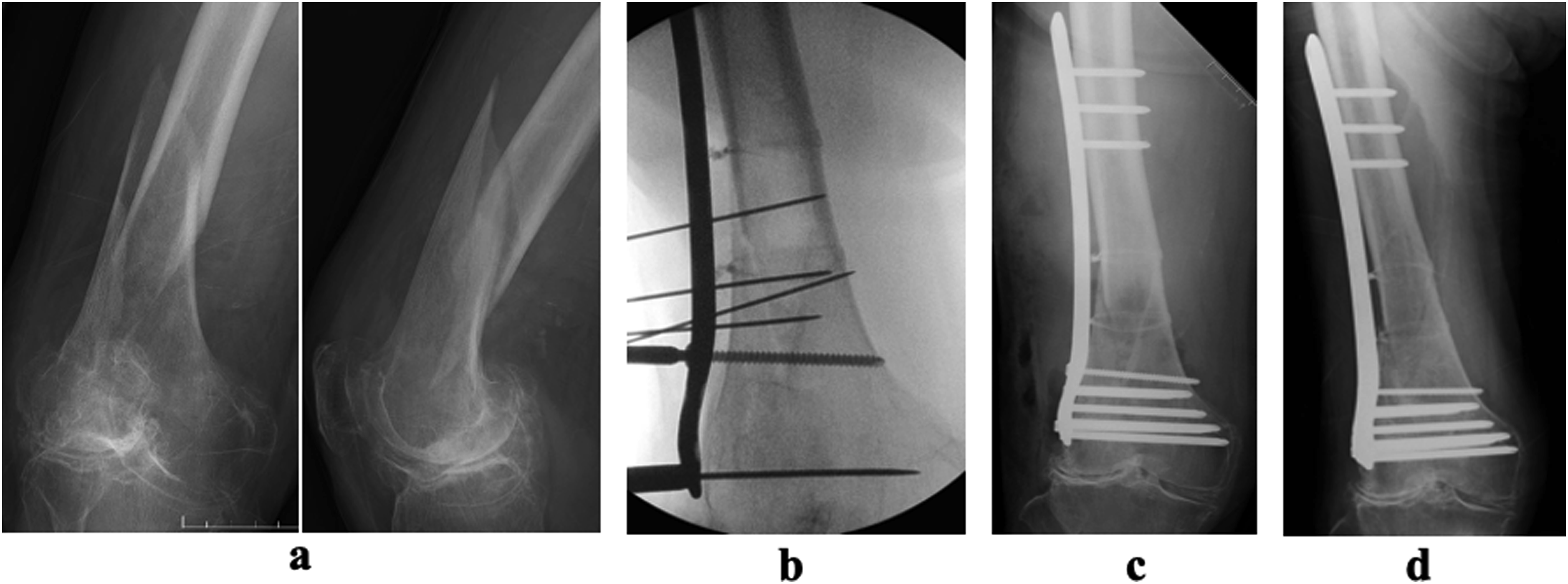
Case 9
An 88-year-old woman weighing 41 kg sustained a fall. Her HDS-R score was 28 points (indicating no dementia). She could only walk short distances with a single cane owing to severe knee osteoarthritis prior to the injury (PMS, 3 points). Plain radiographs indicated end-stage knee joint osteoarthritis and a distal femur fracture (Figure 2(a)). Computed tomography imaging revealed a comminuted fracture of the distal femur and an intraarticular fracture (AO classification type C2, Figure 2(b)). Osteosynthesis was performed using one-stage TKA (Figure 2(c)). The operation time was 287 min, and the intraoperative blood loss was 2370 mL owing to challenges in stemming the bleeding with a tourniquet, resulting in the need for invasive surgery. Rehabilitation was initiated with FWB immediately postoperatively. At postoperative week 5, she could walk short distances without any support (PMS, 6 points), and improvement in lower extremity alignment was observed when using the standing sterEOS imaging system (Figure 2(d)). A fall injury in a 89-year-old woman. (a) Plain radiographs showing a supracondylar fracture of the femur and osteoarthritis of the knee joint. (b) Computed tomography showing an intra-articular comminuted fracture of the distal femur (AO classification 33-C2). (c) Postoperative plain radiographs showing primary TKA in combination with a plate and wiring osteosynthesis. (d) Standing sterEOS imaging system showing good alignment of the lower extremity at 1 month follow-up. Abbreviation: TKA, total knee arthroplasty.
Discussion
Life expectancy is increasing worldwide, and societies are aging at an unprecedented rate. The need for geriatric orthopedic care has received increasing attention given fragile bone fractures are the most common type of orthopedic trauma in older adults. Additionally, prolonged bed rest can result in various complications, such as thromboembolism, bedsores, urinary tract and respiratory infections, frailty progression, delirium, and exacerbation of pre-existing conditions. 1 Japan has the world’s most-aged population, with those aged 65-74 years defined as early-stage older adults and those aged ≥75 as late-stage older adults. Rehabilitation with adherence to PWB is challenging for almost all patients aged ≥75 years.2,3 This study is the first to compare surgical outcomes, including gait function for distal femur fractures, between patients aged ≥75 years treated with postoperative FWB exercises and those treated with NWB exercises. Distal femoral fractures are relatively rare, accounting for 3-6% of all femoral fractures, with a reported two-peaked distribution of high-energy trauma in young men and low-energy trauma in older women.4-8 This study included older patients aged ≥75 years, with >50% of all distal femur fractures treated at our hospital fitting within this age category. Moreover, most patients were women, which is consistent with previous reports.4-7 Additionally, 13 of 21 patients in our study had existing implants, and TKA periprosthetic fractures accounted for >50% of these, reflecting the current situation in which TKA periprosthetic fractures are no longer rare among fragility fractures in the older adult population.
Our study findings indicated that the FWB group maintained their walking ability better than the NWB group. Young patients can be rehabilitated in a standing position even if they are instructed to undergo NWB exercises. However, for older adult patients who face challenges standing in a NWB position, the NWB instructions refer to rehabilitation in a seated position. Thus, the same rehabilitation instructions involve very different content for young and older adult patients. In a gait analysis using insoles postoperatively for proximal femur fractures, Pfeufer et al suggested that older adult patients should try to perform postoperative FWB exercises given those performing partial weight-bearing exercises are prone to failure, which may decrease their walking ability. 3 Therefore, even in distal femoral fractures, surgical treatment with the goal of early postoperative FWB exercises is necessary for older adult patients. No differences in operative time or intraoperative blood loss were observed between the two groups; however, the frequency of postoperative complications was significantly higher in the NWB group. The most frequent complications were urinary tract infections, which were considered mainly to result from an inability to transfer a patient to the toilet in an upright position. There were no significant differences in surgery-related complications in the FWB group, which is consistent with previous studies reporting that the early weight-bearing protocol did not increase postoperative complications.4-7
Generally, in relation to distal femoral fractures, a patient is typically placed on partial weight-bearing or NWB instructions postoperatively depending on fracture type or fixation technique, which continues from 4 to 12 weeks until bone callus is formed.4-8 This is an unacceptable rest period in geriatric orthopedic care; therefore, we performed surgical procedures for older adult patients with two requirements, aiming for early FWB exercises. The first requirement was achievement of bony support through anatomic reduction of the medial aspect of the femur. Based on the anatomical features of the femur, as tensile forces are exerted on the outside of the fracture site and compressive forces are exerted on the inside, anatomical reduction of the medial cortex is important. Compressive forces between bone fragments are also effective in maintaining reduction and can distribute the load on the implant to the bone. The second requirement was implementation of adequate supportive fixation to maintain the reduction. In most fragile fractures, the basic principles of fracture treatment can be applied; however, these principles should be adjusted to account for bone strength loss.1,13 Bone mineral density has been reported to correlate with screw-holding power, and prolonged implant-only loading on osteoporotic bone can lead to implant failure, screw loosening, microfracture, and bone resorption around the fracture site. 1 The wiring technique is useful for thin cortical bones with osteoporotic changes when compression using the lag screw technique is not possible.1,13 Furthermore, older adult patients require a longer period for bony union given their reduced osteogenic potential. Therefore, for successful FWB rehabilitation in older adult patients, it is important to provide sustained stabilization of the fracture site using supplemental fixation with screws or wiring. In this study, anatomical reduction and supplemental fixation were considered important to ensure success of the surgical technique. One case in which the first requirement could not be achieved involved a patient with a comminuted fracture with difficulty in obtaining medial bony support. One biomechanical study reported that double plates have the strongest torsional and axial stiffnesses among single plates, double plates, retrograde intramedullary nails, and retrograde intramedullary nails plus external plates for the treatment of distal femur fractures. 13 In a review of double plating for femoral fractures, Lodde et al reported bone union rates of 88% and 89% for distal femur fractures and TKA periprosthetic fractures, respectively, while showing no difference in bone union rates, complications, or functional outcomes compared with single plating. 14 We consider that, given the surgical invasiveness involved, double-plate fixation should be limited to cases in which medial bony support cannot be obtained. Primary TKA for distal femur fractures plays an important role in the treatment of older adult patients; however, comparative studies are limited, making a general recommendation difficult. 1 In a review of primary TKA for fractures around the knee joint, Parratte et al reported that the most common indication was complex intraarticular fractures in older adult patients with underlying knee osteoarthritis, consistent with the indications in this study. Primary TKA for fractures could lead to lower rates of revision surgery and complications compared with secondary TKA after failure of nonoperative treatment or osteosynthesis. Furthermore, the authors concluded that primary TKA is promising as it allows for early postoperative FWB rehabilitation and better functional outcomes. 15 In this study, primary TKA in combination with osteosynthesis tended to require a longer operating time and involve greater blood loss than osteosynthesis alone. Therefore, we recommend that this operation be performed or assisted by a surgeon who has mastered the technique of revision surgery, and that careful evaluation is necessary to determine the indications for this type of surgery.
For older adult patients who have difficulty with adherence to FWB, a surgical procedure that allows for immediate FWB is ideal to achieve early mobilization. With advances in surgical techniques and instrumentation, surgery with early FWB rehabilitation for distal femur fractures is now possible.16,17 In geriatric orthopedics, surgeons are required to select the best treatment for fractures and in relation to a patient’s general condition. It is also necessary to establish an optimal patient-oriented standard treatment system for distal femur fractures, and the findings of this study may be helpful in this regard.
This study had some limitations. It was a retrospective cohort study involving a small sample size, and was undertaken at a single institution. However, power analysis and statistical power were performed to detect an effect size of 76% (α = 0.05, two-sided) or 85% (α = 0.05, one-sided), which indicated acceptable reproducibility. The selection of surgical procedures and post-treatment varied according to each patient’s condition. The rehabilitation program and duration of NWB rehabilitation also varied. Another limitation was the predominately female sample recruited for this study. Further prospective large-scale studies including more equal numbers of both sexes are necessary to establish a treatment strategy based on geriatric care similar to that for proximal femur fractures. However, our study findings highlighted the usefulness of early postoperative FWB gait-related exercises between the two groups, with no difference observed in patient background, fracture type, and among the older adult patients.
Conclusion
Our study findings suggest that distal femoral fractures in older adults should be treated with early mobilization training. As a surgical procedure aimed at early FWB exercises, the achievement of bony support through anatomical reduction of the medial aspect of the femur and the application of supplemental fixation sufficient to maintain the reduction are prerequisites. Early rehabilitation with FWB instructions can preserve gait function and reduce postoperative complications.
Footnotes
Acknowledgements
Author contributions
All authors commented on previous versions of the manuscript, and approved the final manuscript. Conceptualization: Shin Watanabe; Data curation: Shin Watanabe, Yasuharu Shinjo, Koushiro Imai, Mikio Muraoka; Methodology: Shin Watanabe, Kei Watanabe; Formal analysis and investigation: Shin Watanabe, Yasuharu Shinjo, Koushiro Imai, Mikio Muraoka; Writing - original draft preparation: Shin Watanabe; Writing - review and editing: Kei Watanabe; Supervision: Mikio Muraoka
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB statement
This study was reviewed and approved by the Ethics Committee of Kameda-Daiichi Hospital (approval number: ket23-10).