
Abstract
Introduction
Up to one-third of patients with fragility hip fractures are totally dependent in the year following the injury which leads to later morbidity and mortality. Understanding the related factors that affect patients’ ambulation helps health care providers prepare for the treatment plans to improve their functional outcomes. This study aimed to evaluate the factors associated with independent walking disability in the early postoperative period after fragility hip fractures.
Material and methods
This retrospective cohort study involved 394 patients with fragility hip fractures with either intertrochanteric, subtrochanteric, or femoral neck fractures from January 2018 to June 2023. The related factors including preoperative demographics, perioperative, and postoperative factors, were collected and analyzed. The endpoint was the independent walking disability of patients at 6 weeks after surgery.
Results
110 patients (27.9%) were disabled, whereas 284 patients (72.1%) could walk independently at postoperative 6 weeks. The multivariable risk ratio regression analysis showed that patients with age ≥80 years (RR 1.65; 95% CI 1.21-2.25; P = 0.001), pre-fracture walking with the gait aid (RR 2.03; 95% CI 1.53-2.69; P < 0.001), having ≥2 underlying comorbidities (RR 1.63; 95% CI 1.19-2.23; P = 0.002), preoperative hypoalbuminemia (RR 1.74; 95% CI 1.32-2.29; P < 0.001), and presence of the postoperative medical complication (RR 2.04; 95% CI 1.37-3.02; P < 0.001) were significantly associated with independent walking disability at the early postoperative period of 6 weeks.
Conclusions
Post-hip fracture surgery patients with the presence of postoperative medical complication have the highest risk of independent walking disability. Health care providers should concentrate on high-risk patients, correct the modifiable factors, and minimize any postoperative complications to improve functional recovery and decrease morbidity related to non-ambulation after fragility hip fractures.
Introduction
Fragility hip fractures are 1 of the major health care issues in recent years, as the increased incidence of osteoporosis in the emerging elderly population. 1 With a global estimated 14.2 million fragility hip fractures annually, the number of patients will become greater by 1.9 times in the year 2050.2,3 These patients are vulnerable to developing any morbidities from direct surgical-related issues eg, wound infection and hardware failure, to postoperative medical complications such as pressure sores, urinary tract infection, acute kidney injury, cerebrovascular and cardiopulmonary problems. 4 Moreover, 1-year mortality in patients with fragility hip fractures remains high, ranging from 13%–30%.5-8 These fractures not only affect the patients’ physical and mental status, but also burden their relatives and caregivers especially in the first 3 months after treatment. 9
Early ambulation is the important goal following fragility hip fracture treatment to prevent the related morbidity and mortality. 7 However, a previous study demonstrated that only 40%–60% of patients were able to regain their previous level of ambulation after fracture, and nearly one-third of them remained totally dependent or in a nursing home.10,11 Approximately 50% of patients could resume walking as pre-fracture status within the initial 6 months, with minimal improvement observed in the subsequent periods.12,13 The early walking ability, either within hospitalization or postoperative 1 month is a prediction factor of both 1-year and 10-year survivorship. The patients who could walk in the early postoperative period showed a significant improvement in the survivorship after surgery. 14 Providing a fracture liaison service model with holistic approaches is encouraged to enhance the ambulatory status of the patients after fragility hip fractures. 8 Recently, there has been a gap of knowledge in the factors influencing walking disability among fragility hip fracture patients, particularly the early postoperative 6 weeks post-surgery, as this time is the beginning of functional recovery for patients in transitioning from acute care to rehabilitation and start to regain mobility and independence. 15 The aim of this study was to evaluate the factors influencing independent walking disability at 6 weeks in patients undergoing fragility hip fracture surgery. Understanding these factors may help health care providers better prepare treatment plans to improve patients’ functional outcomes and ambulatory status.
Material and Methods
This retrospective cohort study was conducted and obtained the data of fragility hip fracture patients from January 2018 to June 2023. The protocol of this study was approved by the Human Research Ethics Committee. Patients aged 60 years and older with fragility hip fractures either intertrochanteric, subtrochanteric, or femoral neck fractures, were enrolled in this study. The fragility hip fractures were diagnosed when the fractures were caused by a minor trauma or a fall from a standing height. 16 The exclusion criteria were the patients with pre-fracture status of bedridden or wheelchair ambulation, refused or had severe medical conditions that were unstable for surgical treatment, pathological fractures from malignancy, and loss to follow-up or death before postoperative 6 weeks. Surgical intervention was performed by board-certified orthopedic surgeons, and the procedures varied according to the fracture characteristics. All patients received identical postoperative physical therapy protocol including muscle strengthening and balancing exercises. They were taught to move from sitting to standing positions and from bed to chair, while walking training with a gait aid was encouraged for those who could tolerate it. Before discharge, patients and their caregivers were instructed to continue the physical therapy and home care programs. The patients were then scheduled for routine follow-up visits at 6 weeks after surgery.
General information and the data of related factors were systematically obtained from a chart review. Preoperative demographics and underlying comorbidities, pre-fracture walking status, nutritional status evaluated by serum albumin, kidney function assessed by the glomerular filtration rate (GFR), and fracture characteristics, were the collected variables. The pre-fracture walking status was classified into 2 groups: the patients who required the assistance of a gait aid and the patients who were able to walk without a gait aid. Perioperative factors including the waiting time for surgery, the American Society of Anesthesiologists (ASA) physical status classification, and the operative procedures, were retrieved. The postoperative parameters consisted of triceps and quadriceps muscle strength which was evaluated by manual muscle testing on the day before discharge from the hospital. Triceps muscle strength was assessed by the power of elbow extension, whereas quadriceps muscle strength was evaluated by the power of knee extension. The grading of both triceps and quadriceps muscle strength ranged from grade zero (no muscle tone) to grade V (resist gravity and be able to hold out against the maximum break force). 17 The other postoperative parameters included the Barthel index, a measurement tool that is used to evaluate physical performance in activities of daily living (ADL). It comprises 10 variables which are based on ADL and mobility, and each item is rated on a scale. A higher score is, a greater likelihood of the patient being independent after discharge from the hospital. 18 The intraoperative and postoperative medical complications were the adverse events that arose during and after surgical intervention during hospitalization, respectively. The specific conditions that were likely to impact the patients’ walking ability eg, unstable hemodynamic status, pressure sores, urinary tract infection, urinary retention, pneumonia, cerebrovascular and cardiopulmonary complications, were also collected. The clinical endpoint of this study was the independent walking disability at postoperative 6 weeks. Patients were classified as having “independent walking disability” when the individuals required human assistance for ambulation or became dependent on a wheelchair. In contrast, patients classified as having “independent walking ability” referred to those who could walk with or without gait aid, but without human assistance. 19
Statistical Analyses
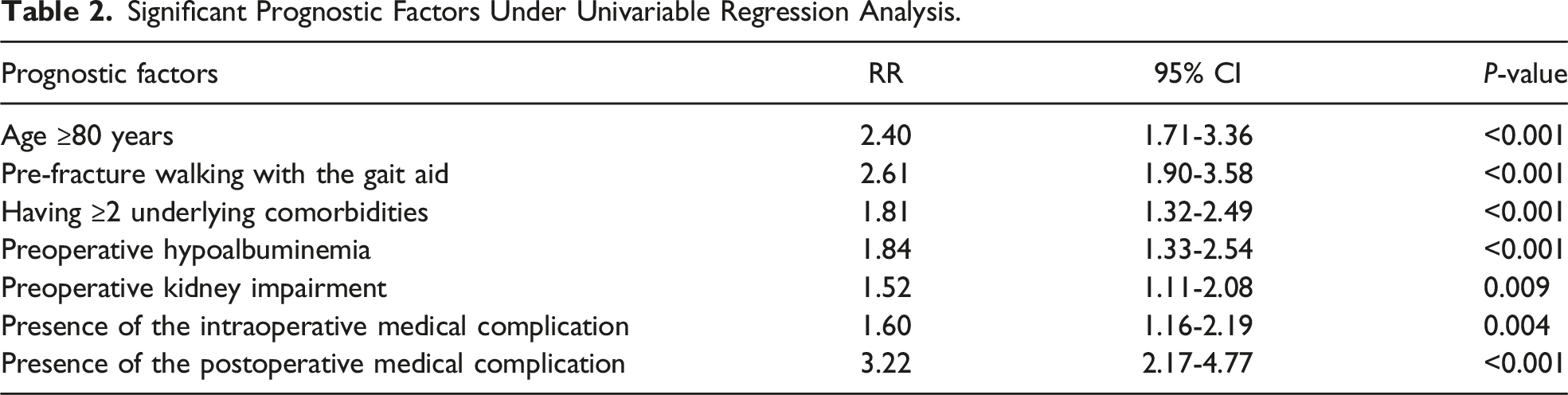
As a comparison of data between the independent walking disability and the ability group, the continuous variables were analyzed using the Student's t-test which demonstrated a comparison of means and standard deviation (SD) between the 2 groups. For categorical variables, the percentage values between groups were analyzed by the exact probability test. In exploring the factors that impact individual outcomes, the univariable risk ratio regression analysis was employed, incorporating the focused 7 variables (age, pre-fracture walking status, preoperative serum albumin level, preoperative GFR, underlying comorbidities, presence of the intraoperative and postoperative medical complications). Crude risk ratios and their respective 95% confidence interval (CI) were established at a significance level of 0.05. The focused variables were considered and indicated as follows: age, specified with a cut-off at 80 years and older; preoperative hypoalbuminemia, denoted by a serum albumin level ≤3.5 g/dL; preoperative kidney impairment, identified by a GFR ≤60 mL/min/1.73 m2; and underlying comorbidities, defined as the presence of 2 or more concurrent diseases before fracture. Following this, these variables were integrated into the equation for multivariable risk ratio regression analysis. The multivariable risk ratios and their 95% CI were then calculated to identify the significance contributing to the prediction of independent walking disability.
Determining the sample size is crucial to ensure the statistical power needed for reliable results. In this study, the power of 80% was set to achieve a significance level of 0.05. Based on the practical data and a study by Smith et al 20 which demonstrated the prevalence of disability prior to hip fractures, we estimated a ratio of 1:9 for patients who were unable to walk independently to those who were able to walk independently, and specifically focused on the age of the patients to identify through a preliminary pilot study as the factor that necessitated the largest sample size. This meticulous approach ensured that the number of study subjects was adequate to detect the effects within the specified confidence level. All statistical analyses were performed using Stata/BE 17.0 software (StataCorp LP, College Station, TX, USA), and statistical significance was defined as a P-value <0.05.
Results
A total of 486 patients with fragility hip fractures were enrolled in this study. Of those, 92 patients were excluded as follows: 62 patients were denied or unstable for surgery, 3 patients were bedridden before fracture, 17 patients died before follow-up, and 10 patients were lost to follow-up. The remaining 394 patients were included in the final analysis. Among them, 110 patients (27.9%) were unable to walk independently, while 284 patients (72.1%) could walk independently (Figure 1). The majority of patients were female in both groups (68.2% and 77.8% in the independent walking disability and the ability group, respectively). When comparing the 2 groups, the independent walking disability group had a larger percentage of patients who were diagnosed with an intertrochanteric fracture of the femur than the independent walking ability group (64.5% vs 52.5%, respectively). Additionally, the patients in the independent walking disability group also provided an older average age (82.2 ± 8.2 years vs 75.9 ± 8.8 years, P < 0.001), a larger percentage of the individuals who required the gait aid before fracture (51.5% vs 20.5%, P < 0.001), a greater prevalence of patients with underlying comorbidities (56.4% vs 35.9%, P < 0.001), a lower average preoperative serum albumin level (3.5 ± 0.5 g/dL vs 3.8 ± 0.5 g/dL, P < 0.001), a lower average preoperative GFR (60.4 ± 22.3 mL/min/1.73 m2 vs 68.1 ± 22.5 mL/min/1.73 m2, P = 0.003), a larger percentage of patients who had the intraoperative medical complication (38.9% vs 24.5%, P = 0.006), and a larger percentage of patients who had the postoperative medical complication (75.9% vs 39.2%, P < 0.001). Poor triceps muscle strength (grade 0-III) was found in almost half of the patients in the independent walking disability group. In contrast, only 10.8% of patients in the independent walking ability group had weakness of the triceps muscle (Table 1). A diagram showing the flow of patients in the study. Patients’ Characteristics. Notes: Data are presented as mean ± SD for age, body mass index, serum albumin level, GFR, and Barthel index.

Significant Prognostic Factors Under Univariable Regression Analysis.
Prognostic Factors Under Multivariable Regression Analysis.


A coefficient plot showing the prognostic factors and the multivariable risk ratios indicates that pre-fracture walking with the gait aid and presence of the postoperative medical complication have the highest risk ratios in the final model.
Discussion
Recovery of independent walking after surgical treatment of fragility hip fractures is associated with improvement of the patients’ quality of life, decreasing morbidity and mortality. 21 Walking ability and motion restoration are among the most common concerns for patients with fragility hip fractures during the postoperative period. 22 Our study found that the presence of at least 1 postoperative medical complication and the use of a gait aid prior to the fracture were the most significant factors associated with independent walking disability at 6 weeks postoperatively in fragility hip fracture patients aged ≥60 years. In addition, the other factors like the elderly with 80 years of age and above, poor nutritional status, and having 2 or more underlying diseases at the time of surgery, were the risk of the undesirable outcome of post-surgical walking ability. For the intermediate and late postoperative period, a study by Ko 23 concluded that older adults >65 years old, altogether with poor pre-fracture ambulatory status, and living in a long-term care facility, were the risk factors of walking recovery failure after 3 to 6 months of hip fracture surgery. Another study by Fu et al 24 also demonstrated that preoperative walking ability, surgical procedure, anesthesia procedure, smoking history, gender, Charlson Comorbidity Index (CCI) score, age, serum albumin, and chest radiograph, were the significant predictors of walking ability at 1 year after arthroplasty in patients with femoral neck fractures. However, in the earliest postoperative period, Buecking et al 25 conducted a prospective observational study and found that pre-fracture CCI, ASA classification, pre-fracture Barthel index, and depression risk were the independent factors influencing walking ability at 4-day post-hip fracture surgery.
This study defined the assessment at 6 weeks after fragility hip fracture surgery as the steady recovery of the ADL in hip fracture patients begins approximately 6-8 weeks after fracture. 15 Overgaard et al 26 performed a randomized controlled trial to compare the walking distance after hip fracture surgery between patients who received 6- and 12-week physical therapy programs and reported that extended physical therapy up to 12 weeks was not superior to 6 weeks in improving walking distance. These findings reassured our theory that the first 6 weeks after hip fracture surgery could be the golden period for walking recovery.
Independent walking may be delayed by several factors. Any postoperative medical complications that occur after surgical intervention could impact walking ability and the long-term outcomes of overall functional recovery. The medical complications affected approximately 20% of hip fracture patients, with cardiopulmonary complications identified as the most frequent adverse events after hip fracture surgery. 27 Cognitive and neurological alterations, gastrointestinal tract bleeding, electrolyte imbalance, urinary tract infection, and anemia were also found frequently in these patients. 4 Pressure sores are another postoperative complication caused by immobility, moisture, and prolonged pressure points. This preventable condition is associated with other medical complications, especially postoperative sepsis, pneumonia, urinary tract infection, and delirium. 28 A study by Uriz-Otano et al 29 demonstrated that patients who developed pressure ulcers after hip fracture surgery had a worse likelihood of walking recovery ability than patients who had cognitive impairment. Previous use of the gait aid before hip fracture is 1 of the most predictable indicators for postoperative independent walking because these patients are prone to have instability gaits and falls. 1 The findings from our study at the early postoperative 6 weeks also support previous literature, which indicates that similar trends are observed at various postoperative time points.
Patients with hypoalbuminemia are correlated to malnutritional status and various chronic diseases. This condition induces accelerated loss of muscle mass, which later in the late stage could become sarcopenia. 30 Sarcopenia combined with hypoalbuminemia increases the risk of incident disability not only in hip fracture patients but also in community-dwelling older adults without existing disability. 31 Similarly to our study, literature published by Aldebeyan et al 32 showed that hypoalbuminemia alone was a predictor of postoperative morbidity and increased length of hospital stay, which directly affected walking recovery. Older patients with underlying several medical comorbidities are straightforwardly associated with recovering ability after hip fracture surgery. A study by González-Zabaleta et al 33 also found that comorbidity was the only variable predicting the incapacity to walk at 90 days after hip fracture surgery in patients with an average age of 84 years. In the previous study, the most common comorbidities in patients who suffered from hip fractures were cardiac, respiratory, and renal conditions, respectively. 34 This result demonstrated similar conditions to the most common postoperative medical complications which had been stated earlier.
The findings from our study highlight several key prognostic factors for walking disability following fragility hip fractures, including non-modifiable factors such as age, pre-fracture use of the gait aid, and comorbidities, as well as modifiable factors like preoperative hypoalbuminemia and postoperative complications. These insights can significantly impact clinical practice by informing strategies to minimize postoperative complications and improve ambulation outcomes. Addressing modifiable factors through preoperative nutritional optimization and timely surgical intervention can enhance recovery. Early and intensive mobilization, facilitated by a multidisciplinary approach is crucial for improving functional outcomes. By implementing these targeted interventions, health care providers can reduce the incidence of walking disability and improve the overall quality of life for patients with fragility hip fractures.
There are several limitations in this study. Although we attempted to collect various related factors in which the medical records were provided, the retrospective study may have resulted in incomplete data or missed variables, potentially introducing inherent bias and lacking some information. The standard CCI score was not collected in this study as we couldn’t calculate from the existing data. However, the report of each underlying comorbidity demonstrated the actual condition of the patients’ characteristics. The other variables including ASA classification, postoperative muscle strength, and Barthel index might be found relating to postoperative walking ability. Nevertheless, we couldn’t perform a prognostic factors analysis of these factors due to incomplete data of all patients from the medical records. Lastly, this present study involved only patients who underwent surgical treatment for hip fractures. Health care providers should be cautious when interpreting these data to non-surgical fragility hip fracture patients.
Conclusions
Elderly with ≥80 years of age, pre-fracture walking with the gait aid, having ≥2 underlying comorbidities, preoperative hypoalbuminemia, and the presence of postoperative medical complication, were the factors prognosticating independent walking disability within the first 6 weeks following fragility hip fracture surgery. Among these, the postoperative medical complication was realized as posing the highest risk. These factors could be utilized as the treatment plans to decrease morbidity and improve functional outcomes in those patients.
Footnotes
Acknowledgements
We are deeply grateful to Professor Jayanton Patumanond, MD, PhD, Thanin Lokeskrawee, MD, and Suppachai Lawanaskol, MD for their expert guidance in methodology and statistical analyses, which greatly contributed to the success of this research. Additionally, we extend our sincere thanks to their research team for the collaboration with our co-workers who assisted in data collection.
Author Contributions
P.C. provided data collection and analysis, wrote the original draft of the manuscript, and prepared all materials. N.T. provided data collection and commented on previous versions of the manuscript. A.L. provided data analysis and coordination, commented on and edited the manuscript. A.J. provided data analysis and coordination, wrote, supervised, and reviewed the manuscript. All authors contributed to the conceptual and methodological design of the study, read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.