
Abstract
Introduction
A negative correlation exists between functional outcomes and leg length discrepancy (LLD) following hip fracture repair. We have assessed the effects of LLD following hip fracture repair in elderly patients on 3-meter walking time, standing time, activities of daily living (ADL), and instrumental activities of daily living (IADL).
Methods
One hundred sixty-nine patients enrolled in the STRIDE trial were identified with femoral neck, intertrochanteric, and subtrochanteric fractures that were treated with partial hip replacement, total hip replacement, cannulated screws, or intramedullary nail. Baseline patient characteristics recorded included age, sex, body mass index Charlson comorbidity index (CCI) score. ADL, IADL, grip strength, sit-to-stand time, 3-meter walking time and return to ambulation status were measured at 1 year after surgery. LLD was measured on final follow-up radiographs by either the sliding screw telescoping distance or the difference from a trans-ischial line to the lesser trochanters, and was analyzed as a continuous variable using regression analysis.
Results
Eighty eight patients (52%) had LLD <5 mm, 55 (33%) between 5-10 mm and 26 subjects (15%) >10 mm. Age, sex, BMI, Charlson score, and ambulation status had no significant impact on LLD occurrence. Type of procedure and fracture type did not correlate with severity of LLD. Having a larger LLD was not found to have a significant impact on post-operative ADL (P = .60), IADL (P = .08), sit-to-stand time (P = .90), grip strength (P = .14) and return to former ambulation status (P = .60), but did have a statistically significant impact on 3-meter walking time (P = .006).
Discussion
LLD after hip fracture was associated with reduced gait speed but did not affect many parameters associated with recovery. Continued efforts to restore leg length after hip fracture repair are likely to be beneficial.
Introduction
As few as 40-60% of elderly patients with hip fractures return to their pre-injury level of mobility and capacity for performing activities of daily living. 1 Controversy exists as to whether this functional decline is more from pre-existing comorbidities and medical complications or due to the surgical outcomes that relate to the hip. Type of anesthesia, treatment with total hip or hemiarthroplasty as well as use of geriatric fracture programs have not convincingly shown improvements in functional outcomes.2-4 Fracture types and differences in surgical approach have not shown overall differences in functional outcomes despite a wide variety of fracture patterns and treatment types.5-7
Despite the lack of influence of fracture type and fixation methods, it is widely held that failed fixation leads to worse outcomes. Failure of fracture fixation may lead to severe femoral neck shortening (≥10 mm) in 12.9% 8 to 32% 9 of patients following internal fixation of femoral neck fractures. Significant shortening may also occur following repair of fractures in the trochanteric region. 10 Femoral shortening has been correlated with decreases in Harris hip scores, 8 physical functioning scores, 11 and SF-12 scores, 12 as well as increased pain and loss of mobility. 13 Patients treated with arthroplasty may also develop leg length discrepancy (LLD). Limb lengthening is more common than shortening following total hip arthroplasty and has been associated with back pain, neurologic injury, gait disorders, and patient dissatisfaction following surgery.14-19 LLD after hip fracture repair can have a notable negative impact on functional outcomes, due in large part to a decrease in the abductor moment arm accompanied by changes to gait mechanics. 12
We retrospectively assessed the radiographs of older patients (≥65 years) treated for hip fracture in the A Strategy to Reduce the Incidence of Postoperative Delirium in Elderly Patients (STRIDE) randomized trial where functional outcomes were prospectively assessed. The goal of this study was to determine to what degree functional outcomes, including activities of daily living (ADLs), instrumental activities of daily living (IADLs), and gait speed, at 1 year after surgery are affected by LLD, determined by radiograph, following hip fracture repair in an elderly population.
Methods
We conducted a secondary analysis of data from the STRIDE trial, the protocol of which was previously described in detail. 20 STRIDE was a prospective randomized trial performed at 1 academic medical center with the purpose of determining if the sedation level of patients during surgery affects delirium after hip fracture treatment. Patients included were those 65 years or older undergoing partial hip replacement, total hip replacement, intramedullary nailing, or cannulated screw fixation following femoral neck, intertrochanteric, or subtrochanteric fracture. Patients had no preoperative delirium or severe dementia and received spinal anesthesia and propofol sedation during their procedures. Patients were recruited from November 18, 2011, through May 19, 2016. Upon informed consent, 200 patients were randomized to receive either heavier (modified observer’s assessment of alertness/sedation score [OAA/S], 0-2) or lighter (OAA/S, 3-5) intraoperative sedation levels. 21 Charlson Comorbidity Index (CCI) and Geriatric Depression Scale (GDS) were measured in all patients before surgery.
Patients in the trial were followed for a year to determine functional outcomes including sit-to-stand time, 3-meter walking time, grip strength, self-reported ambulation status, ADL, and IADL. Ambulation status was determined using baseline and 12-month ADL ambulation scores and was graded as 0, 1 or 2, with 0 indicating return to baseline or improvement from baseline at 12 months, 1 indicating decline from baseline at 12 months, and 2 indicating no assessment at 12 months.
Patients included in the present analysis were those with suitable pre- and post-operative (≥ day 6) anteroposterior radiographs. Patients with anatomic abnormalities preventing accurate radiographic measurement were excluded. Of the 200 STRIDE patients, 30 were excluded in the present study due to lack of radiographs at or after post-operative day 6, and 1 was eliminated due to anatomic abnormalities preventing accurate measurement. In total, leg length discrepancy was measured in 169 patients. The mean time from surgery to measured post-operative x-ray was 290 days, and the range was 6 to 2963 days (approximately 8 years).
Fracture classifications were determined using the earliest pre-operative radiographs available with the AO Foundation and Orthopedic Trauma Association (AO/OTA) classification system. 22 LLD was determined using radiographs from the 1-2-year post-operative range when available so as to match timing of physical functioning data collection as best possible. LLD of patients with hip screw fixation (sliding hip screw and side plate as well as intramedullary hip screws) was determined through measurement of subsidence of the sliding screw. As previously described by Serrano et al, the entire length of the screw was measured and compared against the length of the screw medially. 23 The standard screw diameter of 10.5 mm was used to scale the measurements.
LLD of patients with partial or total hip replacements or cannulated screws was determined by measuring from each lesser trochanter to a trans-ischial line drawn to intersect both ischial tuberosities (Figure 1).
24
When 1 or both lesser trochanters were absent, the greater trochanters were used. The prosthetic head diameter as confirmed by the surgical notes was used to scale the measurements. LLD in patients with partial/total hip replacements or cancellous screws was measured as the difference in distance from the less trochanters to a trans-ischial line. The known prosthesis head diameter was used to scale the measurements.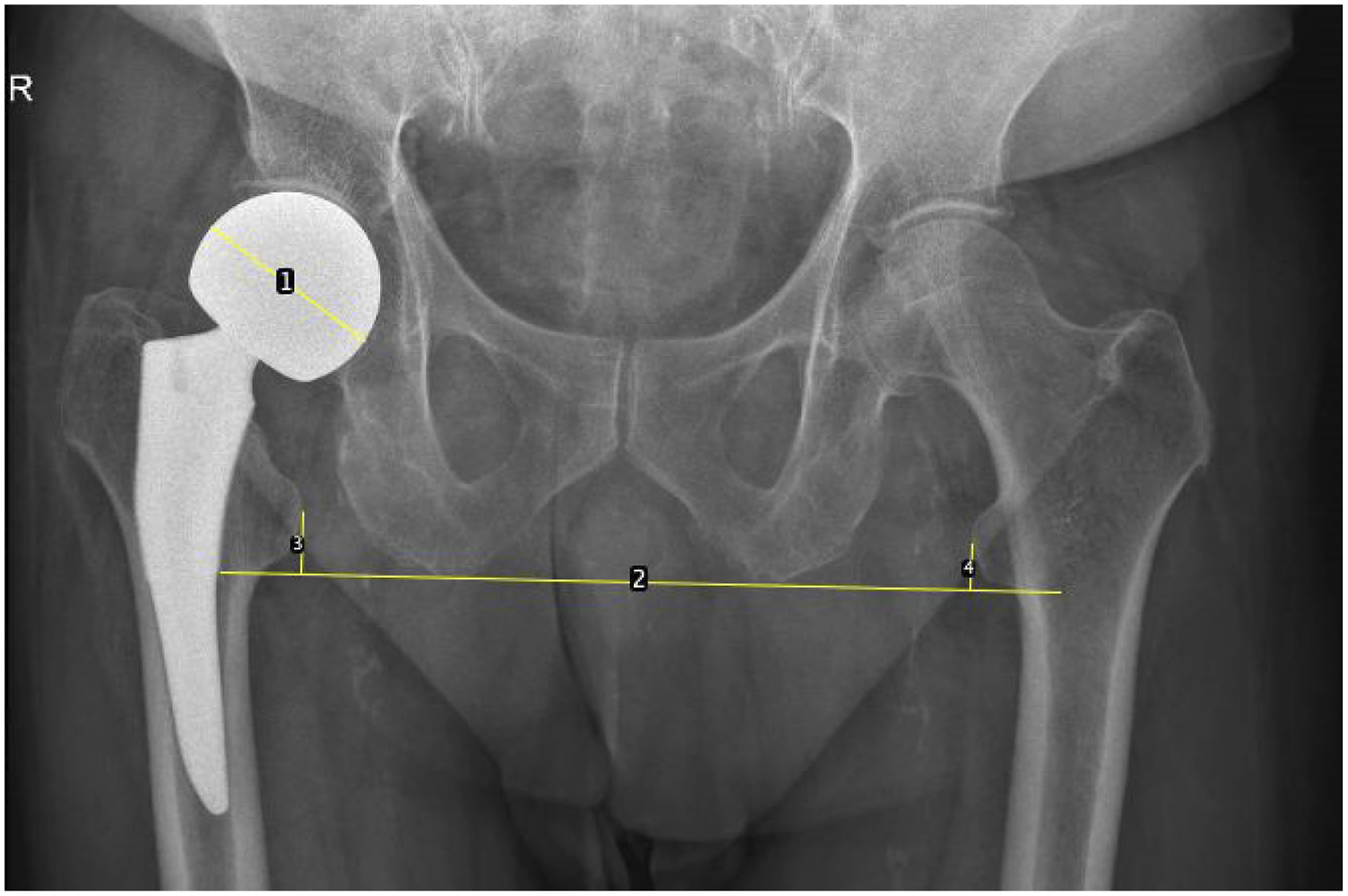
Baseline Patient Characteristics.

Patient characteristics were described using mean and standard deviation (SD) for continuous variables and frequency distribution for categorical variables. LLD, defined as either shortening or lengthening on the affected side, was analyzed both as a continuous measure of absolute discrepancy in mm and a categorical variable of 3 discrepancy severity levels, defined as none to mild (<±5 mm), moderate (±5 to ±10 mm inclusive), and severe (±10 mm) LLD. 25 Bivariable association between baseline characteristics and LLD severity levels was analyzed using analysis of variance F-test for continuous baseline characteristics and chi-square or Fisher’s exact test for categorical baseline variables. Association of functional outcomes of ADL, IADL, ambulation status, sit-to-stand time, 3-meter walking time, and grip strength at 12 months with absolute discrepancy of LLD were assessed using general linear model adjusting for relevant baseline characteristics. Analyses were conducted using SAS version 9.4. A P-value <.05 was considered statistically significant.
Results
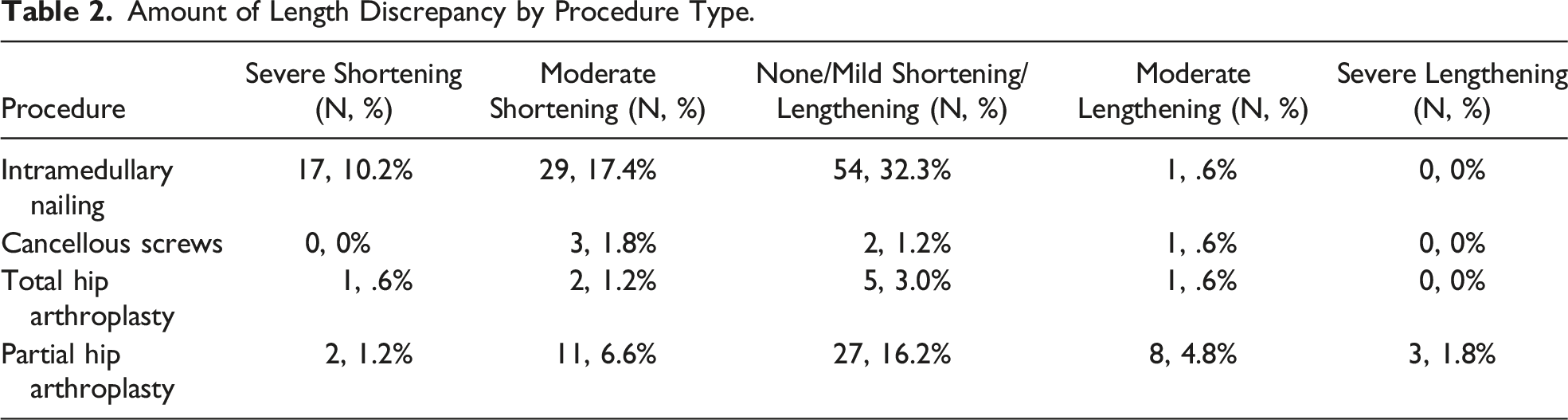
Amount of Length Discrepancy by Procedure Type.
The total mean ADL was 4.24. Patients having a LLD discrepancy severity level of 2 (severe shortening or lengthening) had the lowest mean ADL at 3.83. Patients with a LLD discrepancy severity level of 1 (moderate shortening or lengthening) had a mean ADL at 4.46. while patients with a LLD discrepancy severity level of 0 (no/mild LLD) had a mean ADL score of 4.22. Overall, having a larger absolute discrepancy in postoperative LLD was found to have no significant impact on post-operative ADL (P = .60) at 12 months after surgery.
The total mean IADL score was 4.87. Patients having a LLD discrepancy severity level of 2 had the lowest mean IADL at 4.04. Patients with LLD discrepancy severity levels of 0 and 1 had mean IADL scores of 5.14 and 4.98, respectively. Although the association between IADL and LLD seemed to show a stepwise pattern, having a larger absolute discrepancy in postoperative LLD did not have statistically significant impact on post-operative IADL (P = .08) at 12 months after surgery.
Most patients (n = 100, 59.17%) had a post-operative ambulation status of 1, indicating a decline in ADL ambulation score at 12 months compared to baseline. 48 patients (28.40%) had a post-operative ambulation status of 0, indicating maintained or improved function compared to baseline, and 21 patients (12.43%) had no measurement at 1 year. Having a larger postoperative LLD was found to have no significant impact on return to former ambulation status at 12 months after surgery (P = .60).
The total mean 3-meter walking time was 6.48 seconds. The LLD cohort with discrepancy severity level of 0, 1 and 2 showed a stepwise pattern in the mean walking time, at 6.10, 6.62, and 7.51 seconds, respectively. A statistically significant overall association was found between walking time and absolute discrepancy of LLD (P = .006, Figure 2). Our analyses found no correlation between LLD and IADL, ADL, or sit-to-stand time. There was, however, a positive correlation between LLD and 3-meter walking time.
The total mean sit-to-stand time was 1.81 seconds. The LLD cohorts with discrepancy severity level of 0, 1, and 2 had the mean sit-to-stand time of 1.75, 1.89 and 1.87 seconds, respectively. Having a larger absolute discrepancy in postoperative LLD was found to have no significant impact on sit-to-stand time (P = .90), nor with grip strength (P = .14) at 12 months after surgery.
Discussion
The 3-meter walking time was the sole functional outcome at 12 months post-surgery found to be associated with LLD. This is consistent with previous studies that have shown that LLD after internal fixation in geriatric populations can lead to poorer walking function. 26 Our data is consistent with the biomechanical report by Zielinski et al, which found lower gait velocity in individuals with severe femoral neck shortening after internal fixation when compared with those having no/mild shortening (.8 to 1.2 m/s vs 1.0 to 1.3 m/s). 27 Studies addressing LLD after THA have also confirmed that smaller LLD leads to a faster gait in these cohorts. 15
The increase in walking time with larger LLD may be related to changes such as a shorter stance time, increased painful weightbearing on the fractured leg in stance, and a shorter single support phase, all of which were reported by Zielinski et al. for patients with severe shortening. 27 In contrast, Zhang et al reported a longer single support phase in patients with larger LLD after THA. This suggests that there are differing biomechanical explanations for loss of gait economy after internal fixation vs arthroplasty, which may be linked to the prevalence of lengthening rather than shortening after THA. Other functional outcomes were unaffected by LLD. IADL, ADL, post-operative ambulation status, and sit-to-stand time may have been unaffected due to the limited baseline function of older patients. As would be predicted, post-operative grip strength was not influenced by LLD amount.
Previous studies have also shown that LLD can affect outcomes in a gradient fashion. Zlowodzki et al showed that both moderate and severe shortening had a significant impact on short form-36 (SF-36) physical functioning scores when compared to no/mild shortening, but that severe shortening had the greatest influence, with mean scores of 74 for no/mild shortening (indicating lower disability), 53 for moderate (indicating mild disability), and 42 for severe (indicating higher disability). 11 While our study did not report SF-36 outcomes, comparable physical function measures such as ambulation status, grip strength, sit-to-stand time, and 3-meter walking time did not demonstrate a significant difference between moderate and severe LLD groups.
We found no to mild LLD in half of patients and moderate LLD in one-third of patients. Only 1 in 6 patients experienced severe LLD. Other studies have found severe shortening to be present in a larger proportion of their cohort but have not typically included arthroplasty in their analysis. Indeed, the study by Crosby and Parker on elderly patients undergoing internal fixation demonstrated severe shortening in 25% of the cohort. 13 Another study on LLD after fixation with multiple parallel screws or sliding hip screws found moderate femoral shortening to occur in 36% of patients and severe shortening to occur in 30% of patients. 11 Zlowodzki et al found nearly equal distribution of mild, moderate, and severe shortening in their study in which the mean age of their study participants was 71. 11
The present study demonstrated a mean LLD of −3.48 mm, falling within the range that might be expected for a cohort that includes both internal fixation and arthroplasty. The study by Zielinski et al. showed a median LLD of −11 mm after 22 months in internal fixation patients ranging in age from 61.6 years to 78.4 years. 27 Similarly, Crosby and Parker found a mean fracture collapse of 8.0 mm (0-20 mm) for an internal fixation cohort in which the mean age was 76.1 years (24-101 years). 13 In contrast, the study by Roder et al identified just 30 cases of shortening greater than 10 mm in a cohort of 10 415 THA patients, as compared to 405 cases of lengthening greater than 10 mm. Furthermore, Papadopoulos et al found a mean postoperative LLD of 1.58 mm (−8 mm to 7 mm) in their THA cohort with a mean age of 71 years.
Our study did not determine an association between age and LLD after hip fracture surgery. The correlation between age and LLD has been debated in the literature. Some studies in younger populations have shown that femoral shortening and fracture collapse after dynamic hip screw (DHS) fixation are predisposed by old age, 26 while others have shown no association between age and LLD. 8 In the study by Zielinski et al focused on patients 50 to 80 years old, LLD was in fact shown to be influenced by patient age, weight, and Pauwels fracture classification. 27 Crosby and Parker also found there to be a slight increase in fracture collapse with age, particularly in those who had experienced undisplaced fractures. 13 We also found BMI to have no significant impact on LLD. Previous reports have demonstrated a positive correlation between weight and LLD, and some have also shown a correlation between BMI and LLD.27,28
While we did not find any association between procedure type and amount of LLD, other studies have shown that cancellous screws or non-sliding screws result in less femoral shortening than sliding screws. 9 Indeed, in the study by Boraiah et al, only non-sliding hip screws were used in their cohort of 54 patients and fracture healing complication occurred in just 6% of patients. 29 Similarly, Lin et al treated 41 hip fracture patients with static locking plates, and fracture healing complications occurred in only 15% of individuals. 30 Previous studies have found limb lengthening to be a more common occurrence in hip arthroplasty than shortening, but have also demonstrated shortening to have a more significant impact on outcomes. 17
Our results did not suggest that fracture pattern has an impact on LLD in older populations. However, previous reports have found that patients with displaced or comminuted fractures have an increased chance of developing LLD.8,26 Crosby and Parker found the difference in mean collapse between displaced and undisplaced fractures to be 9.5 mm and 5.9 mm, respectively. In regards to AO/OTA fracture classifications, 31. A2 has been correlated with increased fracture collapse, 26 and B2 fractures have been shown to cause significantly increased LLD when compared to B1 and B3. 28 Differences between our findings and other studies could be due to the fact that we evaluated both arthroplasty and fracture fixation methods.
There are several limitations to our current study. First, this project was a retrospective review of a prospective study that was not powered to look at hip fracture outcomes and LLD. Our study had variability in radiographic follow-up times, which may have impacted measured LLD. However, Haider et al measured femoral shortening on radiographs from 3-month as well as 5-year follow-ups and noted that there was generally not an increase in the LLD with elapsed time. 28 Another limitation of our study is the difference between the methods used to measure LLD after hip arthroplasty and internal fixation, as this may have introduced some level of treatment variability. Measurements of x-rays also may have inaccuracies based on difficulties in seeing landmarks. 24 Finally, like other studies, we were not able to eliminate possible pre-existing LLD as a confounding variable.
Clinical Relevance
Our assessment of LLD following hip fracture repair is clinically important because LLD has been shown to lead to pain, osteoarthritis of the knee/hip/spine, and changes in gait.27,31 In the study by Roder et al, both lengthening and shortening after THA resulted in increased limping and decreased patient satisfaction. 17 Interestingly, only lengthening resulted in a decrease in walking capacity. Regardless of the discrepancy, restoration of leg length equality (LLE) should be a central aim in any hip fracture surgery.
LLD can be difficult to avoid in hip arthroplasty, as the surgeon must ensure adequate soft tissue tension (a task that may result in lengthening), while avoiding the stretching of the sciatic nerve (a task that may result in shortening). 32 LLE can nonetheless be achieved through attention to offset, socket position, and neck length. 14 Generally, 0-5 mm of leg lengthening should be considered adequate for soft tissue tensioning. 16 For internal fixation, surgeons may consider the use of static devices. Given the findings by Lin et al and others, the use of non-sliding screws or static locking plates may be advantageous.11,30 However, this approach must also be treated with caution, as a study by Berkes et al reported catastrophic failure for 37% of their cohort treated with static locking plates. 33 Our study helps to confirm the necessity of measures such as those above in preventing significant LLD.
Conclusion
There was a significant increase in 3-meter walking time with increased LLD with no evident impact of LLD on more general outcomes of recovery such as ADLs and IADLS. Continued efforts should be made to reduce anatomical leg length discrepancy, especially in surgical technique, as this can help achieve optimal mobility and patient satisfaction outcomes in geriatric populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by National Institute on Aging grant R01 AG033615 and National Center for Advancing Translational Sciences UL1TR003098.
Trial Registration
Trial Registration clinicaltrials.gov Identifier: NCT00590707.