
Abstract
Introduction:
Twenty-five percent to seventy-five percent of independent patients do not walk independently after hip fracture (HF), and many patients experience functional loss. Early rehabilitation of functional status is associated with better long-term outcomes; however, predictors of early ambulation after HF have not been well described.
Purposes:
To assess the impact of perioperative and patient-specific variables on in-hospital ambulatory status following low-energy HF surgery.
Methods:
This is a retrospective analysis of 463 geriatric patients who required HF surgery at a metropolitan level-1 trauma center. The outcomes were time to transfer (out of bed to chair) and time to walk.
Results:
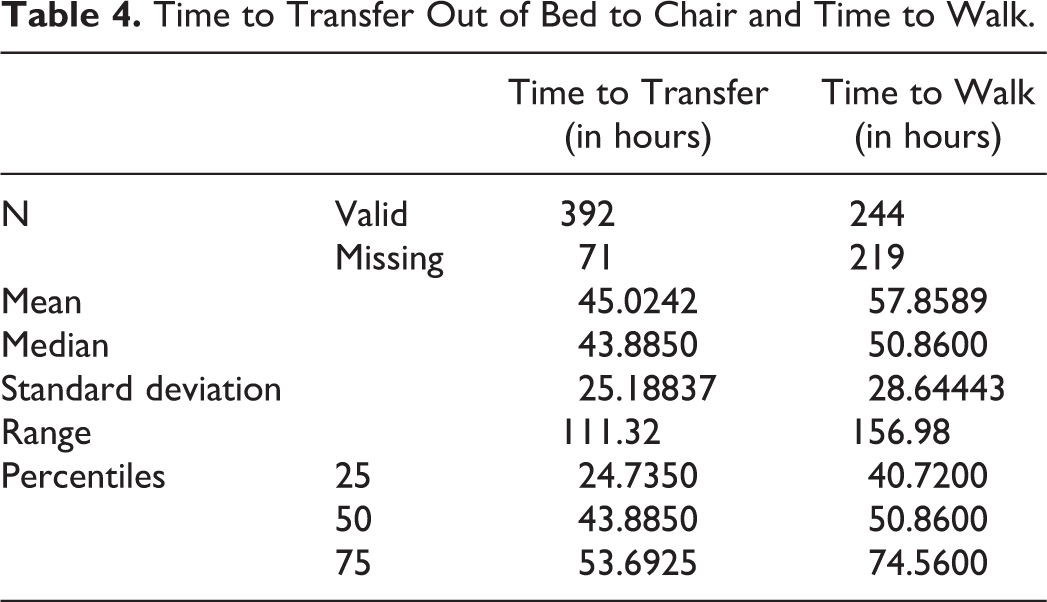
Three hundred ninety-two (84.7%) patients were able to transfer after surgery with a median time of 43.8 hours (quartile range: 24.7-53.69 hours), while 244 (52.7%) patients were able to walk with a median time of 50.86 hours (quartile range: 40.72-74.56 hours). Preinjury ambulators with aids (hazard ratio [HR]: 0.70, confidence interval [CI]: 0.50-0.99), age >80 years (HR: 0.66, CI: 0.52-0.84), peptic ulcer disease (HR: 0.57, CI: 0.57-0.82), depression (HR: 0.66, CI: 0.49- 0.89), time to surgery >24 hours (HR: 0.77, CI: 0.61-0.98), and surgery on Friday (HR: 0.73, CI: 0.56-0.95) were associated with delayed time to transfer. Delayed time to walk was observed in patients over 80 years old (HR: 0.74, CI: 0.56-0.98), females (HR: 0.67, CI: 0.48-0.94), peptic ulcer disease (HR: 0.23, CI: 0.84-0.66), and depression (HR: 0.51, CI: 0.33-0.77).
Conclusions:
Operative predictors of delayed time to transfer were surgery on Friday and time to surgery >24 hours after admission. Depression is associated with delayed time to transfer and time to walk. These data suggest that is important to perform surgeries within 24 hours of admission identify deficiencies in care during the weekends, and create rehabilitation programs specific for patient with depression. Improving functional rehabilitation after surgery may facilitate faster patient discharge, decrease inpatient care costs, and better long-term functional outcomes.
Introduction
Hip fractures (HFs) are a major public health concern because of their prevalence, high costs, and poor postsurgical outcomes. 1,2 Hip fracture is the second most common osteoporotic fracture with an incidence of 794 per 100 000 females and 369 per 100 000 males in 2004. 1 Although HFs are more common in females, males are known to have higher postoperative morbidity and mortality (33% at 1 year). 1,3 -6 In addition, HFs represent total inpatient care costs reaching up to 6 billion dollars per year. 7 Lastly, 25% to 75% of functionally independent patients do not walk independently after HF, and many patients experience functional loss related to impaired balance and mobility. 2,8,9
Evidence-based clinical practice guidelines regarding management of HFs have recommended early assisted ambulation within 48 hours after HF surgery. 10 Early ambulation may prevent loss of muscle strength, 11 improve the level of assistance required to walk, and improve walking distance. 10 Furthermore, early ambulation may contribute to shorter length of stay (LOS) and result in lower levels of functional dependency at discharge from acute care. 12 Delay in standing is associated with deterioration of functional recovery at 1 month, lower levels of self-care, less ability to transfer, worse locomotion at 2 months, and higher mortality at 6 months when controlling for preoperative immobility. 10,12,13
Short- and long-term functional outcomes after HF surgery have been extensively studied. 12 -18 However, few studies have evaluated the in-hospital ambulatory status following HF surgery. 10,19,20 Furthermore, while it is well-established that postoperative morbidity and mortality are greater in males than in females, there is a paucity of data regarding gender differences on in-hospital ambulatory status. 1,5,6 Therefore, the aim of this study is to assess the correlation of perioperative and patient-specific variables with in-hospital ambulatory status using time to transfer (out of bed to chair) and time to walk after HF surgery as outcomes. Due to the multifactorial nature of perioperative recovery, it is necessary to assess the relationships between ambulatory status and patient-specific, preoperative, and operative factors. This may allow clinicians to better identify modifiable factors that may prolong postoperative physical therapy (PT) and ambulatory recovery. In addition, we analyzed whether gender is an independent predictor of time to transfer and time to walk after HF surgery when controlling for covariates. We hypothesized that there are identifiable perioperative risk factors that can delay the time to transfer and time to walk after HF surgery and that male gender is a predictor of delayed improvement in ambulatory status after HF surgery.
Methods
Patients
A retrospective analysis was performed in all patients over 50 years old admitted for surgical repair of HF between January 2013 and December 2014. This study utilized our institutional Fragile Bone Registry, and approval was granted by our institutional review board prior to initiation of the study. Patients were initially identified using the hospital daily orthopedic trauma list. Subsequent information was gathered from the electronic records. Inclusion criteria were (1) diagnosis of femoral neck or intertrochanteric HF and (2) recorded discharge date (n = 548). Exclusion criteria (Table 1) consisted of patient conditions or chart characteristics that would likely confound ambulation or data analysis, including (1) pathological, atypical, periprosthetic, and chronic fractures (n = 11); (2) nonunion HF (n = 1); (3) combined femoral neck and femoral shaft fracture (n = 1); (4) concomitant acetabular, pelvic, or humerus fracture (n = 13); (5) high-energy fractures (n = 2); (6) patients treated conservatively (n = 1); (7) contralateral HF in the last year (n = 2); (8) preinjury nonambulatory patients (n = 3); (9) incomplete chart information (n = 38); (10) age younger than 50 (n = 12); and (11) atypical fracture (n = 1). Eighty-five patients were excluded from the analysis, resulting in 463 patients included in this study.
Patients Excluded From Analysis.

Assessment
Data were collected from the electronic database records by authors V.J. and K.J. Information gathered through admission notes, anesthesia records, operative notes, and postoperative notes included age, gender, preinjury ambulatory status, side of fracture, fracture type, time to surgery, surgical intervention, American Society Anesthesiologist score (ASA), 21 type of anesthesia, blood loss, operating room (OR) day of the week, associated medical comorbidities, postoperative pain management (patient-controlled analgesia [PCA]), ambulatory status during each PT session, and presence of pain at time of PT, as stated in the PT note.
Predictors of Ambulatory Status
Preinjury ambulatory status was categorized as “independent” when patient did not require any assistive devices or “ambulator with aids” when patient required assistive devices (ie, cane, walker). Type of HF was categorized as femoral neck fracture or intertrochanteric fracture. The ASA rating scale was used to assess the role of severity of comorbidities at time of admission, as described by Owens et al. 21 Patients were categorized as ASA 1-2 or ASA 3-4. No patients with ASA 5 were identified. Time to surgery was determined by the time between admission, as reported in the admission note, and initiation of anesthesia and was classified as ≤24 hours or >24 hours. Type of surgery was reported as hemiarthroplasty, total hip arthroplasty (THA), cephalomedullary nailing (CMN), and open reduction internal fixation which includes percutaneous pin fixation (closed reduction percutaneous pinning [CRPP]). The amount of blood loss was obtained from the operative report and was intraoperatively estimated in milliliters. In addition, comorbidities were included (Table 2) as patient-specific variables that may have negative impact on functional status within this population. 6,20,22 -25 Presence of PCA and pain at the time of PT were evaluated from postoperative day (POD) 1 to 5 to assess postoperative care that may influence early ambulation.
Included Patients With Comorbidities.

Abbreviations: AIDS, acquired immune deficiency syndrome; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; MI, myocardial infarction; PCA, patient-controlled analgesia.
a Peripheral disease include aneurysm >6 cm.
b Cerebrovascular disease (CVA with mild or not residua or transient ischemic attack).
c Excluded if >5 years from diagnosis.
d Leukemia acute or chronic.
Ambulatory Status
In order to assess the ambulatory status after surgery, all electronic PT notes from POD 1 through the patient’s day of discharge were reviewed. Physical therapy sessions were performed once or twice per day during the weekdays and once a day during the weekends. Each session was performed every POD with the assistance of two therapists. Therapists documented encounter time, duration, type of activity, walking distance reached by the patient, and the amount of assistance given by those assisting. In-hospital ambulatory status was categorized in PT notes as: (1) patient is confined to bed; (2) patient stood, no steps; (3) steps by the bed and to the chair (1-3 ft); (4) walked inside the room (4-24 ft); and (5) walked outside the room (>25 ft). Those categories were grouped into 2 categories: (1) nonambulatory, (2) transfer (out of bed to chair), and (3) ambulatory (either in the hospital room or outside the room). The level of assistance required for transfer or ambulation was reported according to the suggested terminology for objective data, using definitions from the Adult Functional Independent Measure. 26 For analysis purposes, levels of assistance were grouped into: (1) complete independence, close supervision, and contact guarding; (2) minimal and moderate assistance; and (3) maximal and total assistance. Finally, time to transfer and time to walk were defined as the amount of time between surgery (anesthesia start time) and the first PT assessment in which the patient was able to transfer and ambulate, respectively, with any kind of assistance.
Statistical Analysis
Data entry was performed using a spreadsheet application (Excel 2010, Microsoft Corp, Redmond, Washington). Descriptive statistics are presented as frequencies and percentages for categorical variables. Median and quartile ranges were used to describe time to transfer and time to walk because the data are not normally distributed in our population. Multivariable cox proportional hazards modeling was used to compare time to transfer and time to walk while correcting for covariates. Ambulatory status and level of assistance required to walk was compared between groups using χ2 tests. Statistical tests were performed using SAS version 9.3 (Cary, North Carolina) and SPSS 20.0 (IBM, Armonk, New York) with significance level of α = .05.
Results
Descriptive Data
A total of 548 consecutive patients were admitted to our institution with the initial diagnosis of fragility HF. Eighty-five patients were excluded (Table 1) resulting in the inclusion of 463 patients (mean age: 81.1 years; range: 51-102) of which 72.4% were females. The clinical demographic characteristics are shown in Table 3. American Society Anesthesiologist 3 to 4 and general anesthesia were more common in males when compared to females (P < .01 and P = .04, respectively). Hypertension was the most common comorbidity in both females and males (57% and 60.2%, respectively). In males, history of myocardial infarction (P < .01), diabetes mellitus (P < .01), and renal disease (P < .01) were more common when compared to females (Table 2).
General Characteristics of Study Population.

Abbreviations: ASA, American Society of Anesthesiologists; ORIF, open reduction internal fixation; TFN, trochanteric fixation nail; THA, total hip arthroplasty.
Time to Transfer and Time to Walk
Total number of patients who transfer out of bed to chair after surgery was 392 (84.7%) with a median time of 43.88 hours (quartile range: 24.73-53.69 hours). Total number of patients who were able to ambulate was 244 (52.7%) with a median time of 50.86 hours (quartile range: 40.72-74.56 hours; Table 4). The percentage of patients who were able to transfer out of bed to chair or walk each POD is represented in Figure 1. The level of assistance required to transfer from bed to chair is represented in Figure 2, and the level of assistance required to walk is represented in Figure 3. The majority of evaluated patients were able to transfer with minimal to moderate assistance from POD 1 to POD 5 (range 64% to 69%), while the majority of patients who were able to ambulate had complete independence, contact guard, or close supervision (range 45% to 68%). There was a tendency to decrease the level of assistance after each day. Figure 4 shows an analysis of the dose–response relationship between PT and percentage of patients able to transfer with 46% of patients transferring after 1 session, 28% after 2 sessions, 18% after 3 sessions, and 8% after 4 sessions. Figure 5 shows that 22% of patients were able to ambulate after 1 PT session, 30% after 2 sessions, 24% after 3 sessions and, 24% after 4 sessions.
Time to Transfer Out of Bed to Chair and Time to Walk.
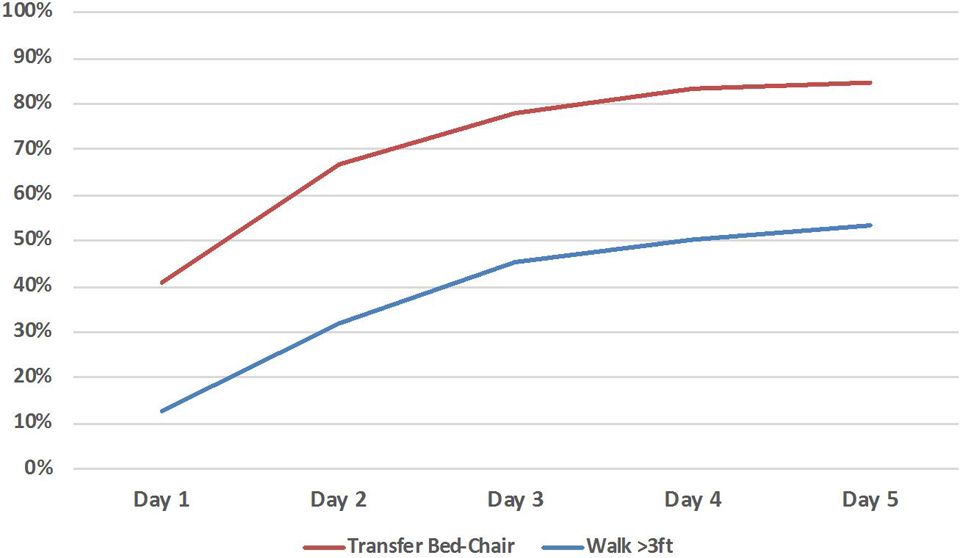
Percentage of patients able to transfer or walk per day.

Level of assistance required to transfer from bed to chair after hip fracture surgery.

Level of assistance required to walk after hip fracture surgery.
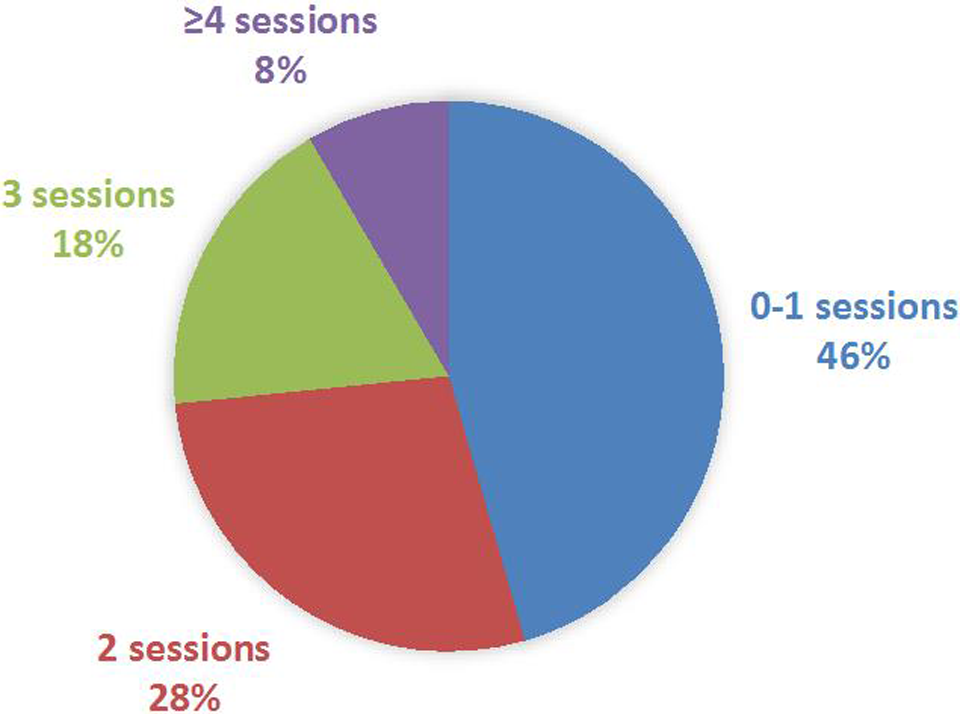
Patients able to make bed to chair transfer by number of physical therapy sessions.
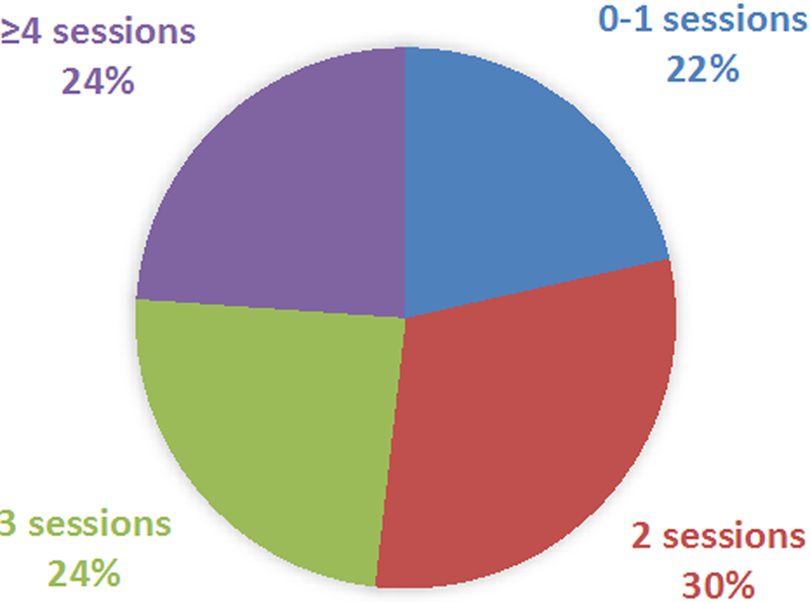
Patient able to walk by number of physical therapy sessions.
Delayed time to transfer was observed in patients over 80 years old (hazard ratio [HR]: 0.66, confidence interval [CI]: 0.52-0.84; P = .001), preinjury ambulators with aids (HR: 0.70, CI: 0.50-0.99; P = .46), and diagnoses of peptic ulcer disease (HR: 0.57, CI: 0.57-0.82; P = .04) and depression (HR: 0.66, CI: 0.49-0.89; P = .007). Earlier time to transfer was observed in patients with anemia (HR: 1.84, CI: 1.16-2.91; P = .009). Preoperative and operative variables associated with delayed time to transfer were surgery >24 hours after admission (HR: 0.77, CI: 0.61-0.98) and surgery on Friday (HR: 0.73, CI: 0.56-0.95). No significant difference in time to transfer was found between males and females after correcting for confounding variables as shown in Figure 6.

Probability and time to transfer by gender.
Delayed time to walk was observed in patients over 80 years old (HR: 0.74, CI: 0.56-0.98; P = .02), diagnoses of peptic ulcer disease (HR: 0.23, CI: 0.84-0.66; P = .06), and depression (HR: 0.51, CI: 0.33-0.77; P = 0.02). Earlier time to walk was observed in patients with anemia (HR: 3.44, CI: 1.58-7.47; P = 0.002). Significant differences in time to walk were found between males and females with males outperforming females (HR: 0.67, CI: 0.48-0.94) as shown in Figure 7.

Probability and time to walk by gender.
Discussion
The main findings in this study were that age over 80 and certain comorbidities (eg, depression and peptic ulcer disease) were risk factors for delayed time to transfer out of bed to the chair and delayed time to walk following HF surgery. Preinjury ambulatory status requiring aids was also associated with delayed time to transfer. In addition, preoperative and operative prognostic factors for delayed time to transfer were time to surgery >24 hours and surgery on Friday. Finally, it was found that gender was not associated with time to transfer but was associated with time to walk after HF surgery.
This study has several limitations. First, the retrospective design limits control over data collection. Therefore, as an observational study, we are limited to identifying associations and not causal relationships. Second, 90% of the study population was Caucasian and therefore, the data may not reflect the general population. Third, the number of patients with specific comorbidities was small in certain cases and therefore difficult to draw conclusions on these findings. Fourthly, dichotomization of outcomes was necessary for analysis purposes, resulting in substantial loss of information. However, it allows easy clinical identification of patients who would present delayed time to transfer or time to walk.
Despite limitations, this large retrospective cohort study assessed the impact of several epidemiologic, perioperative, and patient-specific factors on in-hospital ambulatory status. It is important to identify factors that can delay ambulation since ambulation within 48 hours after HF surgery have been associated with lower incidence of deep vein thromboembolism, less pulmonary complications, less skin breakdown, decreased rates of mental status decline, and improvement in physical independence. Furthermore, return of ambulatory function is one of the major goals of care for patients prior to discharge, and therefore delayed ambulation can significantly increase patients’ LOS and costs. 20,27,28
Preoperative factors correlated with delayed time to transfer or time to walk include preinjury ambulatory status and age of the patient. Patients walking with assistive devices before their injury were found to need more time to transfer postoperatively when compared to patients who walked independently before the surgery. Similar association was also found when evaluating inpatient rehabilitation hospital outcomes at the time of discharge and 1 month after surgery. 13,18 However, to our knowledge, there are no studies evaluating the in-hospital ambulation status. 20 Results in this study showed that patients older than 80 years have delayed time to walk after HF surgery. Similar results were found when evaluating an early ambulation program after HF. 19,20 It is suggested that poorer nutrition and number of comorbidities are factors that may contribute to this association. 19
The comorbidities found to be associated with delayed time to transfer and time to walk after HF surgery were presence of peptic ulcer disease and depression. The finding of delayed time to transfer and time to walk in patients with peptic ulcer disease is supported by studies showing that peptic ulcer disease is associated with increased risk of delirium after HF surgery. 29 The definition of peptic ulcer disease includes the use of proton pump inhibitors and may represent previous hospitalizations, frequent interaction with the health-care system, or polypharmacy. 30 The use of proton-pump inhibitors has also been associated with increased risk of HF and periprosthetic fracture after primary THR possibly due to decreased calcium absorption. 31 However, in this population, the number of patients presenting peptic ulcer disease was small (3.7%; Table 2), and therefore caution is advised with drawing conclusions from these results. Patients with depressed have shown to have inferior functional outcomes, longer LOS in rehabilitation centers, and decreased rehabilitation participation. 3 This may be secondary to lack of motivation and/or energy to sufficiently participate in rehabilitation. Furthermore, depression is aggravated by the experience of a fall-related fracture and hospital stay. 32 Additionally, anemia was associated with a faster time to walk. The small number of patients with anemia (7.3%) could explain why they were correlated with faster time to walk. Previous studies have shown that preoperative anemia is associated with increased mortality, poorer physical function, and lower health-related quality of life after HF surgery. Furthermore, perioperative blood transfusion and predischarge anemia have shown no effect in outcomes. 33,34 Our results showing that patients with anemia were able to transfer out of bed to chair 1.07 hours faster (median; 26.9 hours) than patients without anemia (median: 27.97 hours) were statistically significant but are not clinically relevant, and this difference could represent variations in PT encounter time.
Regarding perioperative factors associated with bed to chair transfer, this study demonstrated that surgery performed 24 hours after admission was associated with delayed time to transfer. Several studies have failed to find a correlation between time to surgery and in-hospital functional outcomes, but a previous study done in this institution showed that patients having surgery >48 hours from admission were less likely to walk by POD3 when compared to patients having surgery <48 hours from admission. 10,19,20,35 Furthermore, it has been shown that surgery >24 hours after admission for HF is associated with increased pain which might partially explain our results. 36,37 As time to surgery increases, morbidity, LOS, and total hospital costs progressively increase. 38 To our knowledge, this is the first study evaluating the association between time to surgery and ambulatory status, and level of assistance. We demonstrated that patients having surgery >24 hours after admission are less likely to transfer at the time of discharge (P = .04). This suggests that time to surgery is a predictor of time to transfer regardless of the amount of assistance required during PT. Delayed surgery is often related to medical instability or the presence of a correctable condition that required initial stabilization; however, the majority of cases of delay are due to system problems such as timely consultation, absence of OR space, or availability of the surgeon. 36,37,39 Therefore, it seems feasible to decrease the time to surgery after patient admission with more coordinated fracture care pathways with the goal to improve functional outcomes after HF surgery.
Surgery performed on Friday was also associated with delayed time to transfer, and this echoes the results of Barone et al. The lower number of physical therapists available during the weekends, the absence of medical orthopedic trauma service meetings, and the decreased presence of mid-level providers through the day to address patient needs might explain this finding. Lack of patient continuity among weekend PT staff and nursing staff may be a contributing factor. Surgery performed on Saturday was not associated with delayed time to transfer or time to walk; however, this is limited by our small sample size of surgery on this day (n = 20). Further studies should be done to assess the associations of surgery day and time to walk in larger groups of patients. Operating room availability and greater coordination between physical therapists and the orthopedic team on weekends may achieve optimal return of ambulatory function before discharge. 19
In this study, there was no difference in time to transfer when comparing males versus females. This lack of gender differences has also been reported in long-term functional outcome studies. 3,14,17,18,40 –42 We found that males with HF presented more comorbidities, had significantly higher ASA rating, and as consequence were more likely to receive general anesthesia as reported previously. 19,23 However, when including these factors as covariates in statistical analysis, gender was not an independent factor affecting time to transfer. There was significant difference in time to walk when comparing males versus females but was not clinically significant as seen in Figure 7.
In conclusion, significant predictors of time to transfer out of bed to the chair and time to walk after HF surgery were preinjury ambulatory status, age over 80, and specific comorbidities (eg, peptic ulcer disease and depression). Preoperative and operative factors directly associated with delayed time to transfer were general surgery on Friday and time to surgery >24 hours after admission. Based on the findings of this study, we recommend increased awareness for patients with specific risk factors for delayed time to transfer out of bed to the chair. Further, we recommend efforts to identify deficiencies in care during the weekends, to perform surgeries within 24 hours from hospital admission if possible, and to create rehabilitation pathways aiming to improved outcomes in patient with diagnoses of depression.
Footnotes
Author’s Note
Jordan C. Villa is now affiliated with Department of Orthopaedic Surgery and Rehabilitation, Howard University, Washington, DC.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Joseph M. Lane is consultant from Agnovos, Amgen, Inc Bone Therapeutics, SA, CollPlant, Inc. Graftys, Kuros, Lilly, Inc and is currently receiving research support from Merck, Inc and NIH.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Institutional Review Board (IRB) approved #1301013433.