
Abstract
Introduction
The surgical approach of hemiarthroplasty for displaced femoral neck fractures remains debated. The study objective was to compare in-hospital outcomes for geriatric displaced femoral neck fractures treated with hemiarthroplasty based on surgical approach (direct lateral vs. posterior approach).
Materials and Methods
This retrospective cohort study included geriatric patients (≥60 y/o) admitted 7/1/2016-3/31/2020 treated with hemiarthroplasty. Outcomes included: operative time (incision to closure), length of stay (HLOS), and blood loss volume (mL). The Harding direct lateral approach was compared to the posterior approach; P < .05.
Results
There were 164 patients (59% direct lateral, 41% posterior). Patients treated with the direct lateral approach had an advanced directive (P = .03), dementia, (P = .03), or were functionally dependent (P = .03) more often than patients treated with the posterior approach. Time to surgery was comparable between groups (P = .52). The direct lateral approach was associated with a shorter operative time (2.3 vs. 2.8 h, P = .03), a longer HLOS (5.0 vs. 4.0 days, P < .01), and a lower median volume of blood loss (50 vs. 100 mL, P = .01), than the posterior approach, respectively. In a stratified analysis, for those who were not functionally dependent, did not have dementia or an advanced directive, the direct lateral approach led to a longer HLOS (P = .03) and shorter operative time (P = .04) than the posterior approach. Whereas among those who were functionally dependent, had dementia or had an advanced directive, the direct lateral approach led to less blood loss (P = .02) than the posterior approach.
Discussion
While those treated with the direct lateral approach lost significantly less blood, they had a significantly longer HLOS than those treated with the posterior approach. Comorbidities significantly modified outcomes, which may suggest their presence could assist with treatment decisions.
Conclusions
This study found neither approach, the direct lateral nor posterior, to be superior. Surgical approach could remain physician preference.
Keywords
Introduction
In North America, there are approximately 320,000 hip fractures annually, with femoral neck fractures making up half of these cases. 1 Hemiarthroplasty (HA) is one of the most common procedures for the treatment of femoral neck fractures.1,2 There are several described surgical approaches to HA, although a vast majority (∼80%) of HAs are performed via the posterior or direct lateral approach.3-6 The posterior approach, first described in 1940, involves disrupting the hip capsule, dividing the gluteus maximus, and detaching the external rotators.3,4,7 In contrast, the direct lateral approach involves transecting the anterior portion of the gluteus medius and vastus lateralis muscles, then suturing these back together again, while the posterior capsule remains intact.4,6 There remains controversy as to which approach, posterior or direct lateral, is best in terms of improving patient outcomes. 3
The posterior approach is thought to have fewer complications related to gait because the abductor muscles are not dissected, but prior studies have associated the posterior approach with sciatic nerve injuries and an increased dislocation rates potentially due to capsule disruption, when compared to the direct lateral approach.3,4,8-10 The posterior approach has also been associated with lower levels of postoperative pain at 2 year follow-up, improved patient satisfaction, and improved quality of life when compared to the direct lateral approach.2,10 This was further described by Amlie et al, who observed that the direct lateral approach was associated with worsened quality of life, increased postoperative pain, and more subjective limping when compared to the posterior approach among patients treated with a total hip arthroplasty (THA). 11 However, orthopedic surgeons have reported that the posterior approach is a more difficult procedure to perform than the direct lateral approach. 5
A multitude of studies have sought to describe differences in complications and outcomes among the different surgical approaches.2-5,8,10-13 However, some studies focus on THAs, rather than HAs; some include all adults instead of geriatric patients who often have more comorbidities and may benefit from differing surgical approaches than their younger cohorts; some studies do not directly compare the direct lateral approach to the posterior approach and instead include less common approaches; research primarily focuses on dislocation and revision rates, rather than other in-hospital metrics, and lastly, some focus on elective surgery (ie, osteoarthritis cases) rather than traumatic hip fracture surgery.3,6-8,10,11,14-21 In fact, Chaudhry et al discuss the need for standardization in hip fracture repair to optimize outcomes, rather than studies focusing on hip replacements due to osteoarthritis. 1 Thus, there is a growing need to better delineate advantages among the surgical approaches to HA for geriatric patients suffering traumatic displaced femoral neck fractures. This study sought to add to the available literature directly comparing the two most common approaches, the posterior and direct lateral approach, and describe their effects on in-hospital metrics including: hospital length of stay (HLOS), blood loss volume, time to surgery, and discharge disposition specifically among a population of geriatric trauma patients with displaced femoral neck fractures admitted to a level 1 trauma center.
Materials and Methods
This retrospective cohort study at a level 1 trauma center included geriatric trauma patients (aged ≥60 years old) who suffered a displaced femoral neck fracture (July 1st, 2016, to March 31st, 2020) and who were managed with HA. Non-traumatic (ie elective) cases were excluded. Approval from the participating center’s Ethics Committee and Institutional Review Board was received prior to initiating the study. This study was approved with a waiver of patient consent. No funding was obtained. The patients were identified from the trauma registry at the participating center using International Classification of Diseases 10 codes for displaced femoral neck fractures. The data were collected from the trauma registry and the patient’s electronic health record. Any data missing from the trauma registry was collected from the patient’s electronic health record. The STROBE guidelines were followed when preparing this manuscript.
The primary aim of this study was to compare outcomes by surgical approach, posterior vs Harding direct lateral. There was no formal protocol directing the selection of the surgical approach. The surgical approach was at the discretion of the treating physician. At this institution, two orthopedic trauma surgeons exclusively used the direct lateral approach because of its reduced postoperative restrictions; the remaining four surgeons use both approaches and stated they do not use any specific patient characteristics used to guide treatment. At this institution the hip fracture is accessed posteriorly via elevation of the gluteus minimus and a posterior capsulotomy, taking down the short external rotators and piriformis. The posterior capsule is repaired at the conclusion of the procedure. When using the lateral approach, the hip fracture is accessed anteriorly via reflection of the anterior 1/3 of the gluteus medius insertion allowing access to the anterior capsule. The released portion of the medius insertion is repaired at the conclusion of the procedure. Anesthesia methods were not specific to the treatment approach, and data on anesthesia were not collected.
Patient Characteristics Compared by Surgical Approach.
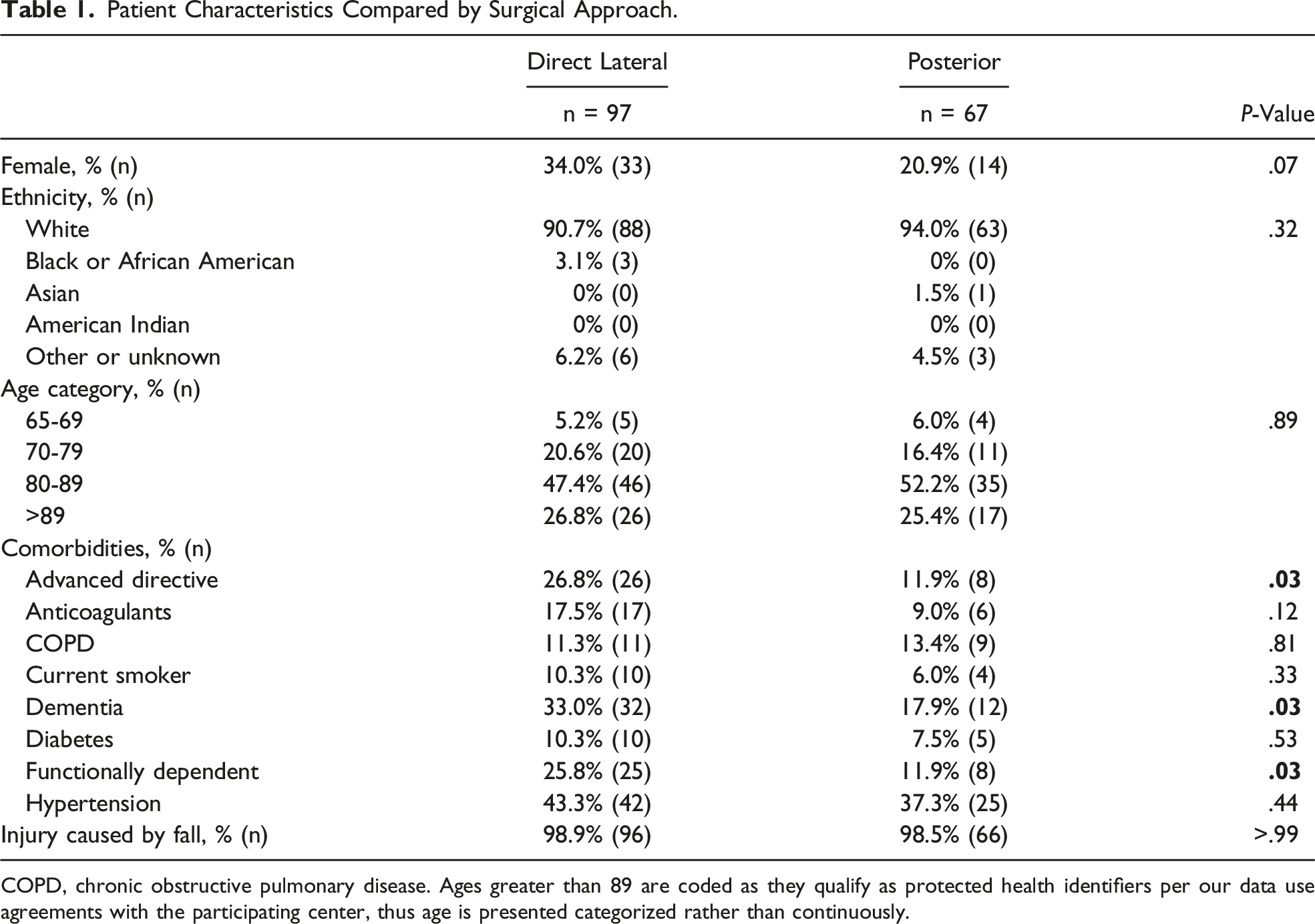
COPD, chronic obstructive pulmonary disease. Ages greater than 89 are coded as they qualify as protected health identifiers per our data use agreements with the participating center, thus age is presented categorized rather than continuously.
Results
Of the 164 patients who met the selection criteria, 59% (97) of patients were treated with the direct lateral approach and 41% (67) were treated with the posterior approach, Table 1. There was a trend (P = .07) towards higher proportion of females than males treated with the direct lateral approach than the posterior approach. The ethnicity (P = .32) and age (P = .89) were similar when compared by surgical approach. Those treated with the direct lateral approach had an advanced directive (P = .03), dementia (P = .03), or were functionally dependent (P = .03), more often than those treated with the posterior approach. The other comorbidities were similar between groups. Almost all patients’ injuries occurred after a fall, and there was no difference in the cause of injury, P > .99.
Outcomes Compared by Surgical Approach.

ICU, intensive care unit; LOS, length of stay; HLOS, hospital length of stay; DVT, deep vein thrombosis; CVA, cerebrovascular accident; PE, pulmonary embolism.
aCalculated for patients who went to the ICU.
bOnly includes survivors.
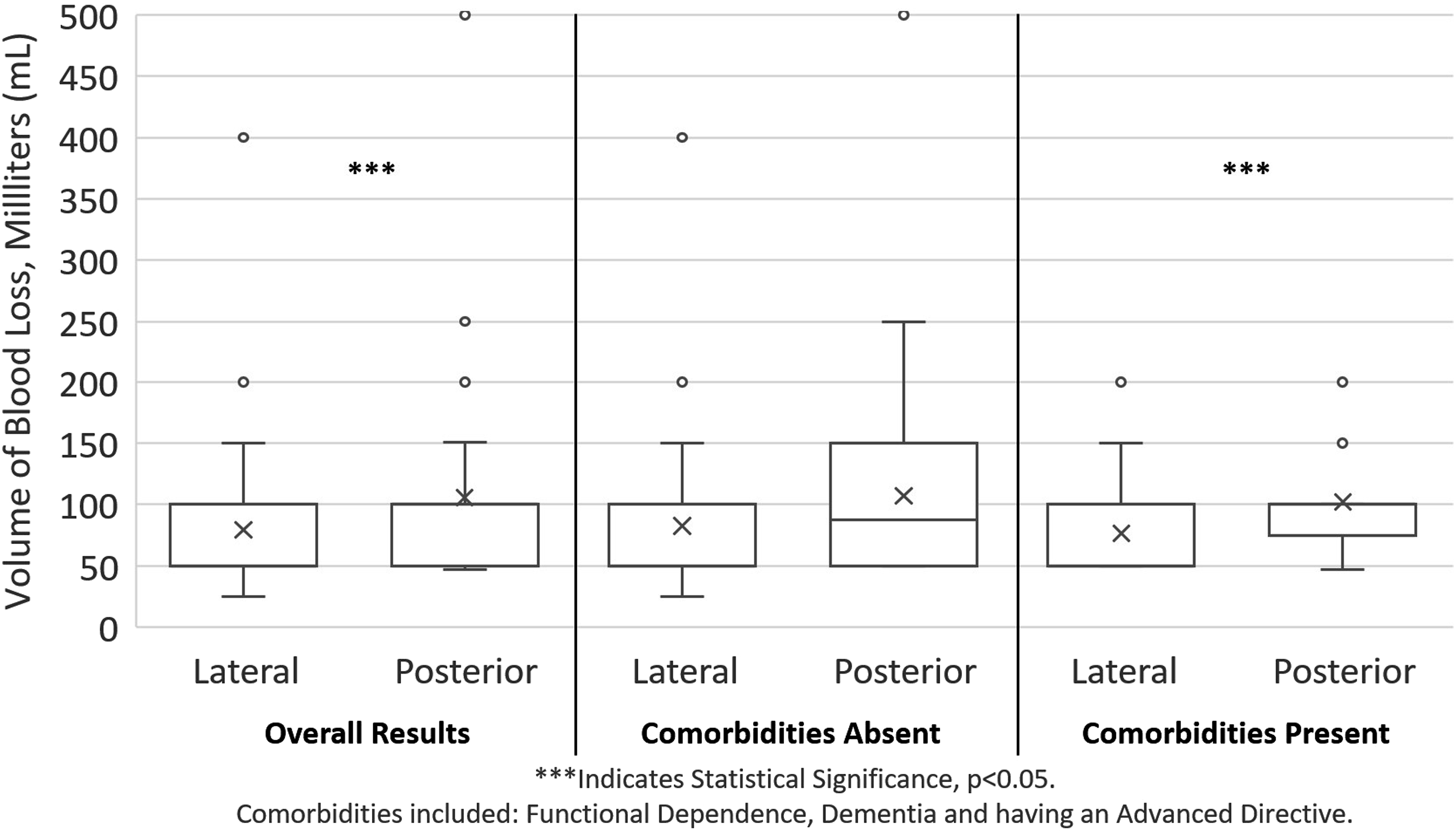
The blood loss volume is compared by the treatment approach, overall, and stratified by the presence and absence of the following comorbidities: functional dependence, dementia, and having an advanced directive. These comorbidities were significantly different when comparing patients by the treatment approach overall. The “X” in each box and whisker plot describes the mean. *** indicates statistically significant differences between groups.
Stratified Analysis
Outcomes Compared by Surgical Approach, Stratified by Presence of Comorbidities.
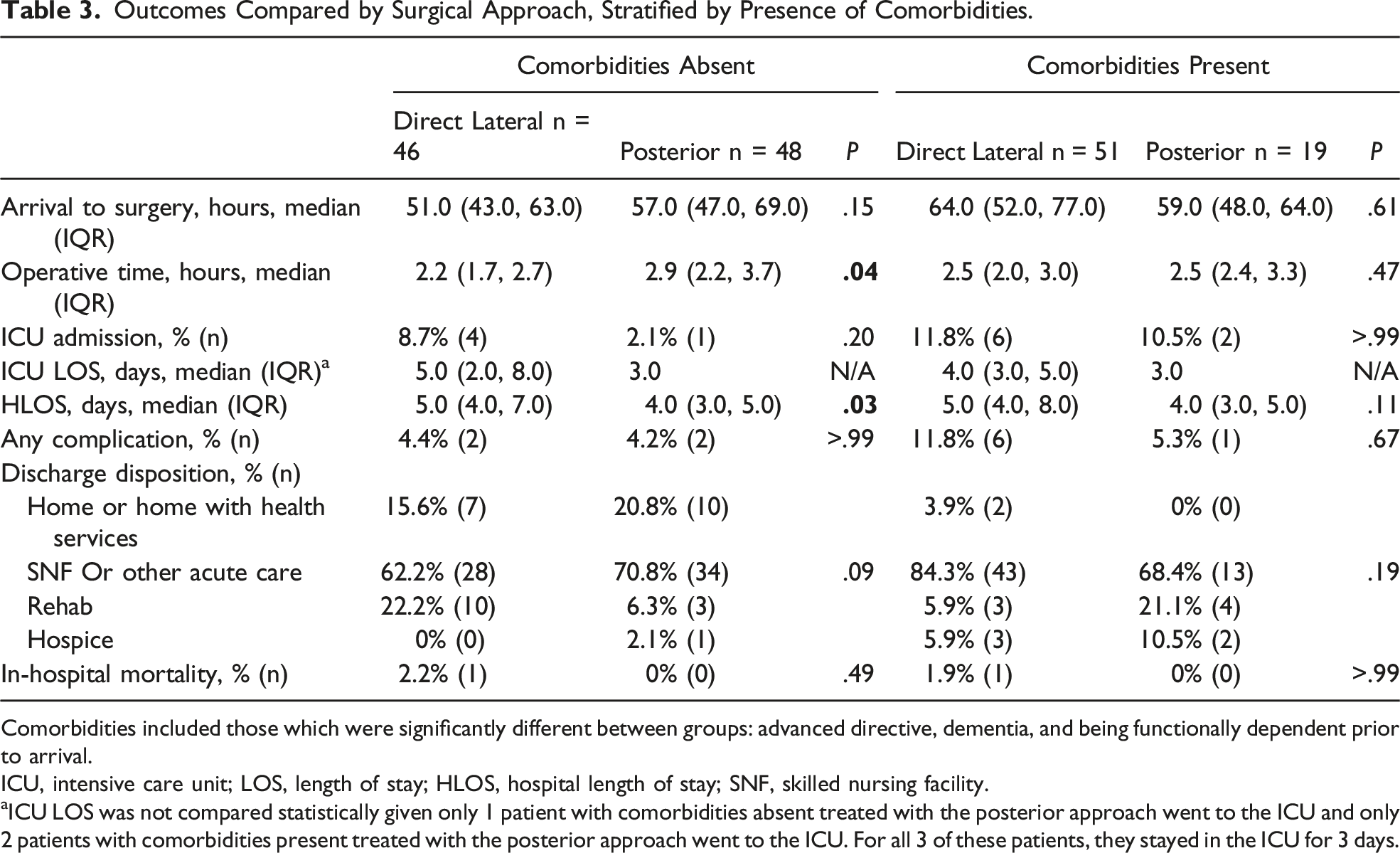
Comorbidities included those which were significantly different between groups: advanced directive, dementia, and being functionally dependent prior to arrival.
ICU, intensive care unit; LOS, length of stay; HLOS, hospital length of stay; SNF, skilled nursing facility.
aICU LOS was not compared statistically given only 1 patient with comorbidities absent treated with the posterior approach went to the ICU and only 2 patients with comorbidities present treated with the posterior approach went to the ICU. For all 3 of these patients, they stayed in the ICU for 3 days.
Discussion
There remains an unclear consensus on whether the posterior or the direct lateral approach to HA among geriatric trauma patients with displaced femoral neck fractures results in improved outcomes. In this study, patients treated with the direct lateral approach had a shorter operative time and a lower volume of blood loss, but a longer average HLOS with no difference in the time from arrival to surgery when compared to those treated with the posterior approach. There were also no differences in the complication rates, discharge disposition, or rate of in-hospital mortality between groups overall. However, it was observed that patients treated with the direct lateral approach had an advanced directive, dementia, or were functionally dependent more often than patients treated with the posterior approach; suggesting that despite the absence of a formal protocol for selection of patients for each treatment approach, surgeons may be selecting those with less comorbidities for the posterior approach. When a stratified analysis was performed, it was observed that patients with these comorbidities present (advanced directive, dementia, or functional dependence) who were treated with the direct lateral approach experienced a lower median volume of blood loss when compared to the patients treated with the posterior approach but had no other differences in any other outcome. Whereas, among patients with these comorbidities absent, there was no difference in blood loss when compared by the surgical approach, but compared to those treated with the posterior approach, patients treated with the direct lateral approach experienced a shorter operative time and a longer HLOS. This indicates that baseline patient comorbidities played a significant role in outcomes based on treatment approach. This study adds to the available literature comparing the posterior approach to the direct lateral approach, providing evidence that patient comorbidities may assist with decisions on the surgical approach when considering the outcomes of blood loss and HLOS. For example, for patients who are at an increased risk for bleeding, or those who have a comorbidity present, the direct lateral approach may lead to less blood loss. Whereas for healthier patients without comorbidities, the posterior approach may lead to shorter HLOS. Because of the lack of significant differences in major morbidity or mortality when comparing the direct lateral to the posterior approach, the decision to choose one approach over another could remain surgeon preference.
Although the median total blood loss was minimal for patients treated with both approaches, it was slightly higher (50 mL) for those treated with the posterior approach when compared to the direct lateral approach. However, this difference in volume of blood loss was not clinically significant. Lazaru et al reported that the direct lateral approach was associated with an increase of 51 mL of blood loss when compared to the conventional methods, including the posterior approach, however their study included THAs, not HAs. 14 Another meta-analysis of surgical approach for THA not HA, observed no difference in blood loss.17,22 Parker et al conducted a prospective randomized study and found no difference in the rate or volume of blood product transfusion between the two approaches. 5 One factor the investigators in this study thought might contribute to blood loss, was the use of pre-hospital anticoagulants; however the rate of pre-hospital anticoagulants use was similar when compared by the direct lateral and posterior approaches, which may be related to the lack of clinically significant differences in blood loss. Interestingly, in the stratified analysis, increased blood loss was noted for patients treated with the posterior approach when compared to the direct lateral approach, only among those with comorbidities present. For those with comorbidities absent, the median volume of blood loss reported was similar between those treated with the posterior approach and those treated with the direct lateral approach. These comorbidities could affect frailty, which has been shown to be a predictor of blood loss. 23 The findings in this study pertaining to blood loss, although statistically significant, may be clinically insignificant. To our knowledge, there have been no prior studies which have directly investigated blood loss between HA approaches when stratified by the presence of patient comorbidities. There was no difference in blood loss among the healthier patients, without comorbidities present, which may suggest that the comorbidities might have contributed to the blood loss. Another explanation not investigated in this study was the level of experience of the surgical team with each approach; van der Sijp et al conducted a meta-analysis and found that reported blood loss was correlated with the experience level of the surgical team and the technical difficulty of the procedure. 24
Because of the perceived difficulty of the posterior approach, surgeons may be selecting patients who are deemed healthier for the posterior approach, having less comorbidities, and this may explain why patients treated with the direct lateral approach had comorbidities (dementia, advanced directives, or functional dependence) more often than those treated with the posterior approach. 5 The surgical approach in this study was partially a result of the surgeons preference, as at this institution, two trauma orthopedic surgeons exclusively use the direct lateral approach because of its perceived reduced postoperative restrictions, but the remaining six trauma orthopedic surgeons chose the surgical approach at their discretion. The surgeons reported no criteria are used to guide treatment. Despite this, the posterior approach was used more frequently than the direct lateral approach for healthier patients with less comorbidities. This may have been an inadvertent decision by the surgeons. Therefore, surgical approach in this population, was a combination of surgeon preference and based on presence of comorbidities. Kristensen et al. also observed that patients treated with the posterior approach had higher rates of low American Society of Anesthesiologists (ASA) classifications, which is indicative of less comorbidities, than patients treated with the direct lateral approach. 2 Leonardson et al reported the posterior approach was associated with improved patient-reported outcomes when compared to the direct lateral approach, but after adjusting for factors including the ASA score there was no difference in outcomes. 12 Because of these baseline differences between groups and potential for the presence of comorbidities to introduce bias into the results, a stratified analysis based on presence and absence of comorbidities, was conducted.
The median operative time was 30 min longer for patients treated with the posterior approach when compared to the direct lateral approach. This is contrary to prior studies which have noted no significant differences in the average operative time between these approaches.5,8,22,24 Four other studies found the posterior approach was associated with shorter operative times than the direct lateral approach, however two of those were in a population of THA not HA, one study only observed a trend towards a statistical difference, and the differences were often short (∼10 min).2,14,22,24 It is possible that the difference in operative time noted in this study could be related to surgeon factors. As described by Parker et al orthopedic surgeons stated that the posterior approach was more technically difficult than the direct lateral approach. 5 This increased technical difficulty could potentially explain why the median operative time was longer for patients treated with the posterior approach in this study. Further van der Sijp et al. state that most surgeons are predominantly trained in a single approach and that could partially explain the variance in results related to operative time across studies. 24 When the stratified analysis was performed, this difference in the median operative time was only noted among patients with comorbidities absent. The patients with comorbidities present may be more medically complex, resulting in longer operation times for the direct lateral approach, making it more comparable to the operative time for the posterior approach for patients with comorbidities present. The operative time for the direct lateral approach for patients with comorbidities absent was a median of 2.2 h, whereas for patients with comorbidities present was 2.5 h. Therefore, it could be deduced that the direct lateral approach typically has a shorter operative time, but that it appears comparable to the posterior approach only when more medically complex patients with comorbidities present are included. Although the operative time was significantly shorter for those treated with the direct lateral approach when compared to those treated with the posterior approach for patients with comorbidities absent, the HLOS was significantly longer. However, the difference in operative time between groups was small, being less than 1 h. In this study operative time and HLOS were not significantly correlated (data not visualized, P = .26), meaning when operative time increased, there was not a corresponding increase in HLOS. Other factors such as the patient’s comorbidities, ICU admission, or complications may have been more important factors for the HLOS than the operative time in this subset of patients. While not significant, the ICU admission rate was higher for those treated with the direct lateral approach than the posterior approach, among those with comorbidities absent. Both having a complication and ICU admission were associated with a longer HLOS in this population (data not tabulated).
Similar to the results related to blood loss and operative time, HLOS also seemed to be dependent on the presence of comorbidities. Across all patients the posterior approach was associated with a shorter HLOS on average, but in the stratified analysis this was only true for patients with comorbidities absent. For patients with comorbidities present, there was no significant difference noted in the average HLOS. One meta-analysis including 21 studies examining approaches to HA, found only one study reported on the difference in HLOS between these surgical approaches, with no significant difference between groups. 24 Another study also reported no significant difference in HLOS, but that study was not restricted to only geriatric patients. 5 Given that prior research has observed an association between HLOS and cost, these findings may indicate that the direct lateral approach is associated with higher costs in this population, specifically for patients with comorbidities absent, but further data is needed to confirm this.24,25 Furthermore, prolonged HLOS is associated with increased risk of postoperative complication and infection, these are other factors to consider when selecting the surgical approach to HA for geriatric trauma patients. 26 The extended HLOS for patients treated with the direct lateral approach may be related to the higher count of complications observed for patients treated with the direct lateral approach overall; however this difference in complications was not significant between groups. Patients treated with the direct lateral approach had unplanned admissions to the ICU more than those treated with the posterior approach, but again the difference was not significant. This is consistent with prior literature which found no difference in in-hospital complications and mortality.3,5,8-10
Limitations
This was a retrospective study with a small sample size, which limited the ability to conduct adjusted analyses. It was observed that there were significant differences in the rate of comorbidities between groups; to address for this confounding variable a stratified analysis was conducted and the individual effects of each strata were discussed in detail. Information related to ambulation (postoperative, and long-term after discharge, timed up and go, time to ambulation), patient pain, the use of cement, revisions, and dislocation rate were not collected. Because of the traumatic mechanism of the injuries included in this study, patients who suffer dislocations or need revisions may not return to the initial admitting center who performed the surgery and may instead go to a different hospital. Because of this dislocation and revision rates would be lower at this center than the rates reported for hospitals conducting elective surgeries. Factors such as surgeon experience may also play a role in outcomes. Data on the reason why either approach (direct lateral or posterior) was used was not documented in the charts and could not be summarized. The blood loss volumes included estimates from the treating physician, which have previously been shown to be relatively inaccurate. Antithrombotic medications used in-hospital may play a role in the amount of blood loss during operation, but this data was not collected. This study may not be generalizable to other centers, a younger population, or to non-trauma elective patients. Future studies should focus more on postoperative gait information such as timed up and go, and time to ambulation. Data on the anesthesia medications and techniques used were not collected and therefore we were unable to analyze any differences in the anesthesia medications and techniques between groups.
Conclusions
While those treated with the direct lateral approach lost significantly less blood than those treated with the posterior approach, the difference was small and possibly clinically negligible. Those treated with the direct lateral approach had a significantly shorter operative time and they had a significantly longer HLOS than those treated with the posterior approach, but there were no significant differences noted for complications, discharge dispositions, or mortality between groups. Thus, neither the direct lateral approach nor the posterior approach was identified as superior in terms of in-hospital metrics and either approach remains a viable strategy when treating displaced femoral neck fractures in geriatric trauma patients. While surgery was at the discretion of the treating physician, there was evidence that the direct lateral approach was used more often for patients with comorbidities than the posterior approach. This study found that presence or absence of comorbidities also played a significant role in outcomes. Those who were functionally dependent, had an advanced directive, or had dementia, experienced a higher volume of blood loss when treated with the posterior approach than the direct lateral approach. Whereas those who did not have an advanced directive, dementia and were not functionally dependent had a longer HLOS and shorter operative time when treated with the direct lateral approach than the posterior approach, with no other differences noted in other outcomes. While this study provides further evidence that the surgical approach could remain a matter of physician preference, presence or absence of these comorbidities may assist with selection of surgical approach in terms of preventing blood loss and reducing HLOS. For those without these comorbidities, the posterior approach may lead to a shorter HLOS than the direct lateral approach, whereas for those with these comorbidities present, the direct lateral approach may lead to less blood loss than the posterior approach.
Footnotes
Acknowledgements
We would like to thank our Clinical Research Coordinator, Breanna Nickels, our Project Manager, Diane Redmond, and our Institutional Review Board Coordinator, Tina Thompson. This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Author Contributions
SM, SJ, AC, KS, CR and DBO contributed to the study of the study. AC contributed to the data acquisition. SJ conducted the analysis and interpretation of the data. SJ, KS and SG drafted the initial manuscript. SM, AC, CR, and DBO provided substantial revisions to the manuscript. All authors approved of the final version of the manuscript for submission and take public responsibility for appropriate portions of the content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
Due to the data use agreements with the participating hospital we are unable to provide the data used in this study.