
Abstract
Introduction
Controversary exists around the best surgical management for traumatic geriatric displaced femoral neck fractures. The study objective was to compare outcomes among those managed with a total hip arthroplasty (THA) to those managed with a hemiarthroplasty (HA).
Methods
This retrospective matched cohort study included geriatric hip fractures (≥65 y/o) admitted 7/1/16-3/31/20. Patients were matched on having an advanced directive, pre-existing dementia, and age. Outcomes included: time to surgery, length of stay (LOS), blood loss volume, and discharge destination. THAs were compared to HAs; an alpha of <.05 indicated statistical significance.
Results
There were 191 patients: 86% were treated with HA and 14% with THA. Most (40%) were 80-89 years old, 66% were female, and 92% were white. After matching, the groups were well balanced on demographics and baseline characteristics with 27 patients/arm. The median time to surgery was 23 hours for both arms, P = .38. The LOS was significantly longer for those managed with a HA when compared to those managed with a THA, 5.6 vs 4.0 days, P = .001. The median blood loss volume was significantly lower for HAs than for THAs, but the difference was small, 100 vs 120 mL, P = .02. Patients managed with a HA were less likely to be discharged home than those managed with a THA, 22% vs 70%, P = .005.
Conclusions
While patients managed with a THA had significantly more blood loss than those managed with a HA, the difference in blood loss was small and not clinically relevant. Those managed with a THA experienced a significantly shorter LOS and were more likely to be discharged home than patients managed with a HA. Among a healthier, younger geriatric population, THA may lead to shortened LOS and improved discharge destinations when compared to HA for treatment of femoral neck fractures.
Introduction
As many as 30% of geriatric patients die within a year of sustaining a hip fracture; among those who survive, approximately half do not achieve their pre-injury ambulation.1,2 Earlier surgical intervention is significantly associated with decreased mortality and the goal of surgery is to achieve or improve the pre-injury ambulation, and to mobilize early after surgery.1,3 It is estimated that the number of annual hip fractures in the United States will increase in the next 30 years, from 300,000 to 700,000.4,5 Hence the need for improved guidelines on the management of geriatric hip fractures to optimize outcomes. 3
While nondisplaced femoral neck fractures (FNFs) are regularly managed with osteosynthesis, controversy remains regarding the management of displaced FNFs.6-8 Hemiarthroplasty (HA) was the initial surgical procedure of choice for displaced FNFs, however total hip arthroplasty (THA) has emerged as an alternative method over the past 20 years. 7 HA has been associated with shorter operative time and less postoperative complications, but with poorer postoperative functional results, higher revision rates, and increased postoperative pain.3,4,9 Because of this, HA is typically reserved for sicker and more medically complex patients.3,8 In contrast, THA had been associated with longer operative times, increased surgical complexity, higher costs, and higher rate of post operative dislocation, but better postoperative function and pain control.4,7,9-11 As a result, it is preferred for younger and healthier patients who have a better functional condition pre-injury.3,4,10 While these factors are reported in the literature, the effect of surgical management on other in-hospital outcomes is unclear.
As the number of geriatric patients is expected to dramatically increase over the next 20 years, so are the projected number of hip fractures, thus there is a need for more definitive guidelines for the surgical management of geriatric hip fractures.1,3 Many studies have compared the effect of HA and THA on postoperative morbidity and mortality but, few studies have investigated their effect on blood loss volume, postoperative complications, LOS, and discharge destination.3,4,6-10,12 These factors can have major implications in patient morbidity and mortality, which need to be considered when selecting the appropriate surgical procedure for individual geriatric patients. The purpose of this study is to compare the outcomes of time to surgery, LOS, blood loss volume, postoperative complications, and discharge destination among those treated with THA to those managed with a HA among geriatric hip fractures.
Methods
This was a retrospective cohort study at a level 1 trauma center. Geriatric trauma patients (aged ≥65 years old) who suffered a hip fracture admitted July 1st, 2016, to March 31st, 2020, were included. Patients were excluded if they were not managed with a THA or a HA. Ethics Committee and Institutional Review Board (IRB) approval were received from HealthONE, LLC (study number 1615858). This study was approved with a waiver of patient consent. The primary aim of the study was to compare outcomes between those managed with a THA and those managed with a HA. The decision to offer THA to a patient is at the discretion of the surgeon. In general patients who are community ambulators without significant medical comorbidities are offered THA regardless of age. Outcomes included time in surgery (hours), LOS (days), blood loss volume (mL), in-hospital complications, and discharge destination. Any blood loss reported perioperatively in the patients’ electronic medical record was included. This often includes estimates from the treating physician, or blood soaked in sponges measured and documented.
Matching
Demographics and Baseline Characteristics.

Abbreviations: AIS, Abbreviated Injury Scale; SBP, systolic blood pressure; COPD, chronic obstructive pulmonary disease; IQR, interquartile range. Bold values indicate statistically significant differences between groups.
Statistical Analysis
Dichotomous and categorical variables were summarized as percentage (count) and were compared using McNemar’s test. Continuous variables were summarized as means (standard deviation) or medians (interquartile range) and were compared using paired Student’s t test or Wilcoxon paired-rank sum, when appropriate. An alpha of less than .05 was used to define statistically significant differences between groups. Analyses were performed using Statistical Analysis Software (SAS) v. 9.4.
Results
Of the 191 patients who met the selection criteria, a majority (85%) were managed with a HA. The groups were similar in their sex (P = .62), and race (P = .65), however those managed with a HA were significantly older (P < .0001) than THA patients, Table 1. While the admission heart rate was similar (P = .20), the admission systolic blood pressure was trending towards (P = .06) statistically higher for those managed with a HA when compared to those managed with a THA. Patients managed with a HA also had a preexisting advanced directive (P = .01) and dementia (P = .001) more often than patients managed with a THA; other comorbidities were similar between groups. There was no difference in the cause of injury (P = .27) between groups. Additionally, the time from arrival to surgery (P = .42) and injury to surgery (P = .76) were similar between groups. There was no difference in the surgical approach between groups; 40.9% of those treated with a HA received the posterior approach compared to 29.6% of those treated with a THA, P = .27.
Matched Population
Matched Patients Demographics and Baseline Characteristics.
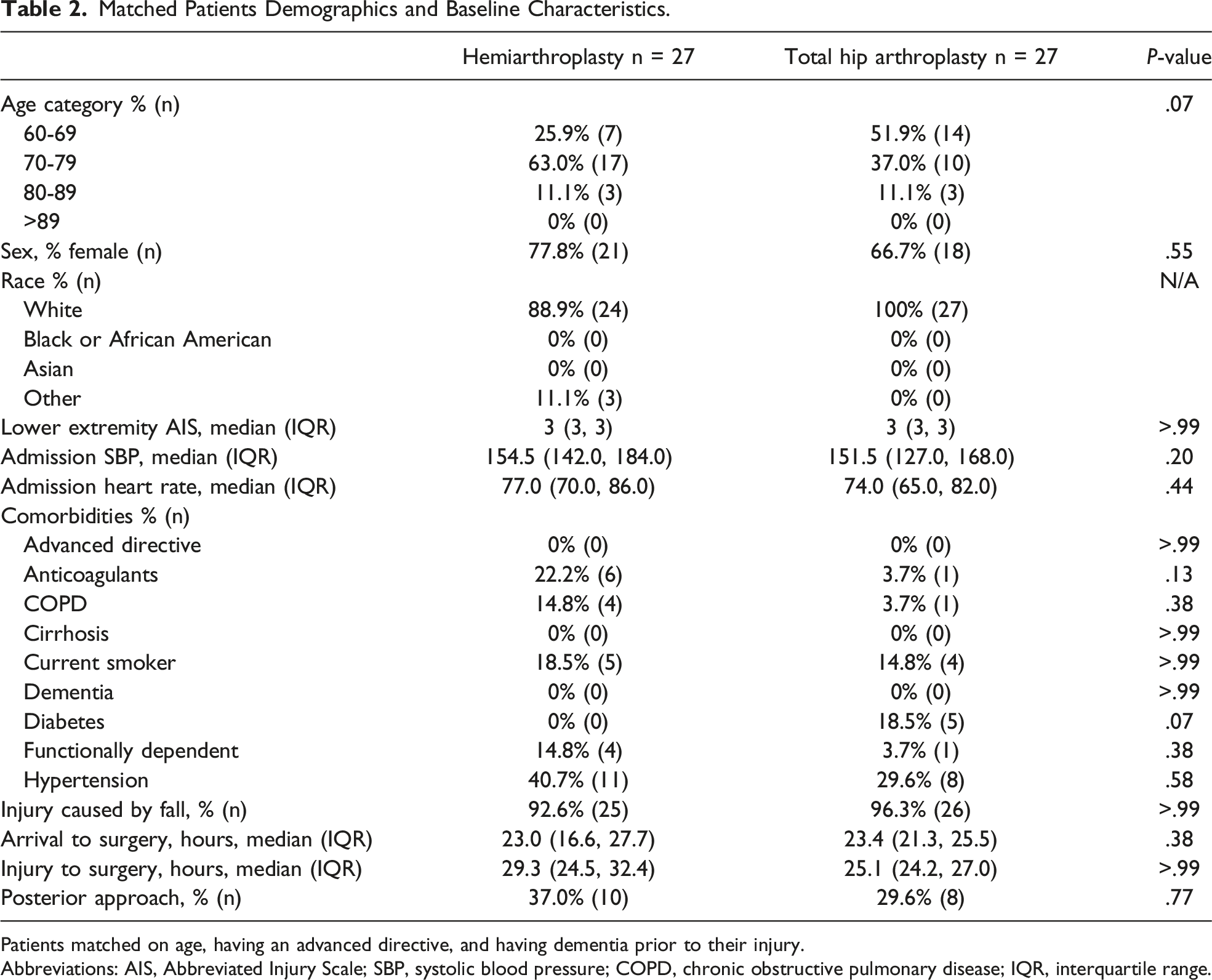
Patients matched on age, having an advanced directive, and having dementia prior to their injury.
Abbreviations: AIS, Abbreviated Injury Scale; SBP, systolic blood pressure; COPD, chronic obstructive pulmonary disease; IQR, interquartile range.
Outcomes for Matched Population.

Abbreviations: ICU, intensive care unit; HLOS, hospital length of stay; DVT, deep vein thrombosis; CVA, cerebrovascular accident; PE, pulmonary embolism; SNF, skilled nursing facility; IQR, interquartile range. Bold values indicate statistically significant differences between groups.
The time from arrival to surgery was approximately 23 hours for both groups (P = .38), Figure 1. The time in surgery was also statistically similar between groups, being a median of 1 hour for those managed with a HA and 1.3 hours for those managed with a THA, P = .50. Those managed with a HA had a significantly longer median LOS when compared to those managed with a THA (5.6 vs 4.0 days, P = .001). There was also no difference in the surgical approach after matching, 37.0% of those treated with a HA compared to 29.6% of those treated with a THA received the posterior approach, P = .77. Timing metrics by surgical approach.
In-hospital complications were rare, but the rate of complications was similar between groups (P = .25) Table 3. Of the complications, all were among patients managed with a HA: 7.4% suffered a deep vein thrombosis, 7.4% suffered a stroke or cerebrovascular accident, 7.4% suffered a pulmonary embolism and 3.7% had an unplanned admission to the intensive care unit (ICU). While those managed with a HA had a significantly lower median volume of blood loss than those managed with a THA, the difference was small (100 mL vs 120 mL, P = .02). Patients managed with a HA were less likely to be discharged to home or home with health services, and more likely to be discharged to a skilled nursing facility, other acute care, or to rehabilitation, than those managed with a THA (P = .01)
Discussion
Both HA and THA have been shown to be viable options for the treatment of displaced FNFs for geriatric trauma patients. In this study the patients managed with a THA were significantly younger and had dementia or a preexisting do not resuscitate (DNR) order less often than HA patients. After matching for these characteristics, management with a THA was associated with greater blood loss, though the difference was clinically insignificant, as well as a significantly shorter LOS and a greater likelihood for the patient to discharge home rather than to a rehabilitation facility when compared to HA. This data suggests that younger age, dementia, and preexisting DNR may be useful factors to consider for THA selection. Notably, there were no significant differences in the mortality rate, complication rate, time to surgery, or time in surgery when comparing patients managed with THA to those managed with HA.
While the literature suggests that THA may be preferable for younger and less medically complex patients, and that HA is better suited for older and sicker patients, there has been little consensus regarding the specific factors that should be used to guide treatment.3,4,12 Like prior studies, this study found older age was associated with HA management.3,4,7,9,12 Additionally presence of dementia or a preexisting DNR were factors related to treatment with HA. Another study found that congestive heart failure, chronic lung disease, diabetes, hypertension, renal failure, and older age to be related to treatment with HA. 4 It has also been suggested to consider the preinjury level of activity when determining the best treatment approach. 4 Dangelmajer et al observed that THA operation was associated with age, race, payer status, hospital size, and being a teaching hospital, they discuss that the high cost of THA may be another factor driving the decision process.7,11 Another study observed younger age and use of steroids to be predictive of THA. 9 Boniello et al. suggest that HA is utilized for sicker, older patients more often due to the complexity of THA and longer operative times, however in this study the median time in surgery was comparable between groups. 4
The lack of statistical difference for the median time in surgery between the groups is in contrast to existing literature; prior studies have noted an increased time in surgery for patients managed with a THA when compared to a HA.8,11,12 This difference may be related to surgeon experience or hospital protocols, as this study evaluated a single-institution, as opposed to studying multiple centers which may have varying levels of surgeon experience or treatment protocols. Time to surgery was also not statistically different between patients who underwent HA and THA, with a mean time of 23 hours observed for both groups. Consistent with this study, a prior study saw no significant differences in time to surgery. 12
The LOS was significantly longer among patients who underwent HA as compared to THA (5.6 vs 4.0 days), which may be related to improved postoperative functionality among THA patients priming them for discharge quicker than HA patients. Other studies also observed a longer LOS for patients managed with a HA compared to THA; however, the difference in both studies was small (<1 day) which raises the question of clinical significance.4,13 Sharma et al observed no difference in the LOS between groups.12,13 Alternatively, Ogawa et al reported the patients treated with HA experienced a significantly shorter LOS than THA patients, P < .001. 11 In a study by van den Bekerom et al, THA patients stayed a mean of 18.8 days, and HA patients a mean of 17.1 days, but they did not provide the significance of this difference. 14
While the complication rate was similar between groups, complications were rare and only occurred in patients managed with a HA. The complications were: thromboembolic events, stroke, and unplanned admission to the ICU. Other studies also observed no differences in complications.11,14,15 Ogawa et al noted that the rate of systemic complications was similar between groups, P = .65. 11 However when examining individual complications, they observed a statistically higher rate of urinary tract infections among patients managed with a HA. 11 While complication rates were similar, there was a significant difference in the blood loss volume.
The volume of blood loss was significantly lower for patients managed with HA compared to THA, although the difference was small (100 mL vs 120 mL) and may be clinically negligible. Similar to our study, Ogawa, et al reported higher volumes of blood transfusions in patients undergoing THA, which they attributed to a longer operative time and surgical complexity for THAs. 11 van den Bekerom et al. noted higher blood loss among patients managed with THA, which also appeared to correlate with longer operative time. 14 This was further noted by Sharma et al, Blomfeldt et al, and in a systemic review by Li et al8,12,16 There was no difference in operative time between THA and HA in this study, which may be why the difference in volume of blood loss was so minute.
Patients treated with HA were less likely to be discharged to home and more likely to be discharged to a skilled nursing facility or other rehabilitation facility when compared to THA patients. This suggests that those treated with a THA needed further care after they were approved for hospital discharge than patients who were treated with a HA. Stonach et al reported the same finding of improved rates for patients managed with a THA to be discharged home. 13 This finding is in line with other studies that found THA was associated with improved functional outcomes compared to HA.3,4 If patients are more functional and ambulate faster postoperatively, they would be more likely to be discharged home when compared to those patients who have more functional limitations postoperatively and therefore are in greater need of physical rehabilitative support before and after leaving the hospital. Alternatively, Blomfeldt et al. reported no difference in living conditions between groups at 4 months or at 12 months after discharge. 8
Limitations
This study had limitations; this was a retrospective study with a small sample size. Information on the post-operative gait was not collected, nor was the dislocation rate. The dislocation rate can be difficult to determine for trauma cases who might not receive further treatment at the same center where they were sent after their traumatic injury. Blood loss volumes included estimates documented by the operative surgeon, which may vary by the operative surgeon. The results may not be generalizable to elective cases or to populations younger than 65 years old. In future studies, it may be of interest to evaluate the time to postoperative ambulation between THA and HA. Additionally, this study did not look at the effects of operative cementing. Surgeon preference may also influence the decision to conduct a HA or a THA, a survey found 73% of general orthopedic surgeons preferred HA. 10
Conclusions
This study found that while patients managed with THA experienced significantly more blood loss, the difference was not clinically relevant. The patients managed with THA also had a shortened LOS and were more likely to discharge home rather than a rehabilitation facility, with equivalent time to surgery and postoperative complications compared to patients managed with HA. Among a healthier, younger geriatric population, THA may lead to shortened LOS and improved discharge destinations when compared to HA for treatment of hip fractures. Patient age, presence of dementia, or a preexisting DNR may be important factors for operative management of geriatric hip patients.
Patient Consent
This study was approved with a waiver of consent.
Footnotes
Acknowledgements
We would like to thank our Clinical Research Coordinator, Breanna Nickels, our Project Manager, Diane Redmond, and our Institutional Review Board Coordinator, Tina Thompson.
Author Contributions
SM, SJ, AC, KS, CR and DBO contributed to the study of the study. AC contributed to the data acquisition. SJ conducted the analysis and interpretation of the data. KS and SJ drafted the initial manuscript. SM, AC, CR, and DBO provided substantial revisions to the manuscript. All authors approved of the final version of the manuscript for submission and take public responsibility for appropriate portions of the content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity.
Disclaimer
The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Ethical Statement
Data Availability Statement
Due to the data use agreements with the participating hospital we are unable to provide the data used in this study.