
Abstract
Introduction:
Hemiarthroplasty is increasingly used for the treatment of geriatric femoral neck fractures in an effort to optimize value-based care. The current American Association of Orthopaedic Surgeons (AAOS) guidelines released in 2014 for the treatment of geriatric hip fractures recommend the utilization of monopolar cemented constructs. The purpose of this study was to evaluate hip hemiarthroplasty implant cost variability and implant selection trends from 2006 to 2018.
Materials and Methods:
A retrospective review of 940 geriatric hip fractures treated with hemiarthroplasty was conducted across 3 institutions from 2006 to 2018. Variables examined were construct type, surgeon, operative time, patient mortality, and implant cost. Statistical analysis consisted of multigroup comparative tests and multiple linear regression analyses to evaluate correlative measures.
Results:
The study population was 85.0 ± 7.9 years of age with a body mass index of 24.0 ± 5.5. A total of 33 (3.5%) patients were deceased at the 90-day postoperative mark and 45 (4.8%) patients at the 1-year mark. There was no statistical difference in terms of mortality between the 4 implant cohorts at the 90-day mark (P = .56) and 1-year mark (P = .24). The bipolar press-fit construct was the most expensive, US$3900.61 ± US$2607.54, and the monopolar cemented construct was the least expensive, US$2618.68 ± US$1834.16. The mean operative time was 6 minutes greater for press-fit implants, 93.6 ± 32.0, than cemented implants, 87.1 ± 33.6 (P = .02). The use of monopolar cemented implants increased from 12.1% to 83.3%, while bipolar press-fit decreased from 57.6% to 4.6% from 2013 to 2018.
Discussion:
The use of a bipolar and/or press-fit implant significantly increases construct cost despite little evidence in the literature of improved outcomes. Contrary to previous research, cemented implants do not increase the operative time.
Conclusions:
Encouragingly, selection of the most cost-conscience implant, monopolar cemented, has been increasing since 2014, which may reflect the influence of current AAOS guidelines.
Level of Evidence:
Diagnostic Level III.
Introduction
Geriatric femoral neck fractures are common and associated with significant medical costs. There were more than 65,000 geriatric femoral neck fractures in the United States in 2013. 1 This number is projected to significantly rise as the population over 65 is estimated to increase from 49.2 million in 2016 to 80.8 million in 2040. 2 The American Academy of Orthopaedic Surgeons (AAOS) guidelines contain a strong recommendation for the use of arthroplasty for displaced femoral neck fractures. 1,3 Currently, 63.6% of operatively treated femoral neck fractures in geriatric patients are treated with hip hemiarthroplasty. 1
Historically, matters of pricing in the US health care system were not of great concern to surgeons. However, current and projected health care costs have increased to unsustainable levels. By 2025, national health expenditures in the United States are projected to balloon to 19.9% of gross domestic product. 4 The exorbitant cost of health care provides impetus to orthopedic surgeons to understand their role in managing scarce resources by considering cost when selecting orthopedic implants. 5
It is widely accepted that bipolar implants are more expensive than monopolar implants with minimal impact on functional outcomes in the elderly (Figure 1). 6 -10 A systematic review of 10 randomized control trials found that bipolar and monopolar implants are associated with similar outcomes in hip function, hip pain, and quality of life with no significant difference in operative time, mortality, reoperation, and complications. 6 Although bipolar implants significantly decreased the incidence of acetabular erosion at 1-year follow-up, there was no significant difference in acetabular erosion between monopolar and bipolar constructs at any other follow-up point from 4 months to 4 years. 6
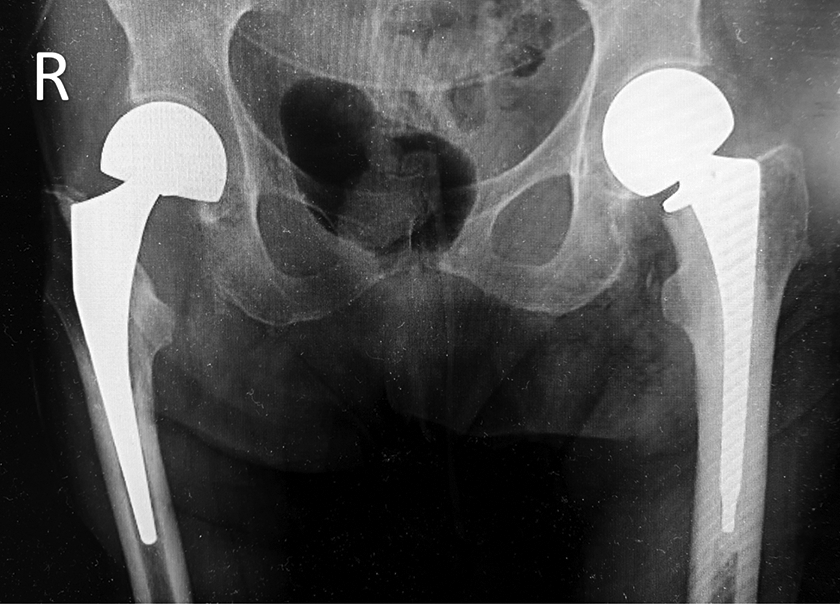
Anteroposterior pelvic radiograph displaying a monopolar cemented hemiarthroplasty construct (L) and a bipolar press-fit construct (R).
Less is known about the economic impact of selecting cemented versus press-fit (non-cemented) implants in the US market. 11,12 Studies have demonstrated that the additional operative time and accessories used to achieve the cement technique result in a higher cost than when utilizing a press-fit construct. 13 Because there is little evidence to suggest superior clinical outcomes through contemporary implants and fixation methods, the choice of the device can result in cost savings without impacting the quality of care.
American Academy of Orthopaedic Surgeons guidelines recommend a monopolar cemented implant for the treatment of geriatric hip fractures. 3,14 A meta-analysis of 7 studies reported that cemented implants were associated with better postoperative hip function at 12 months and lower intraoperative and postoperative fracture rates when compared to press-fit implants. There was no significant difference between the groups with regard to mortality, infection, complications, and reoperation rates. 15 However, the devices used in hip hemiarthroplasty procedures often considerably differ in cost. 12 There is limited data in the literature regarding the impact of hemiarthroplasty implant selection and fixation combinations on construct cost and trends in implant selection in the United States. The purpose of this study was to evaluate hip implant cost variability and trends in implant selection from 2006 to2018 in a large health care system. Our hypothesis was that monopolar cemented implants would be the least expensive and that implant guidelines would not correlate with implant selection trends. The primary objective was to determine variation in implant cost for bipolar cemented; bipolar press-fit; monopolar cemented; and monopolar press-fit implants. The secondary objective was to ascertain changes in implant selection over time.
Materials and Methods
Study Design
Following institutional review board approval, femoral neck fractures treated with hemiarthroplasty, between 2010 and 2018, were retrospectively identified using current procedural terminology (CPT) codes across a metropolitan health care system. Inclusion criteria were a displaced femoral neck fracture with a non-pathological origination, greater than or equal to 65 years of age, and treatment with a primary hemiarthroplasty implant. Patients were excluded on the basis of open fracture and polytrauma with concurrent surgical procedures. The electronic medical record (EMR) was queried for patient’s demographics, surgical details, injury characteristics, and hemiarthroplasty construct details. The health care system is a multi-vendor system and each hospital within the system has its own vendor contract.
Sample Population and Data Collection
A total of 1421 patients were identified utilizing CPT codes 27125 and 27236 for hip hemiarthroplasty and open treatment for femoral neck fractures with internal fixation or prosthetic replacement, respectively. A total of 940 (66.2%) patients treated by 26 surgeons were included in this investigation (Figure 2). Of the 26 operating surgeons, 17 were fellowship-trained in adult reconstruction, trauma, sports, pediatric, or hand and upper extremity. All fractures were initially radiographically reviewed for AO Foundation and Orthopaedic Trauma Association (AO/OTA) fracture classification of femoral neck fractures (AO/OTA-31B). Demographic characteristics included: gender, age, and body mass index (BMI) in kilograms per meter squared (kg/m2). Surgical characteristics included the operating surgeon, operative time, conversion to total hip arthroplasty (THA), American Society of Anesthesiologists (ASA) score, 16 mortality, and mortality date. Operative times were collected by circulating nurses at the start and end times of each procedure per system policy. Postoperatively, there was a heterogenous mix of comanagement and hospitalist management. The sum implant cost, including the cost of cement and cementing accessories, in US dollars was derived by obtaining the individual implant model numbers from the EMR and then cross-referencing them to the system’s charge master database, reflecting the direct manufacturer purchase price. Fixation constructs were radiographically reviewed and then stratified for polarity, monopolar versus bipolar, and use of a cemented implant. Identifying information for implant types and associated vendors was not listed in this investigation due to existing nondisclosure contracts between the vendors and their respective health care system clients. Mortality and date of death were determined from a query of the National Death Index (USA National Center for Health Statistics).
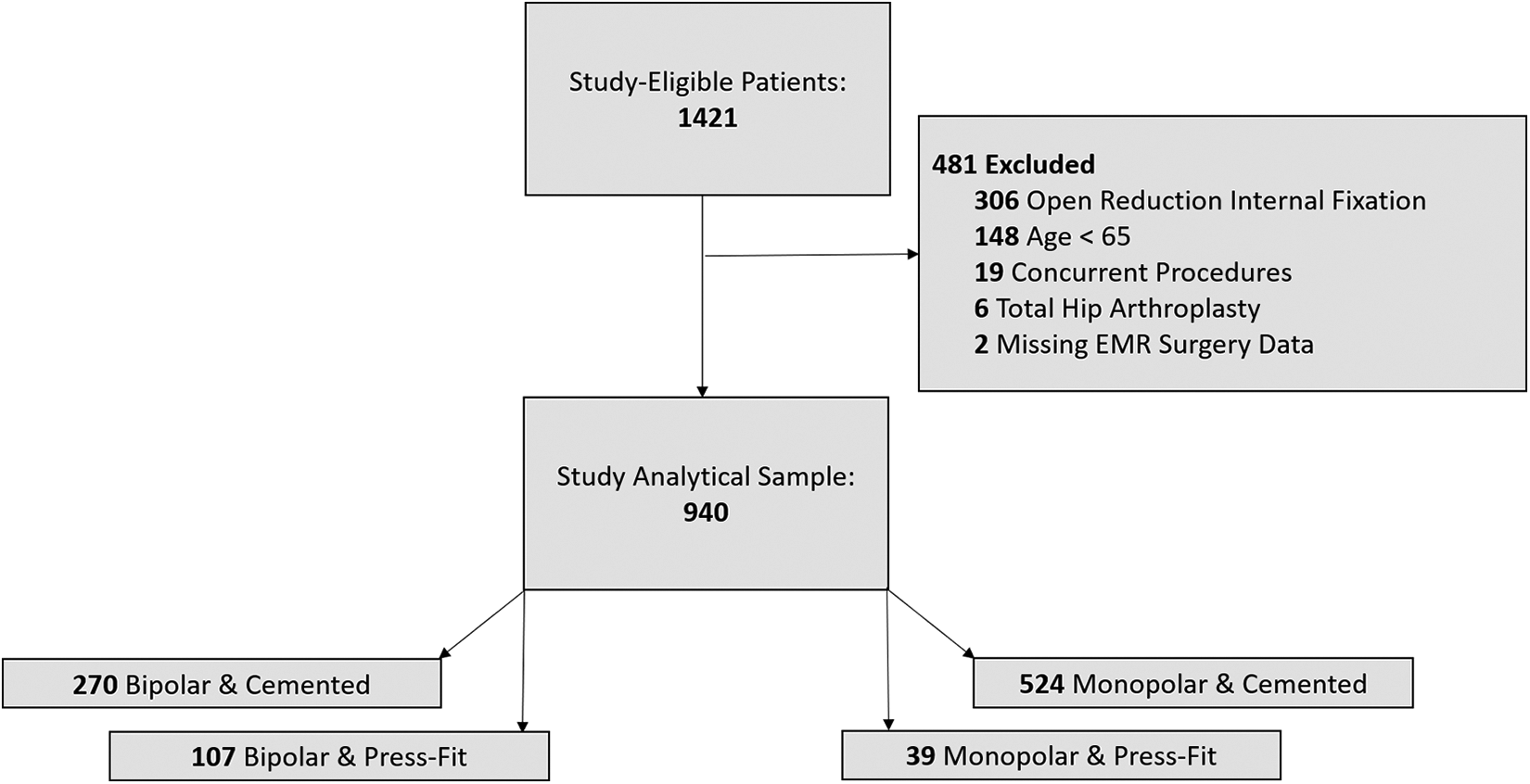
Distributional flow chart of the patient study population.
Statistical Analysis
Statistical analysis consisted of a primary review of the study population (Table 1) and multigroup comparisons of the stratified study cohorts (Table 2) consisting of parametric analysis of variance F-tests and χ2 tests. Multiple linear regression models were generated to assess the covariate influences of implant polarity and cement use to the total construct cost after adjusting for age, gender, and BMI. Additionally, goodness-of-fit regression models were constructed to evaluate the correlation of construct costs to the identified injury and noninjury characteristics. Lastly, the frequency of implant type was graphed in-relation to the year of surgery (Figure 3). All statistical analyses were conducted using SAS 9.4 (SAS Institute). Study data were compiled and maintained via Microsoft Excel on a secure hospital server (Microsoft Corporation).
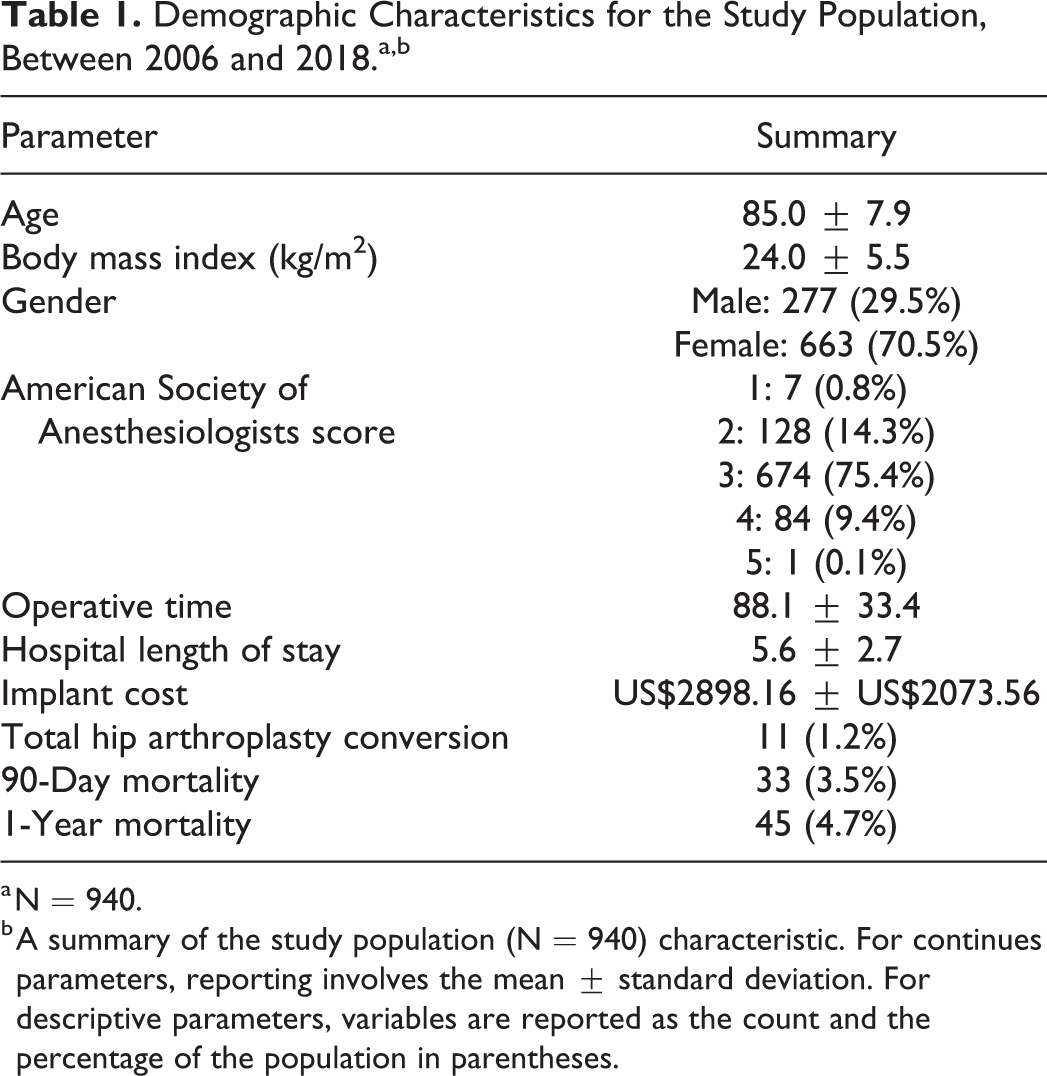
Demographic Characteristics for the Study Population, Between 2006 and 2018.a,b
a N = 940.
b A summary of the study population (N = 940) characteristic. For continues parameters, reporting involves the mean ± standard deviation. For descriptive parameters, variables are reported as the count and the percentage of the population in parentheses.
Study Population Characteristics, Stratified by the Implant Used in Hemiarthroplasty Procedures, Between 2006 and 2018.a,b

a N = 940.
b A summary of study population characteristics relating to samples’ demographics and injury patterns.
c Resulting P value from a one-way analysis of variance F test.
d Resulting P value from a χ2 test between the three treatment arms.

A review of the implant construct utilization for hemiarthroplasty procedures, years 2006 to 2018 inclusive.
Source of Funding
There was no funding used in this investigation.
Results
Overview of Patient Sample
A total of 940 patients meeting inclusion criteria were identified. In summary of the study population, 663 (70.5%) were female and 227 (29.5%) were male. The study population had a mean age of 85.0 ± 7.9 years with a mean BMI of 24.0 ± 5.5 kg/m2. Age at the time of surgery of the patients receiving a cemented implant was 85.6 ± 7.0 years and 81.8 ± 10.9 years in the population receiving a press-fit implant (P < .01). The majority of the patient population had an ASA score of 3 (75.4%; Table 1). The mean hospital length of stay was 5.6 ± 2.7 days. A total of 11 (1.2%) patients were converted to THA. The conversion rate to THA was highest among patients receiving bipolar press-fit implants, 4 (3.7%; Table 2). All patients converted to THA had a chief complaint of hip or groin pain. A total of 33 (3.5%) patients died at the 90-day postoperative mark and 45 (4.8%) patients at the 1-year mark (Table 1). Neither 90-day (P = .56) nor 1-year (P = .24) mortality was statistically significantly different between the 4 patient cohorts (Table 2).
Operative Time
The overall mean operative time was 88.1 ± 33.4 minutes. The mean operative time was greatest in bipolar cemented implants, 102.8 ± 35.1 minutes, and lowest in monopolar cemented implants, 79.0 ± 29.8 minutes (Table 2). Operative time was significantly different between monopolar, 79.8 ± 30.8 minutes, and bipolar implants, 100.4 ± 33.5 minutes (P < .01). Operative time was similar between cemented, 87.1 ± 33.6 minutes, and press-fit implants, 93.6 ± 32.0 minutes (P < .02).
Implant Selection
The use of monopolar cemented implants remained fairly consistent at 60% between 2006 and 2011, then dropped to 12.1% in 2013 and 10.0% in 2014. Following 2014, the usage of monopolar cemented implants dramatically increased to 83.3% by 2018. Monopolar press-fit implants ranged between 0% and 11.7% across the 12-year study period, comprising 1.5% of total constructs in 2018. The use of bipolar cemented implants varied between 10% and 54.3% across the 12-year study period and comprised 10.6% of implants in 2018. Lastly, bipolar press-fit constructs peaked in 2013 at 57.6% and experienced a consistent decline in use to 4.6% in 2018 (Figure 3).
Construct Costs
The mean construct cost for the entire patient population was US$2898.16 ± US$2073.56 (Table 1). Bipolar press-fit constructs had the greatest cost, US$3900.61 ± US$2607.54, with monopolar cemented constructs averaging the least cost, US$2618.68 ± US$1834.16 (Table 2). Multiple linear regression models formulized the total construct cost as: Construct Cost = US$2801.35 ± US$565.50 (Bipolar) − US$559.57 (Cement Use) after adjustment for age, gender, and BMI. Per this regression model, a monopolar cemented construct is the least expensive, US$2241.78, versus a bipolar press-fit construct is the most expensive, US$3366.85 (Table 3).
Linear Beta Coefficients (β) and 95% Confidence Intervals for Association of Implant Makeup to Overall Implant Cost, 2006 to 2018.a,b

a N = 940.
b Linear model results for association between implant makeup to overall implant cost.
c Parameter of polarity is evaluated with monopolar constructs as the set reference.
d Parameter of cement is evaluated with non-cemented constructs as the set reference.
e Adjusting for demographic variables of: age, BMI, and gender.
Discussion
Previous studies have reported an increased cost associated with bipolar implants, but to our knowledge, no previous study has evaluated the costs associated with various combinations of hip hemiarthroplasty constructs. Our study identifies monopolar cemented constructs as the least expensive, US$2618.68 ± US$1834.16, and bipolar press-fit as the most expensive construct, US$3900.61 ± US$2607.54. Both bipolar polarity and cemented fixation influence cost in nearly equivalent and opposite directions. Additionally, we did not find an increase in operative time associated with cemented implants. Selection of the most cost-conscious implant, monopolar cemented, has steadily increased from a low of 10% in 2014 to a high of 83.3% in 2018. Our results indicate that the implant selection choices of individual surgeons have a significant impact on the cost of care. The cost implications of implant selection is one variable to be considered by orthopedists seeking to maximize value of care.
Our study found an increase in implant cost of US$565.50 attributable to the utilization of a bipolar implant versus a monopolar implant. Current AAOS guidelines recommend selection of a monopolar rather than bipolar implant due to decreased cost and largely equivalent functional outcomes. 3 Theoretically, the additional inner-articulation of the bipolar prosthesis design results in a better range of motion and improved functional outcomes. However, studies have found that the bipolar articulation loses functionality over time and ultimately results in the bipolar prosthesis functioning as a monopolar construct. 17 -19
Few quality studies have analyzed construct cost differences in hip hemiarthroplasty procedures in the United States in the past 20 years. A 1998 study by Cornell et al demonstrated a US$690 increase in cost associated with bipolar versus monopolar implants, significantly higher than the US$565.50 cost in our study for bipolar implant selection. 9 Moreover, several recent studies associating implant selection with cost have been conducted internationally. Stoffel et al 7 found that bipolar implants were on average 1000 AUD (Australian dollar, equivalent to about US$662) greater than monopolar implants and Hedbeck et al 20 found that bipolar implants were 1800 SEK (Swedish Krona, equivalent to about US$185) more expensive. These results may reflect the different market pressures of dissimilar health care systems and it would likely be inappropriate to extrapolate these results to the US market. Nevertheless, our results also demonstrate increased cost associated with bipolar implants and are consistent with previous studies.
Our study found a reduction in overall implant cost of US$559.57 associated with the use of a cemented implant versus a press-fit implant. Unlike reports comparing prosthesis polarity, studies comparing prosthesis fixation methods have not clearly examined the cost-efficacy of cemented and press-fit hemiarthroplasty constructs. American Association of Orthopaedic Surgeons guidelines endorse cemented fixation due to evidence suggesting reduced post-operative pain and better mobility. 21 Like our study, Santini et al found that press-fit implants are more expensive, €1980 (Euros, equivalent to about US$2151), than cemented implants, €1065 (equivalent to about US$1157). 22 Conversely, Manoharan et al found cemented hemiarthroplasty to cost £501.42 (British Pound, equivalent to about US$648) more on average than press-fit hemiarthoplasty. 23 Tripuraneni et al similarly determined cemented constructs were US$418.87 more expensive than cement-less constructs. 24 However, this study was underpowered, including a small number (N = 94) of participants operated on by only 2 surgeons. The difference in cost is likely largely impacted by the surgeon implant preferences and institution negotiated prices.
In addition to the costs attributable to implant selection, an often-repeated sentiment is that press-fit constructs decrease operative time which results in decreased cost. However, our study found that the use of cemented implants, 87.1 minutes, does not significantly increase the operative time as compared to press-fit implants, 93.6 minutes. A 2011 Cochrane review comparing cemented and press-fit hemiarthroplasty demonstrated superior performance by cemented implants in terms of postoperative pain, function, and implant-related complications with the downside of a longer operation time. 21 More recent meta-analyses, such as Kumar et al, have found similar results with press-fit hemiarthroplasty being 6.4 minutes faster than cemented. 25 Contrary to these results and our hypothesis, our study found that using a cemented construct does not increase operative time. Few studies have also found decreased or no difference in operative time between cemented and press-fit arthroplasty. Moerman et al found no difference in mean operative time (57.3 vs 55.4 minutes) in cemented and press-fit hip hemiarthroplasty. 26 They postulated that their results were influenced by the academic nature of the institution. 26 However, our study included both academic and nonacademic medical centers and we believe the difference in operative time between cemented and press-fit implants is due to the influence of individual surgeons.
The sharp incline in the utilization of cemented monopolar implants following the release of AAOS guidelines in 2014 suggests these guidelines permeated the orthopedic community and impacted practice patterns. 3,5 However, guidelines alone are not enough to maximize value-centric care without physician and institutional alignment. Physicians are increasingly called to assume leadership roles in the emerging emphasis on the application of evidence-based practice and value-centric care. No value-based incentives (gainsharing, etc) were provided to the surgeons included in our study, thus their behavior was not financially motivated. However, to further incentivize physicians to adopt value-based behaviors, organizations should consider rewarding surgeons whose practice emphasizes value-centric care.
Surprisingly few quality-control studies evaluating the cost-efficiency of hemiarthroplasty implant selection have been conducted in the United States within the past 20 years. Increased investigation surrounding cost and value is vital given the unique nature of the US medical device industry and the increasing frequency of geriatric hip fractures. This study is the first to directly examine the cost of various implant combinations and fixation strategies for hip hemiarthroplasty within a geriatric patient population. A strength of this study is the relatively large sample size derivative of a single-contract, multi-center health system. Thus, differences in costing contracts should not influence cost variation. Additionally, this is the first study to examine the impact of the 2014 AAOS guidelines for geriatric hip fractures on implant selection in hip hemiarthroplasty among US orthopedic surgeons.
Our study also contains a few mentionable limitations. First, this study only accounts for the costs attributable to implant selection but does not tabulate costs across patients’ entire episode of care. Deriving the total episode cost of care requires significant investment of time and resources but allows for greater knowledge of the holistic impacts of implant selection and their related costs. Given the nature and aims of this study, we were also unable to reliably capture postoperative and functional outcomes of the study population outside of 90-day and 1-year patient mortality. Parameters of discharge destination, postoperative complications, and reoperation were not able to be reliably collected and deemed outside the scope of this investigation. Additionally, this study has limitations inherent to a retrospective review as we were unable to correct for selection biases or examine long-term functional outcomes for each hip hemiarthroplasty construct.
Conclusions
Differences in implant cost cannot be disregarded given the vast number of hip hemiarthroplasties performed and the increasing burden on health care institutions to provide value-based care. The use of a bipolar or press-fit implant significantly increases construct cost despite little evidence in the literature of improved functional outcomes. Our study found cemented implants do not increase operative time. Encouragingly, selection of the most cost-conscious implant, monopolar cemented, has increased since 2014, which may reflect the influence of current AAOS guidelines.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.