
Abstract
Introduction
The comparative results of early hip fracture surgery including mortality and postoperative complications in Thailand were not reported. Therefore, we conducted this study to compare the outcomes between patients who received hip surgery within and after 24 hours.
Methods
A retrospective study was conducted at a single center, a tertiary private hospital in Thailand. The medical records of patients who were admitted from 2018 to 2020 were reviewed. Patients aged <50 years, high-energy fracture, pathological fractures, or multiple traumas were excluded. The patients were categorized into two groups for comparison: surgery within and surgery after 24 hours groups. The outcome measures were in-hospital, 30-day, and 1-year mortality rates, length of stay, and the incidences and severities of postoperative complications.
Results
A total of 276 hip fracture patients were analyzed, with the majority (77.9%) undergoing surgery within 24 hours. Patients who underwent earlier surgery had a significantly shorter hospital stay [6 (4, 9) vs 8 (7, 13) days, P < .001]. The cumulative mortality rates at in-hospital, 30 days, and 1 year were 0%, 1.1%, and 2.5%, respectively. The most common postoperative complications observed were anemia (43.1%) and acute kidney injury (32.6%). However, there were no statistically significant differences in mortality rates (P > .05) or postoperative complications (P = .410) between the two groups.
Conclusion
While surgery within 24 hours showed some benefits, such as a shorter hospital stay and reduced pain rescue, it did not reduce mortality or major complications in hip fracture patients.
Introduction
Hip fracture has become a worldwide major public health concern. Due to the global aging population, the number of hip fracture cases will reach 2.6 million in 2026 and 4.5 million in 2050. 1 By 2050, it is predicted that Asian elderly will account for more than 50% of all osteoporotic fractures. 2 According to the World Health Organization (WHO), the life expectancy in Thailand was around 78 years. 3 In Thailand, incidence of hip fracture is more likely to increase, 4 and 1-year mortality rate of hip fracture patients has been reported, ranging from 17% to 19%.5-7 Moreover, hip fracture patients tended to be dependent, and the fracture also negatively affected quality of life. 8
Options for treating hip fractures comprise conservative and operative treatment. Due to many disadvantages of conservative treatment, especially prolonged immobility and high in-hospital complications,9,10 operative treatment was preferred. Early operative treatment contributed to improved functional outcomes, 11 shortened length of stay, 12 reduced duration of pain, 13 decreased postoperative complications, and lower mortality compared to conservative treatment.14-16 However, the reported 1-year mortality rate remained high and varied among different nationalities, ranging from 17% to 29%.7,17-20 The postoperative complications including myocardial infarction, venous thromboembolism, pneumonia, and delirium seemed to be the causes of high mortality.21-24 Many factors were considered to be related to mortality rates such as age, sex, underlying disease, anesthesia technique, and ASA (American Society of Anesthesiology) physical status.25-29 Another factor of concern was the time to operation. It has been proved that delayed time to operation was associated with increased mortality.14,15 However, the definition of delayed surgery, whether 24, 48, or 72 hours, was still under debate. Although, mortality rates after hip fracture surgery and associated factors have been reported in Thailand,5-7,25 previous studies did not report mortality rates of patients who had undergone early surgery.
The primary objective of this study was to report in-hospital, short-term (30 days), and long-term (1 year) mortality rates after hip fracture surgery in Thonburi hospital, a private hospital with high-quality service and a well-established interdisciplinary care team for facilitating hip fast-track surgery. The interdisciplinary care team or ortho-geriatric ward are established only in high resource hospitals such as university hospitals or tertiary private hospitals. Secondary objectives were to compare postoperative complications and length of stay between the patients who underwent hip fracture surgery within 24 hours and after 24 hours.
Methods
This retrospective study enrolled hip fracture patients who underwent urgent surgical fixation or hip arthroplasty at Thonburi Hospital in Bangkok, Thailand. The medical records of those who were admitted from 2018 to 2020 were reviewed. Patients aged more than 50 years and followed up for at least 12 months were included. Patients with multiple fractures, hip fractures from high-energy trauma, diagnosed with a pathological femoral fracture, or insufficient data at baseline/30-day/12-month follow-up were excluded. The protocol for this study was approved by Siriraj Institutional Review Board, and informed consent was waived due to the use of retrospective data. All methods were carried out in accordance with the Declaration of Helsinki.
Hip fracture protocol at Thonburi Hospital
In the hip fast-track protocol, the patients diagnosed with low-energy or osteoporotic hip fractures, the operative or non-operative treatment were assessed by an interdisciplinary care team. All patients were admitted to the orthopedic unit, and routine preoperative laboratory tests were done. Cardiologists/general medicine/geriatricians were consulted on age-related or cardiovascular issues, and additional investigations were performed if warranted. Any other medical problems were optimally treated before the operation. The anesthesiologists experienced in anesthesia for hip surgery was responsible for anesthesia and acute pain management. Multimodal pain management (femoral nerve block or fascia iliaca block or local wound infiltration, oral and intravenous analgesics) was used in preoperative, intraoperative, and post-operative periods. Orthopedists who have expertise in hip fracture surgery carried out all the procedures. The goal was to treat all hip fractures surgically as soon as possible after admission. Generally, the patients were advised to ambulate with weight-bearing as tolerated by a walker as soon as possible after surgery, under the supervision of ward nurse, physical therapist, or attending physicians. All patients were enrolled in the post-hip fracture protocol, and osteoporotic investigations were performed. The patient profiles were reviewed by the metabolic bone disease specialist team. The non-pharmacological and pharmacological treatment of osteoporosis was recommended. Fall prevention including home modification was advised by an interdisciplinary team including video-based osteoporosis education. Once the patient was deemed fit to be discharged, basic exercises, and home physical therapy information were given to all patients and caregivers. They were made an appointment to follow the clinical conditions at the orthopedic clinic.
Variables and Outcome Measurement
Patient data, including age, sex, body mass index (BMI), Charlson Comorbidity Index (CCI), underlying diseases, ASA classification, fracture location, time to operation, and type of fixation were collected. Other preoperative data included laboratory results (complete blood count and blood chemistry), special investigations, and medications aside from routine preoperative medications. The intraoperative data included types of surgeries, anesthesia techniques, total blood loss, blood transfusion, fluid, anesthetic time, operative time, and intraoperative complications. The postoperative data included intravenous rescue analgesia (morphine or pethidine) within 24 hours postoperatively, length of hospital stay, and in-hospital complications. The in-hospital, 30-day, and 1-year mortality rates after hip fracture surgery were primary outcomes and the secondary outcomes were incidences and severities of postoperative complications. All outcome measures were compared between early and late hip fracture surgery, using 24 hours as a cutoff point.
Mortality
After hospital discharge, all hip fracture patients were regularly scheduled at the orthopedic clinic to follow the clinical conditions. The in-hospital, 30-day, and 1-year mortality were collected from medical records or telephone follow-ups by trained registered nurses who were not involved in the study.
Complications
In the present study, we assessed only in-hospital complications categorized into intraoperative and postoperative complications. The anesthetic complications were intraoperative hypotension defined as a patient’s mean arterial pressure (MAP) of less than 65 mmHg, systolic blood pressure (SBP) of less than 90 mmHg, or a MAP or SBP value of less than 20% of baseline blood pressure in patients previously diagnosed with hypertension for at least 1 minute at least 1 time. 30 Patients were designated as having severe hypotension if they had SBP of less than 80 mmHg for more than 10 minutes related to risk of an end-organ specific injury. 31 For postoperative complications, we collected occurrences of anemia, myocardial infarction, heart failure, significant arrhythmia, deep vein thrombosis, pulmonary embolism, pneumonia, respiratory failure, cerebrovascular disease, acute kidney injury, delirium, sepsis, and others. Full definitions of each postoperative complication are provided in Supplementary Table 1. All postoperative complications were graded based on severity using Clavien-Dindo Classification (Supplementary Table 2). 32
Sample Size
Sample size was calculated based on the estimated mortality rate 1 year after hip fracture. In a previous study, Haleem et al 17 reported that 1-year mortality rate was 22%. According to a 95% confidence interval, with a probability of error of .05, at least 264 patients were required for this study. Retrospective data spanning 3 years were collected to ensure an adequate sample size based on the number of patients treated annually at the hospital.
Data Analysis
The in-hospital, 30-day, and 1-year cumulative mortality rates were analyzed and compared between the patients who underwent early surgery within 24 hours and later than 24 hours. Also, rates of postoperative complications were assessed and compared between the two groups.
Baseline patient characteristics and outcomes measure were assessed for normality using Kolmogorov-Smirnov test. The continuous data were presented in mean and standard deviation or median and interquartile range as appropriate. The Student's t-test or Mann-Whitney U test was used to compare continuous data with normal and abnormal distribution. The categorical data were presented in frequency and percentage. The Chi-square or Fisher exact test was used to compare categorical data. Statistical significance was considered as a P-value less than .05. All data were analyzed using the SPSS version 18.0 (IBM Corp., Armonk, NY, USA).
Results
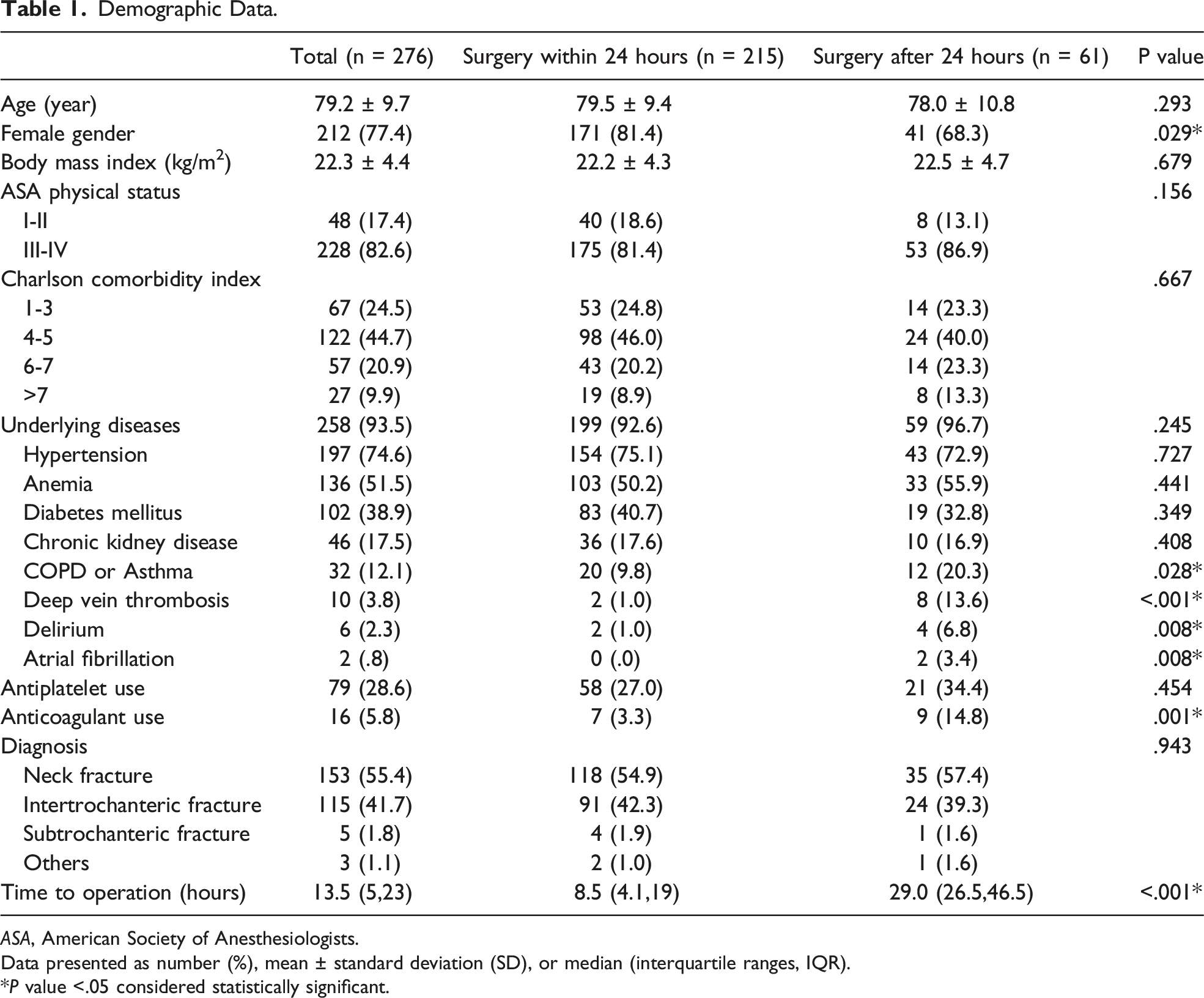
A total of 276 patients were included and analyzed in this study (Figure 1). The patients had a mean age of 72.9 ± 9.7 years with females predominately (77.4%) and 82.6% of patients were in ASA classification III-IV. The majority of patients (44.7%) had CCI scores of 4 to 5. Hypertension (74.6%), anemia (51.5%), and diabetes mellitus (38.9%) were the 3 main underlying diseases. On hospital arrival day, 28.6% of patients used antiplatelets, and 5.8% received anticoagulants. The two main diagnoses were femoral neck fracture (55.4%) and intertrochanteric fracture (41.7%). Most patients came to the hospital on the day of the accident. Most patients (77.9%) underwent surgery within 24 hours. The median time to operate in surgery within and after 24 hours was 8.5 (4.1,19) and 29.0 (26.5, 46.5) hours, respectively. When comparing the two groups, earlier surgery patients were more likely to be female (81.4% vs 68.3%, P = .029), and had fewer comorbidities (COPD or asthma, deep vein thrombosis, delirium, and atrial fibrillation). The proportion of patients using anticoagulants was lower in the surgery within 24 hours group (3.3% vs 14.8%, P = .001) (Table 1). Flow diagram of the present study. Demographic Data. ASA, American Society of Anesthesiologists. Data presented as number (%), mean ± standard deviation (SD), or median (interquartile ranges, IQR). *P value <.05 considered statistically significant.
Preoperative Investigations and Preparation.

eGFR, estimated glomerular filtration rate; BUN, blood urea nitrogen.
Data presented as number (%) or mean ± standard deviation (SD).
*P value <.05 considered statistically significant.
Intraoperative and Anesthesia Parameters.

Data presented as number (%), mean ± standard deviation (SD), or median (interquartile ranges, IQR).
*P value <.05 considered statistically significant.
Length of Stay, Mortality, and Postoperative Complications.

Data presented as n (%), or median (interquartile ranges, IQR).
*P < .05 considered statistically significant.
Discussion
The present study revealed that the mortality rate of patients with fragility hip fracture during admission, at 30 days and 1 year was 0%, 1.1%, and 2.5%, respectively. Additionally, there was no significant difference in the occurrence of postoperative complications, 30-day mortality, or 1-year mortality between hip fracture patients who had undergone surgery within 24 hours and surgery later than 24 hours.
Regarding the 1-year mortality of hip fracture patients in Thailand, the previous studies reported 1-year mortality ranging from 17% to 19%, which was considerably high compared to our results.5-7 The possible explanation for divergent results was the previous studies included hip fracture patients treated with operative and conservative treatment for analysis, with varying proportions of patients treated non-operatively among studies ranging from 14% to 47%. On the contrary, this study included only patients who had undergone surgery with early surgery predominated. It had been proven that patients treated with conservative treatment had a higher risk of mortality and postoperative complications than those treated with surgery,10,16,25 and this may contribute to greater mortality rates in the previous studies. For a similar reason, the in-hospital mortality rate reported by Chariyalertsak et al, 7 which accounted for 2.1%, was relatively higher than the results of this study.
Although, several clinical practice guidelines for early hip fracture surgery recommend surgery within 48 hours,33,34 we attempted to set a lower cut-off time point in order to improve outcomes after surgery. Our hospital is a tertiary hospital with a high bed capacity, abundant operating rooms, and medical personnel. Therefore, resources were not a limitation for treating hip fracture patients. All hip fractures would be treated surgically within 24 hours if they had no contraindications. After initial screening, around 22% of patients were assigned to the late surgery group. Although the CCIs between the two groups were not significantly different, the results revealed that the patients in the later surgery group had more comorbidities (lung diseases, deep vein thrombosis, delirium, and atrial fibrillation) and underwent more echocardiograms. Thus, we assumed that the delayed surgery may result from time spent on pre-operative optimization.
There is still controversy about the definition of early surgery whether 72, 48, 36, 24 hours, or an earlier period, which resulted in inconsistent mortality rates at different time points among studies.15,35 For 24-hour threshold, the previous prospective cohort studies and meta-analysis showed that early surgery within 24 hours was not associated with improved mortality rate either in the short or long term.13,35,36 This outcome was in line with the present study that designated surgery later than 24 hours as late surgery. Moreover, the mortality rate did not decrease even in ultra-early surgery within 6 hours. 37
The apparent benefits of early surgery were decreased amount of rescue analgesia within 24 hours postoperatively and length of hospital stay, which was in line with the previous study. 13 Although we could not draw a conclusion that why earlier surgery had positive effects on pain, we hypothesized that earlier surgery might minimize soft tissue damage and contributed to less postoperative pain and less opioid use. For the length of hospital stay, there was an average difference of 2 days between the two groups, whereas the average difference in time to surgery was around 20.5 hours. Consequently, we postulated that not only time spent on pre-operative optimization but also the duration of hospital stay could be influenced by the postoperative phase, characterized by pain management, predominantly through the administration of opioid analgesics to facilitate gradual ambulation. As established in existing literature, opioids are associated with numerous adverse effects, including ileus, nausea, and vomiting, undoubtedly influencing postoperative functional outcomes and the length of stay. 36
The majority of complications in this study were grade II, which only required blood transfusions for treatment. However, early surgery did not reduce occurrence of postoperative complications in any severity grading (grade I to IV). Reduction of minor and major complications might be clearly distinguished if the cut-off point for early surgery was extended to 48 hours.35,38
Other than early surgery in hip fracture patients, the interdisciplinary care team approach and well-established hip fracture care pathway in our hospital may contribute to low mortality rates. This assumption was supported by the results of previous studies conducted in hospitals that had similar settings to ours.39-42 The studies revealed that the interdisciplinary care protocol in hip fracture patients treated with surgery could reduce the length of hospital stay, postoperative complications, in-hospital, and 30-day mortality rate. Thus, we encouraged all hospitals to develop and implement the interdisciplinary care protocol in the treatment of hip fracture patients. Despite the optimal time for hip fracture surgery still being debated, the surgery should be performed instantly when the patients are in stable clinical conditions.
This study collected data from a private tertiary hospital. All hip fracture patients followed hip fast-track guidelines and were treated by the interdisciplinary care team. Hence, the results presented in this study are representative of the patients treated in a condition of high-resource setting and well-established hip fracture treatment protocol. There are some mentioned limitations in this study. First, this study collected data from Thai patients who were quite healthy (CCIs less than 6) and admitted to a tertiary private hospital with well-established hip fracture protocol management and a highly experienced interdisciplinary care team. Thus, our results may not be generalizable to patients with multimorbidity and community-based hospitals where resources for managing hip fractures among the elderly are limited. Second, the cause of death could not be specified in some patients because we partly collected data from telephone interviews. Third, we evaluated the 30-day and 1-year mortality only and found no different mortality rates between the surgery within and after 24 hours. However, a longer time frame beyond a 1-year follow-up may demonstrate a significant difference. Although, the mortality rate of hip fracture patients treated with surgery was fairly low, further research to identify modifiable factors associated with mortality and predicting mortality using the prognostic model with external validation is still warranted.
Conclusion
The overall mortality rate of hip fracture patients treated surgically with an interdisciplinary care team was low. Early surgery within 24 hours did not have a beneficial effect on mortality and complications of hip fracture patients. However, this study proved that surgery within 24 hours could reduce postoperative pain and length of hospital stay. If resources, operating rooms, and medical personnel are available, and there is no contraindication for early surgery, we encourage hip fracture patients undergo surgery within 24 hours and active management from an interdisciplinary care team be initiated.
Supplemental Material
Supplemental Material - Early Hip Fracture Surgery Within 24 hours did not Reduce the Mortality Rate but Resulted in Less Postoperative Opioid use and a Shorter Length of Stay: A Retrospective Study of 276 Patients From a Tertiary Private Hospital in Thailand
Supplemental Material for Early Hip Fracture Surgery Within 24 hours did not Reduce the Mortality Rate but Resulted in Less Postoperative Opioid use and a Shorter Length of Stay: A Retrospective Study of 276 Patients From a Tertiary Private Hospital in Thailand by Aasis Unnanuntana, Chirathit Anusitviwat, Vasu Lertsiripatarajit, Peerapol Riawraengsattha, and Manee Raksakietisak in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Authors Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by all authors. The first draft of the manuscript was written by Aasis Unnanuntana and Chirathit Anusitviwat, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was supported by Siriraj Research Fund, Grant number R016531006, Faculty of Medicine, Siriraj Hospital, Mahidol University.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.