
Abstract
Introduction
Hip fractures among the geriatric population are an increasingly pressing concern given the expanding aging population worldwide. 1 The adverse effects of such injuries may have a negative impact on functional status and quality of life on patients of all ages, but they may be associated with greater morbidity and mortality among the more fragile aged population.2,3 Identifying the risk factors that predict functional deprivation after a hip fracture and the need for early intervention could reduce the associated economic costs stemming from loss of autonomy 4 and institutionalization, 5 and could also improve the occurrence of postoperative complications. For example, malnutrition is reportedly one of the risk factors that may affect hip fracture healing and rehabilitation, representing an area of great interest because it is both modifiable and highly prevalent in the geriatric population who sustain hip fractures. 6 Malnutrition negatively influences functional recovery after a fracture, in addition to increasing healthcare spending and being associated with high mortality. 7 Several studies have examined the effect of nutritional intervention on postoperative complications in patients undergoing surgical procedure for hip fracture [6-9]. Their results were conflicting, with some studies supporting the effect of nutritional supplements on postoperative complications6,7 and others refuting its effect.8,9 Recent years have witnessed the emergence of high-dose protein formulas (9 gr/100 ml) with a supplement of β-hydroxy-β-methylbutyrate (HMB), a metabolite of leucine, an amino acid. HMB seems to have an anabolic effect on protein metabolism. It was proposed that severe decrease in skeletal muscle and function that occur in the elderly may be mitigated by HBM supplementation, preventing muscle atrophy, such as that induced by bedrest.10-12
The main objective of this study was to evaluate if and how nutritional intervention with oral nutritional supplements (ONS) influences postoperative nutritional status and postoperative complications, including mortality, readmissions, and need for revision surgery.
Materials and Methods
Study Design and Setting
This retrospective cohort study included consecutive patients >65 years of age who were diagnosed with hip fracture Type 31A-C according to the AO/OTA classification,
13
and who underwent either osteosynthesis or arthroplasty in a large tertiary university-affiliated medical center between 2017-2020. Only subjects with a minimum follow-up of 1-year were included. The data were assessed by reviewing electronic medical records, including admission and discharge reports, hospitalization follow-up findings, anesthesia and surgical reports, laboratory details, information on readmissions, and details on outpatient follow-up. The American Society of Anesthesiology (ASA) score was assessed preoperatively by an anesthesiologist. Data on mortality were available in the hospital database by synchronization with the National Ministry of Health. Data on anesthesia were not included due to the high rate of missing information. No data were missing for demographic variables, ASA and Charlson Comorbidity Index (CCI) scores, readmissions, or mortality rates. Patients who underwent surgery that had been delayed for more than 1 week, those with missing body mass index (BMI) data, and those without recorded albumin levels were excluded from the study (Figure 1). The data query was performed by the institutional quality control unit. The results were presented according to the STROBE guidelines for reporting observational research studies. The study was approved by our institute ethical committee which waived informed consent for this anonymous retrospective medical chart review. Study design. ONS, oral nutritional supplement; BMI, body mass index.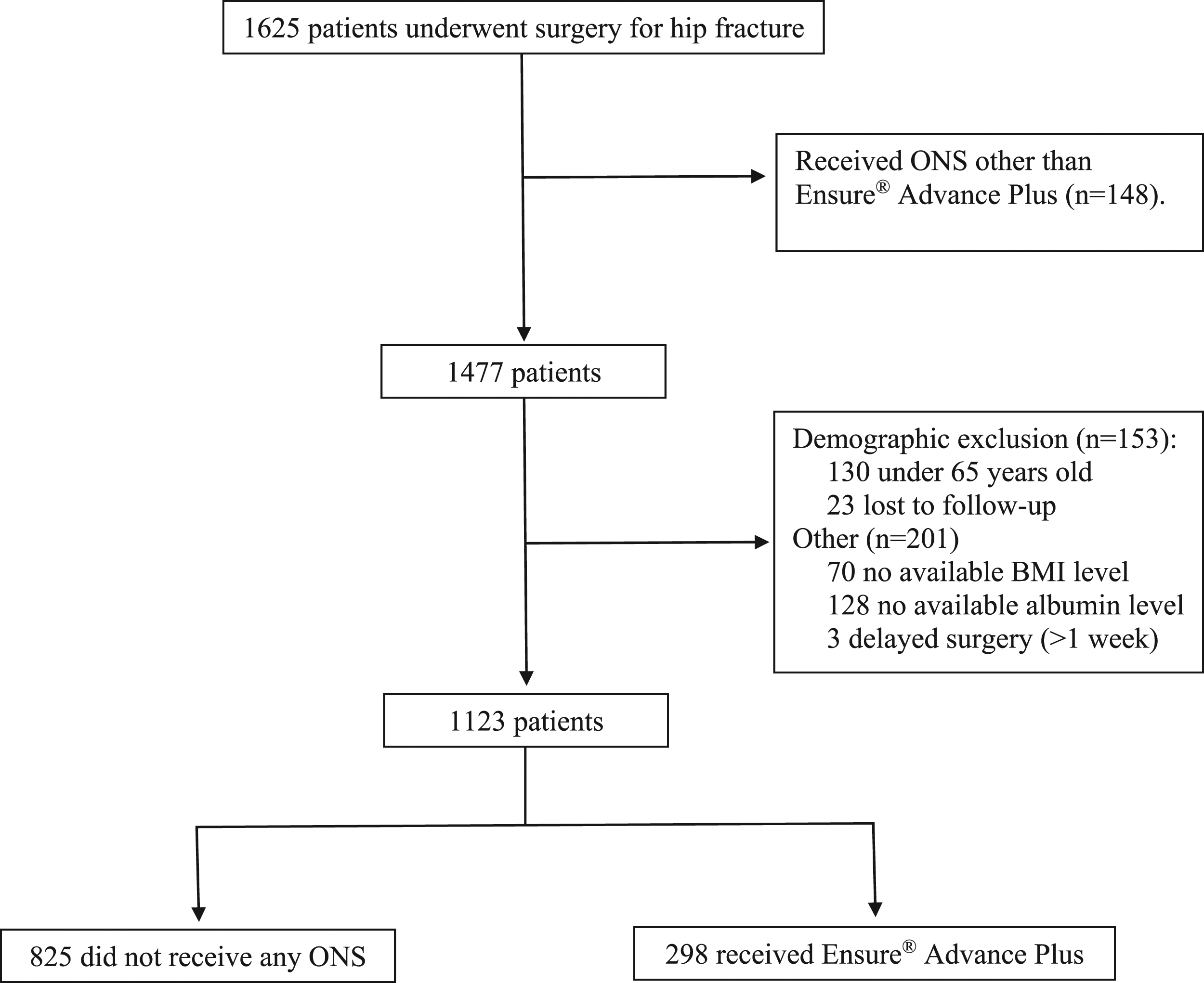
Surgery
All patients were operated by specialists in either joint reconstruction or orthopedic trauma. Surgery type (osteosynthesis vs. arthroplasty) was decided upon by team discussion. Time to surgery was calculated from the time of admission to the emergency department (ED) to the time the patient entered the operating room, and follow-up duration was calculated from the time of surgery until data query and analysis.
Nutritional Intervention
A protocol of nutritional assessment and consultation with a nutritionist was established and first introduced in our center for at risk patients in 2017, becoming routine for all hip fracture patients by 2019. After the initial nutritional assessment that included laboratory and clinical features, ONS were started on postoperative day 1 and were recommended at discharge for a period of 1 month. We were looking for a formula that included high protein levels (9 gr/100 ml) and the HMB supplement and decided upon Ensure® Advance Plus (EAP, 9 gr/100 ml protein and 1.2 gr HMB supplement, Abbott nutrition) for most patients. Glucerna® plus (Abbott Nutrition) was recommended for patients with diabetes mellitus and uncontrolled glucose levels, and Nepro HP® (Abbott Nutrition) for patients with end-stage renal disease. Patients treated with ONS other than EAP were excluded from the study (Figure 1).
Outcome Parameters
The study outcomes included mortality, changes in albumin levels, revision surgery, and readmissions for any cause. Mortality was assessed at 30 days, 90 days, and 1 year after the surgery. Albumin levels were collected from admission and within 1 week after surgery, and changes (Δ albumin) were calculated as the difference between the level at admission and the last one before discharge. The incidence of 30-day or 90-day readmission for any cause and the performance of revision surgery within the follow-up period were assessed from data derived from reviewing the patients’ computerized medical files and from outpatient clinic reports. Infection rates were divided into superficial and deep infection, with “superficial” defined by treatment with antibiotics without the need for revision surgery and “deep” defined by the performance of revision surgery due to the infection.
Statistical analysis All analyses were performed with SPSS version 25 (IBM SPSS statistics, Chicago, IL, USA). Descriptive statistics were applied for patient characteristics. Mean and standard deviations (SD) were calculated for normally distributed continuous variables and compared by Student’s t-test. Frequencies and percentages were calculated for nominal variables and compared between the groups by the Chi-square test. The values of perioperative albumin changes distributed normally and were therefore compared between the 2 groups by Student’s t-test. The percentages of mortality, readmissions, revision surgeries, and infection rates were compared between the groups by the Chi-square test. Significance was set at P < .05.
Results
A total of 1625 consecutive patients who underwent surgical treatment for a hip fracture in our institution between 2017-2020 were included in the study. The final study population consisted of 1123 patients after the exclusion of 502 unsuitable patients (Figure 1). The study group was comprised of 298 patients who received nutritional enrichment with EAP following the surgery, and the control group was comprised of 825 patients who had not received any ONS postoperatively.
Patient characteristics.
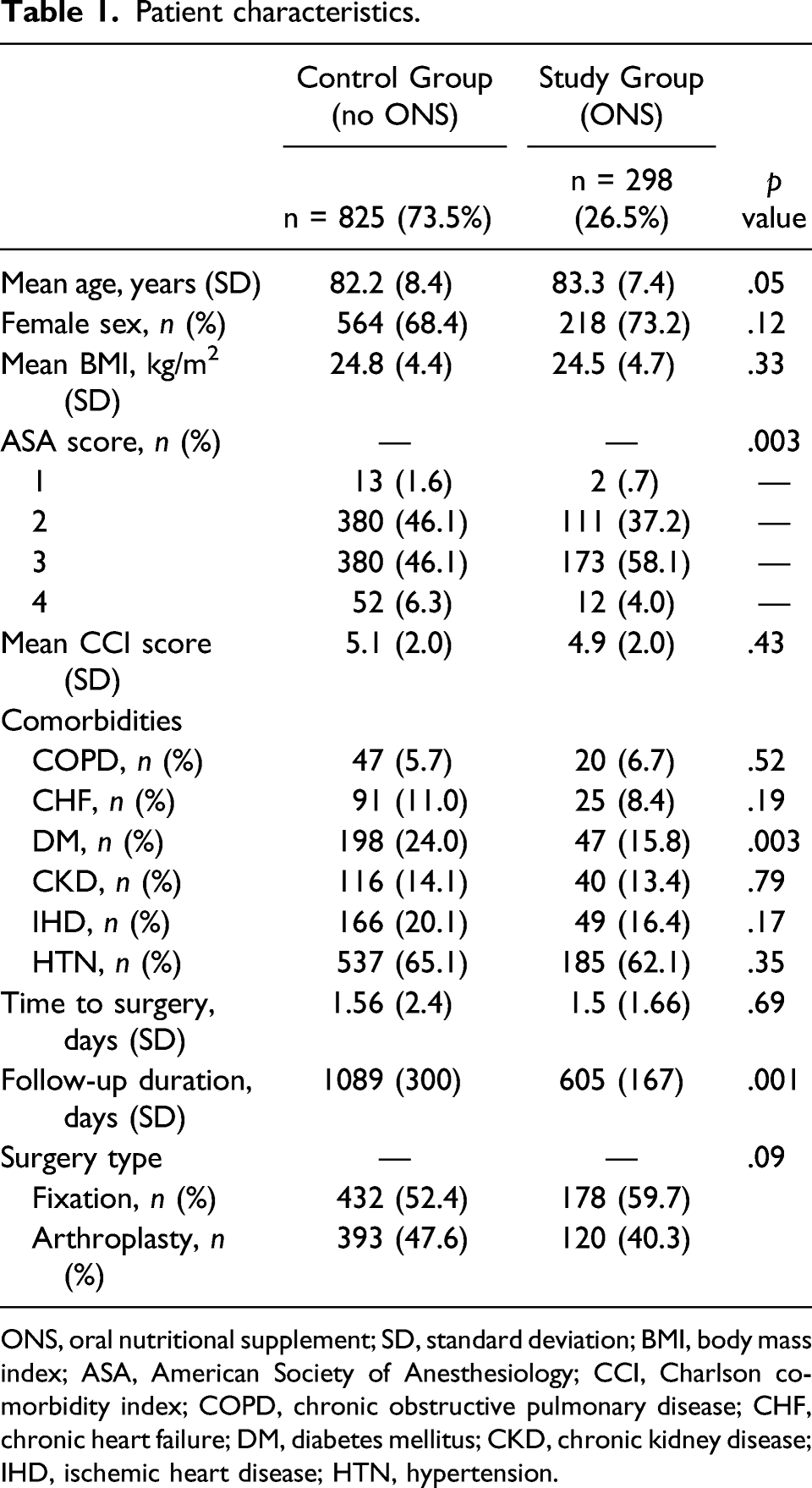
ONS, oral nutritional supplement; SD, standard deviation; BMI, body mass index; ASA, American Society of Anesthesiology; CCI, Charlson comorbidity index; COPD, chronic obstructive pulmonary disease; CHF, chronic heart failure; DM, diabetes mellitus; CKD, chronic kidney disease; IHD, ischemic heart disease; HTN, hypertension.
Outcome parameters.
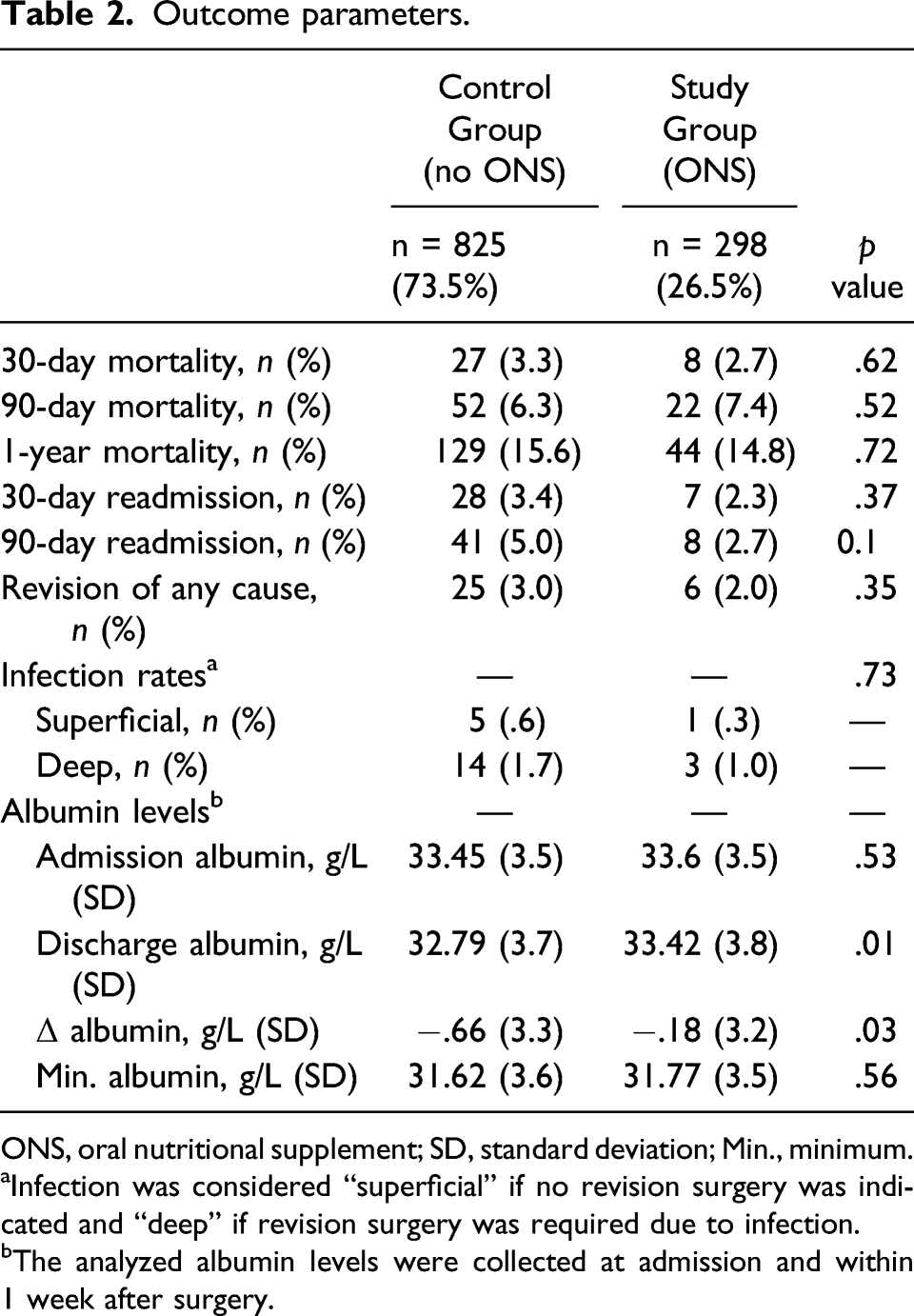
ONS, oral nutritional supplement; SD, standard deviation; Min., minimum.
aInfection was considered “superficial” if no revision surgery was indicated and “deep” if revision surgery was required due to infection.
bThe analyzed albumin levels were collected at admission and within 1 week after surgery.
Discussion
Malnutrition is a subject under lively discussion in geriatric research due to the high prevalence of malnutrition in older people with hip fracture 6 and to the negative influences of malnutrition (including those on functional recovery after fracture) on healthcare spending and association with increased mortality. 7 The interest in malnutrition is further stimulated by the fact that it is treatable, with ONS being a leading treatment modality. However, the role of ONS in reducing postoperative complications and improving nutritional status in patients who sustain a hip fracture and undergo surgery had not been established.
The results of the current study showed that while the consumption of EAP was not associated with change in mortality, readmission, revision surgery, or infection rates, EAP did improve albumin levels, which have traditionally been used as a marker of nutritional status. 14 Similarly, others have observe that the use of ONS improves dietary intake and reduces the risk of complications following hip surgery.15,16 In their review of 12 studies, Grigg et al. 8 evaluated the role of ONS in elderly hip fracture patients: In their review few studies showed that ONS led to a more positive clinical outcome, while most studies found little or no positive results. Wyers et al.’s randomized control trial on intensive nutritional intervention after hip fracture had similar results: nutritional intake and general status improved, but length of hospital stay and clinical outcomes did not. 9 The effect of ONS use on albumin levels and, as a result, the effect of ONS on the patient’s nutrition status has also been assessed in previous studies. Numerus studies have shown no association between nutritional supplementation and an increase in albumin levels,17-21 while others showed a significant increase in albumin levels in supplemented patients.22-25 All of these studies, however, had relatively small cohorts (14-171 patients), and the effect was not observed until 2-4 weeks after surgery in those that found increased albumin levels in the intervention groups. Our cohort included 1123 patients, significantly larger than that of previous studies, and there were significant differences in elevation of albumin levels between our ONS study group and our non-ONS control group within 1 week after surgery, suggesting that the potential of increase in albumin levels associated with ONS use is even greater. The effect of EAP on albumin may be partially explained by HMB. HMB was recently added to high protein ONS (such as EAP) to optimize nutrition supplementation and meet daily requirements of patients with nutritional insufficiencies/deficiencies. HMB exerts its effects through protective, anticatabolic mechanisms, and has been shown to directly influence protein synthesis 26 and mitochondrial dynamics in skeletal muscle. 27 It was also shown to benefit muscle mass and strength of geriatric patients in various other clinical settings [14, 16]. Additional studies have suggested that HMB-enriched ONS seems to be a promising tool to mitigate the decline in muscle mass and preserve muscle function, especially during hospital rehabilitation and recovery.28,29 Current guidelines of the European Society of Parenteral and Enteral Nutrition (ESPEN) recommend that all older adult patients with hip fracture should receive nutritional supplements during hospitalization. 30 The results of the current study and those of the previous ones that reported similar results taken together suggest that paradigms underlying nutritional intervention in the geriatric population after hip fracture should be reconsidered. This study has limitations that bear mention, beginning with its retrospective design and the use of secondary data, which could introduce bias (e.g., missing data, selection bias, and heterogeneity of the study groups). The most important disadvantage of this study is the lack of functional and subjective outcomes that were not available due to the study design. Albumin levels were not assessed at defined time points after surgery, but rather chronologically (at admission and before discharge). Another limitation is that postoperative hospital readmissions included only readmissions to our medical center but not to other institutions. It is possible that our patients were later treated in other medical centers, potentially limiting our access to this information, although this drawback applies to both the study and control groups.
Conclusion
This study is the largest of its kind, and it demonstrated that the use of an oral enriched nutritional supplement was not associated with perioperative complications or mortality, but it did affect nutritional status, as indicated by increased albumin levels, a known marker of nutritional status. The current findings do not support the position that the benefits of ONS use extended to the reduction of major postoperative complications of hip fracture surgery, and further long-term research is needed to evaluate subjective and functional outcomes associated with improved nutritional status.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Study was approved by the medical center’s institutional review board that waived informed consent in view of the retrospective nature of the study and that all the procedures being performed were part of the routine care.