
Abstract
Introduction:
Previous smaller studies suggest that anemia is a risk factor for mortality in patients with hip fracture. The purpose of this investigation was to assess the correlation between hemoglobin at admission with 30-day mortality following a hip fracture in a large-scale study.
Patients and Methods:
From January 1996 to December 2012, all patients with hip fracture (>60 years of age) admitted to Bispebjerg Hospital, Copenhagen, were identified from a local hip fracture database. We excluded conservatively treated patients and patients who died preoperatively.
Results:
Seven thousand four hundred twenty-one consecutive patients with hip fracture were identified. Of those 7319 had a hemoglobin measurement on admission and were thus eligible for further analysis. Mean hemoglobin for patients alive at 30 days was 7.6 (standard deviation [SD]: 1.0) and for deceased patients 7.4 (SD: 1.1), P < .0001. Mean age was 82.6 years (SD: 8.5), and 76.5% of the population were female (Nfemales = 5600). The 30-day mortality decreases for every increase in hemoglobin of 1.0 mmol/L in a univariate analysis (P < .0001). The hazard ratio (HR) with 95% confidence interval (CI) for 30-day mortality in patients with anemia (<7.3 mmol/L for females and <8.3 mmol/L for males; Nanemic = 3235) was 1.66 (CI: 1.43-1.91, P < .0001). Adjusting for age, type of fracture, gender, and comorbidities (Charlson score) slightly attenuated the risk estimate (HR: 1.21, CI: 1.03-1.41, P = .02).
Conclusion:
This study demonstrates increased 30-day mortality in patients with low hemoglobin at admission, even after adjusting for comorbidities.
Introduction
Osteoporosis is diagnosed in 21% of all women and 6% of all men between 50 and 84 years, and the lifetime risk of any of the most common fractures due to osteoporosis is estimated to be 46% for women and 22% for men aged 50 or above. The lifetime risk of hip fracture is estimated to count for more than half of these, 23% in women and 11% in men. This results in a prevalence of 3.5 million fractures per year worldwide. 1
The postoperative comorbidity and complications, such as urinary tract infections, cardiac problems, pressure ulcers, deep venous thrombosis, and pneumonia, 2,3 make the patients a high-risk group in regard to mortality. This is well established in the previously published literature, where 1-year mortality rates are shown to be between 17% and 35%. 4 –9
Given the global increase in life expectancy, 10 the prevalence of hip fractures has been estimated to reach 4.5 million worldwide in 2025. 1 Worldwide indirect and direct costs are estimated to be US$131.5 billion by 2050, 11 due to the substantial rehabilitation, postoperative hospitalization, and complications.
Because of this expected increase in costs, both in economic terms and in human lives, it is important to pinpoint where intervention from the clinician will be the most effective. This can be done through investigation of the impact of different factors on the outcome following a hip fracture. Some factors are nonmodifiable, such as age, gender, type of fracture, hereditary disposition, and comorbidities preoperatively and postoperatively, whereas others are modifiable and the ones that need increased attention. The modifiable factors include physical health, nutrition status, body mass index (BMI), alcohol abuse, sex hormone status, high serum creatinine, low serum albumin, low hemoglobin, pharmacological interventions/comedications (eg, glycocorticoid therapy), time period from fracture to surgery, postsurgery care (eg, institution type), and so on.
Blood tests are stable, easily interpreted, and relatively inexpensive tests. Routine blood tests taken at admission can therefore be a potentially easy way to identify patients at increased risk of dying.
The influence of low hemoglobin levels on mortality in patients with hip fracture has been examined by several smaller studies with limited or no information on comorbidities, and the results pooled in a meta-analysis show excess mortality in patients with low hemoglobin. 12
The aim of this study was therefore to investigate the association of low hemoglobin levels with 30-day mortality in patients with hip fracture in a larger setting, with the possibility of adjusting for comorbidities.
Patients and Methods
Data Sources
The study population was identified in a local database of all surgically treated patients with hip fracture at Bispebjerg Hospital.
Data were subsequently collected from different resources using the social security number. Patient information was anonymized and deidentified prior to analysis.
The databases included were the Danish Civil Registration System (DCRS) and the Danish National Patient Register (DNPR). The DCRS includes all habitants of Denmark. Each person receives a unique identity number, which functions as identification and a social security number. The DCRS stores personal information such as name, address, marital status, place of birth, citizenship, kinship (parents/children), declaration of incapacity, profession, voting rights, municipal circumstances, registration notes, and death. 13 Information from DCRS was combined with information from the DNPR (see Figure 1). The DNPR contains data from all Danish somatic hospitals since 1977. Since 1994, the diagnoses have been coded according to the International Classification of Diseases, 10th Revision (ICD-10). 14

Databases included in the study used to combine and identify information about each patient.
Study Patients
The initial extraction from the local hip fracture database included all surgically treated patients admitted to Bispebjerg Hospital with a fractured hip (femoral neck fracture [57%] ICD-10 code DS720, intertrochanteric femoral fracture [37%] ICD-10 code DS721, and subtrochanteric fracture [6%] ICD-10 code DS722) between January 1996 and December 2012 and aged 60 years or above. Patients treated conservatively and patients who died preoperatively were not included. Seven thousand four hundred twenty-one patients were identified from the database. The hospital laboratory information system was searched for available admission hemoglobin levels (definition: first preoperative hemoglobin measurement following admission and no later than 2 days after admission). Seven thousand three hundred nineteen (98.6%) patients had an admission hemoglobin measurement and comprised the final study cohort.
Comorbidity
The Charlson comorbidity index (CCI) was applied to measure the burden of disease and thus enabling confounder adjustment of the results. The index is based on 22 clinical conditions (myocardial infarct, congestive heart failure, peripheral vascular disease, dementia, cerebrovascular disease, chronic lung disease, connective tissue disease, ulcer, chronic liver disease, diabetes, hemiplegia, moderate or severe kidney disease, diabetes with or without organ damage, tumor, leukemia, lymphoma, moderate or severe liver disease, malignant tumor, metastasis, and AIDS). Each condition is given an associated weight (1, 2, 3, and 6) according to the gravity of the disease. 15
Using the ICD-10 coding algorithm by Quan et al, 16 disease categories were identified from DNPR. The CCI was applied to hospital contacts in the time period from the beginning of January 1977 (establishment of DNPR) until the end of the study, December 2012.
Biochemical Measurements
Anemia was defined as a hemoglobin level below 7.3 mmol/L for women and below 8.3 mmol/L for men at admission, in accordance with the reference intervals for hemoglobin at the Department of Clinical Biochemistry, Bispebjerg Hospital.
Hemoglobin was analyzed using photometric methods. Throughout the study period, the Department of Clinical Biochemistry has participated in external quality assurance programs assuring stable levels.
Statistics
Data analysis was performed using SAS version 9.3 (2011; SAS Institute Inc, Cary, North Carolina) through virtual private network access to Statistics Denmark. The outcome was defined as 30-day mortality. Differences between baseline values of the 2 groups were analyzed using parametric, nonparametric, or categorical statistical methods depending on data nature. Categorical data were analyzed using Pearson χ2 test, and differences between continuous data were compared using unpaired t tests for normally distributed variables and Mann-Whitney U tests for nonnormally distributed variables. Significant differences between the 2 groups were defined as a P value below .05 with 2-tailed tests.
Cox proportional hazards models were used to determine hazard ratios (HRs) for 30-day mortality. Hazard ratios were adjusted for confounders, including age, gender, and comorbidities (CCI). Potential violations of the proportional hazards assumption were evaluated by visual inspection of Schoenfeld residuals over time and did not occur.
Approvals
This study was approved by the data protection agency (j.nr.: 2012-58-0004.)/local number BBH-2014-050 and by Statistics Denmark (project number 704670).
Results
Basic Characteristics
Of the 7319 included patients, anemia was observed in 3142 (42.9%) individuals. The mean hemoglobin level for patients alive at 30 days was 7.6 (standard deviation [SD]: 1.0) and for deceased patients 7.4 (SD: 1.1), P < .0001. The mean age of this population was 82.6 years (SD: 8.5). The majority of the 7319 patients were women 5600 (76.5%). The basic characteristics of the population are summarized in Table 1.
Basic Characteristics According to 30-Day Survival and Mortality.
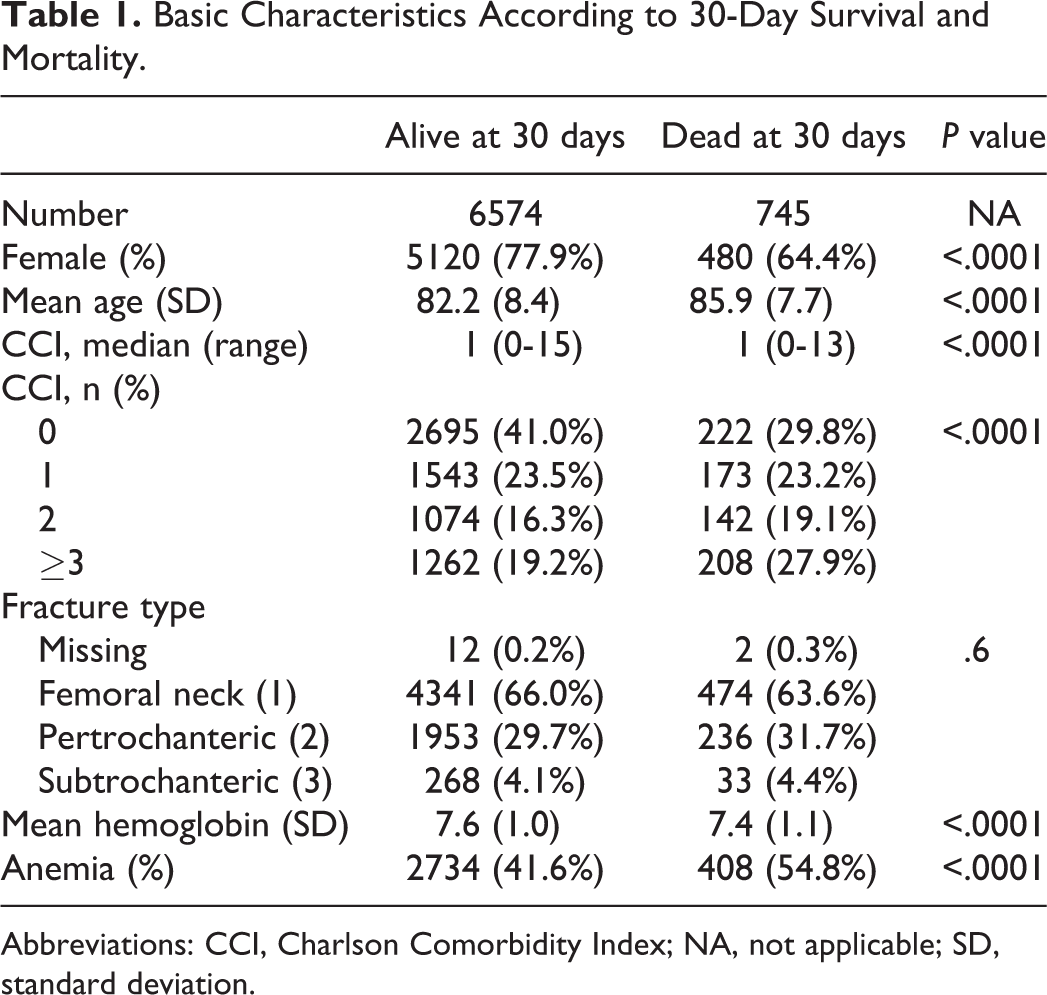
Abbreviations: CCI, Charlson Comorbidity Index; NA, not applicable; SD, standard deviation.
Thirty-Day Mortality
The 30-day mortality for patients with anemia was 13.0% and for nonanemic patients 8.1% (P < .0001). The 30-day mortality decreases for every increase in hemoglobin of 1.0 mmol/L in a univariate analysis (P < .0001), indicating a dose-dependent correlation with mortality (see Figure 2).
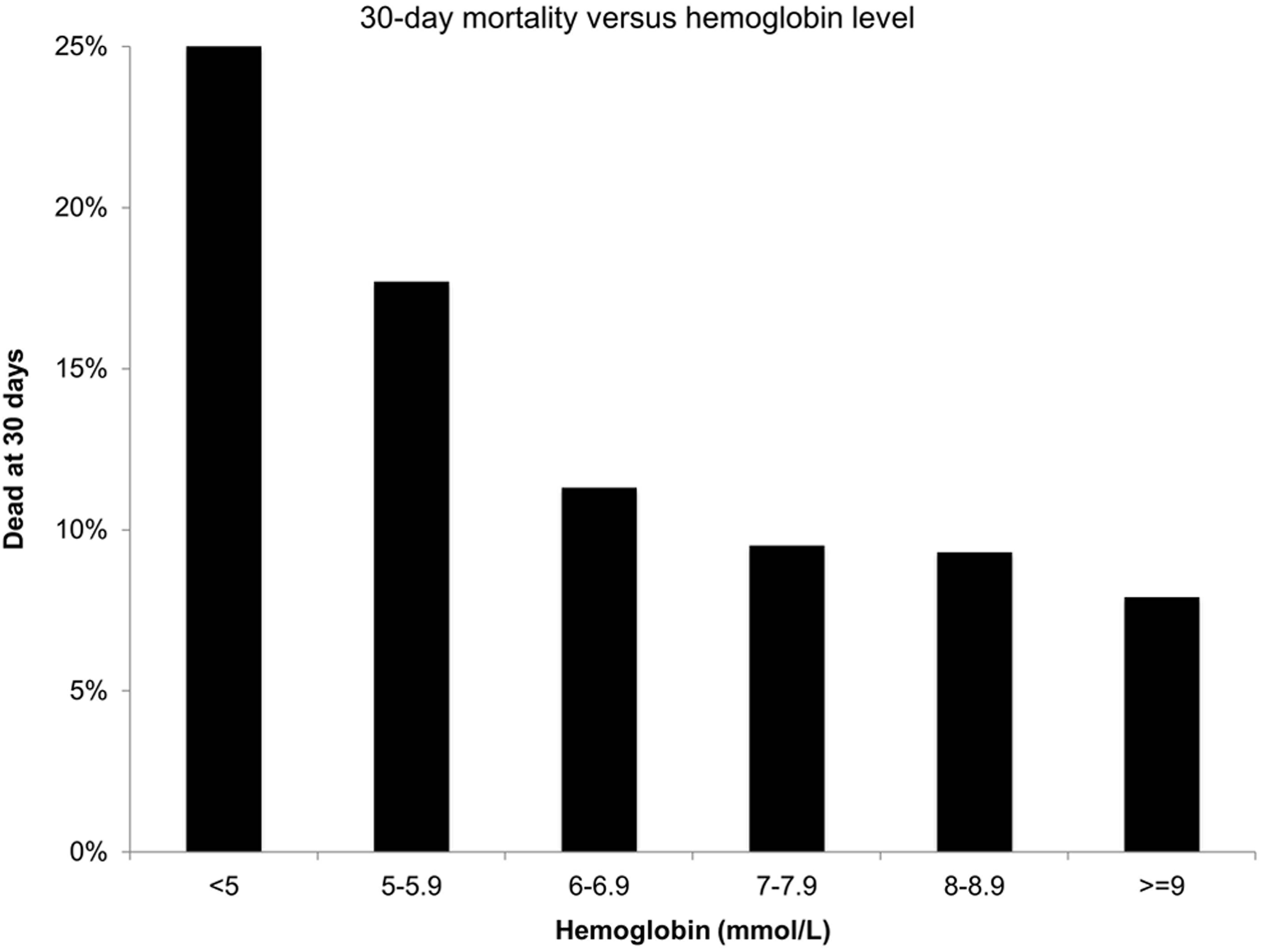
The 30-day mortality decreases for every increase in hemoglobin of 1.0 mmol/L in a univariate analysis (P < .0001).
The HR with 95% confidence interval (CI) for 30-day mortality in patients with anemia was 1.65 (CI: 1.43-1.91, P < .0001). Adjusting for age, type of fracture, gender, and comorbidities (CCI) slightly attenuated the risk estimate (HR: 1.21, CI: 1.03-1.41, P = .02; see Figure 3).

Hazard ratios for 30-day mortality determined with Cox proportional hazards models.
Discussion
The excess mortality in patients with hip fractures compared with the general population is well established. 4 –7,9 In fact, the excess mortality is similar to the 1-year mortality observed for advanced colon cancer. 17,18 Different factors have been associated with this high mortality. In this Danish register-based study based on biochemical data from 7319 individuals with hip fractures, we demonstrated an increased mortality in individuals with a hemoglobin measurement below the reference range.
Previous studies 19 –25 have examined the same association between anemia and mortality in patients with hip fracture, and the pooled results show excess mortality in patients with low hemoglobin. 12 However, these studies had a relatively low number of patients (the highest with 552 patients 20 ). In addition, the cutoff values are not uniform, ranging from 6.21 to 8.07 mmol/L. This fact limits the validity of pooling the results. 12
In contrast to this, our study has a relatively large cohort, which gives it a high statistical power. In addition, this study was a single-center study with a single biochemistry testing facility, which minimizes issues with different procedure at different locations.
The factors affecting postoperative mortality can overall be divided into 2 categories: (1) complications derived from preexisting conditions and (2) complications directly associated with the trauma and treatment. To compensate for the first category, we used previously validated methods to adjust for comorbidities. Despite this, it must be noted that the CCI does not take BMI, smoker, alcohol abuse, or the preoperative functional status into account. Several previously published studies have concluded that these have considerable confounding effect on postoperative outcome. 26,27 Unfortunately, these data were not available for the present study.
The second category includes modifiable factors and thereby the opportunity to optimize individual treatment. Studies investigating these factors with specific protocols to optimize outcome show improved walking on discharge, 28 reduced hospitalization time, 29,30 and significant reductions in the 30-day mortality. 29
Another important factor is the length of time before surgery. It is known to be very central for the survival of patients with hip fracture. This is demonstrated in a study from 2005 by Moran et al, which shows that increased mortality is associated with a delay in surgery for more than 4 days, 31 and in a study from Denmark, which demonstrates an increased 30-day mortality of 24% with each 24-hour surgical delay. 32 Information about surgical delay was unfortunately not available in this study and has therefore not been taken into account.
Hemoglobin level is another potentially modifiable factor, and the measurement has the advantage of being a stable, easily interpreted, and relatively inexpensive test. Our study clearly shows an increased mortality in patients with low hemoglobin level at admission. Intervention such as transfusion and nutritional therapy might be optimizing interventions. There is considerable disagreement about the benefit of transfusion. One study from 2011 conducted a randomized trial to investigate the benefit of a postoperative liberal transfusion strategy in patients with hip fractures, but they did not prove any benefit. 33 In addition, many side effects are linked to blood transfusion. 34 Further studies are therefore needed to investigate this possibility. One thing that we can conclude is that with a hemoglobin measurement, at-risk patients can be identified and further interventions can be instituted.
Conclusion
This study demonstrates increased 30-day mortality in patients with low hemoglobin, even after adjusting for comorbidities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.