
Abstract
Introduction
The complication of delirium for hip fracture patients is a predictor of mortality. Use of opioid medication increases the incidence of delirium in the pre- and postoperative periods. Regional nerve blocks are effective in managing acute pain for acute hip fractures. This study aims to evaluate the utilization of ED physicians to perform fascia iliaca nerve blocks on hip fracture patients to decrease the incidence of delirium by decreasing usage of opioid medication.
Methods
A quality improvement project for performing regional nerve blocks on patients with femoral neck fractures was implemented during fiscal year 2019. Data was collected retrospectively for frequency of ED nerve block procedures, amount of opioid medication use, and incidence of delirium in patients diagnosed with hip fracture. This data was compared to baseline data to determine success of the intervention.
Results
Utilization of regional nerve blocks in the ED increased from 2% in 2018 to 96% in 2021 and 89% in 2022. Preoperative opioid usage decreased from 38 MMEs to 16.9 and 18 MMEs respectively. Daily average MMEs decreased from 34 to 12.1 and 14 respectively. Postoperative delirium decreased from 6% in 2018 to 0% from 2020 to 2022.
Discussion
ED provider administration of fascia iliaca blocks and follow-up is a novel practice in our region to decrease the adverse effects of opiate use and decrease delirium rates. There was a reduction in length of stay and increased discharge home rate despite the Covid-19 pandemic.
Conclusion
Administration of regional nerve blocks by ED physicians to hip fracture patients presenting to the ED results in a decrease in opioid medication usage. This also results in a decreased delirium rates in the hip fracture patient population.
Keywords
Introduction
According to the American Academy of Orthopedics, more than 300 000 people in the United States suffer a hip fracture every year. Most of these fractures occur in people aged 65 years of age or older who injure themselves in a standing height household fall. Projections currently estimate that annual hip fracture nationwide will increase to over 500 000 by 2040. 1 Delirium is one of the most common complications after hip fracture surgery, with estimates ranging from 4-53%.2–4 In patients with delirium, delirium has been found to be an independent predictor of 6 month mortality.5–10 Delirium is a sudden change in mental status characterized by confusion, disorientation, altered states of consciousness (from hyper alert to unarousable), an inability to focus, and sometimes hallucinations. This change in mental status is not one which is better accounted for by a preexisting, established, or evolving dementia. Delirium assessments focus on four cardinal delirium features: acute onset and fluctuating course, inattention, disorganized thinking, and altered level of consciousness. A diagnosis of delirium requires that both the first and second criteria are present, and either the third or fourth. 11
Drugs have long been associated with the development of delirium in the elderly. While delirium is a multi-factorial process, the risk of inducing delirium by medications is high in the frail elderly, and those with dementia. 12 As humans age, changes in receptor function occur across organs. The net effect of these changes is increased drug sensitivity and heightened sensitivity of the brain to adverse drug effects in the frail elderly. Many drugs have been associated with delirium but certain classes of drugs are commonly viewed as being a causative agent for delirium. High dose narcotics are included among those drugs most commonly linked to delirium. It is estimated that medications alone may account for 12%-39% of all cases of delirium.13–15
Hip fracture patients are at increased risk of delirium due to severe pain experienced upon arrival at the emergency department. 16 Regional nerve blocks, specifically fascia iliaca blocks, have been shown to be safe and effective in managing acute hip fracture pain in geriatric patients, leading to decreased opioid use, 17 and a reduction in hospital acquired delirium. 18 The American Academy of Orthopedics, in their 2021 Clinical Practice Guidelines, “Management of Hip Fractures in Older Adults”, recommends the use of preoperative nerve blocks to treat pain after hip fracture. 19 Earlier literature supported the effectiveness of regional anesthesia by anesthesiologists. 20 More recent studies have shown that emergency providers as well as resident physicians can safely and capably perform fascia iliaca blocks in the Emergency Department.21,22
Methods
The hip fracture complication rate at a 219 bed public owned community hospital located in central Oklahoma had increased from 12% in fiscal year 2017 to a six year high of 17% by the end of fiscal year 2018. The Joint Commission Certified Center of Excellence hip fracture care program at this facility admits an average of 280 patients yearly, 69% female and 96% Caucasian, with an average age of 78 years old. 87% of the hip fracture patients resided at home or in an independent living facility prior to their admission. For approximately 89% of the patients, it was their first hip fracture. An analysis of the complications in 2018 showed that 25% of the complications, 6% of the total hip fracture population, were determined to be due to hospital acquired delirium. In the patients who developed delirium, the average time to surgery was 24 hours. Despite timely surgery, 45% of the patients with delirium developed the delirium prior to surgery. In the patients who developed delirium, it was noted that the patients demonstrated poorly managed pain prior to surgery as evidenced by the increased average opioid administration per patient.
Utilizing retrospective chart review, it was determined that the hip fracture patient population received an average of 38 morphine milligram equivalence (MME) prior to surgery. A literature review provided consistent evidence that the fascia iliaca regional nerve block can be administered in the emergency department (ED) setting to reduce pain associated with hip fracture by providing rapid onset, site specific analgesia that is more effective than standard systemic analgesia alone. 23 We hypothesized that utilizing ED physicians and residents to provide fascia iliaca blocks to our hip fracture patients in the ED would reduce the rate of hospital acquired delirium by decreasing the amount of opioids required to manage pain prior to surgery.
A multidisciplinary quality improvement committee responsible for the operation and management of the orthopedic surgery program was tasked to evaluate and identify opportunities to improve pain management between the time of admission and time of surgery, without increasing the amount of systemic opioids given to hip fracture patients. This quality improvement project was approved by the IRB with exempt status.
The initiative providing fascia iliaca blocks in the Emergency Department for pain relief in acute hip fracture patients was launched in fiscal year 2019. All patients diagnosed with an acute (less than 24 hours) hip fracture presenting to the ED would be eligible for a fascia iliaca block once x-ray confirmed a femoral neck, intertrochanteric or subtrochanteric fracture. Contraindications to a fascia iliaca block for a hip fracture included: known allergy or anaphylaxis to local anesthetic, open fracture, cellulitis at injection site, anticoagulation with warfarin or a Xa inhibitor, or an abnormal neurovascular exam of the affected extremity. In addition to contraindications, patients would be excluded from receiving this intervention due to patient refusal, inability to provide consent or being sent directly to Operating Room (OR) from the Emergency Department. Pain blocks were performed on all appropriate patients regardless of age, sex, or socioeconomic factors.
An ED physician or resident trained in fascia iliaca block would assess the patient and then perform a pre-procedural neurovascular exam on the affected extremity. The femoral artery, vein, nerve, and fascia iliaca are identified using ultrasound at the level of the common femoral artery. The area is then sterilized with chlorhexidine. A sterile ultrasound probe cover is placed on the ultrasound. A sonoblock needle is advanced under ultrasound guidance in-plane to the fascia iliaca plane. A weight based dose of .5% ropivicaine is calculated using the SafeLocal app. The ropivicaine is mixed with 10-20 mL of sterile saline to increase volume and is injected into the fascia iliaca plane.
Data collection was completed by orthopedic department staff and entered into a contracted data storage and analysis system based upon CMS quality reporting, daily chart audits, and retroactive chart review. The first performance measure examined was the percentage of patients who received a fascia iliaca pain block in the ED. The second performance measure examined was the calculation of the average MME given prior to surgery as well as the average daily MME given prior to surgery to the hip fracture patients. Average MME and average daily MME were calculated using the Opioid Oral Morphine Milligram Equivalent (MME) Conversion Factors table for prescription drug coverage by the U.S. Department of Health and Human Services. The incidence of delirium was tabulated as hip fracture patients with a secondary diagnosis of delirium and with an accompanying status of not present upon admission. Delirium complications at any coding depth were included. This diagnosis is determined by multi-disciplinary delirium assessments documented in the patient record, such as: nursing performing the confusion assessment method (CAM) every shift, speech therapy performing a cognitive assessment and monitoring of each patient and attending hospitalist rounding daily (orthopedics is a consult service). Delirium was recorded and defined using the confusion and assessment method on any day or night of their hospital stay, whether before or after surgery.
Results
Primary Outcomes
Hip Fracture Delirium Outcome Measures by Fiscal Year, 2018-2022.

The outcome measure utilized to determine successful implementation was defined as the incidence of delirium in the patient population with an acute hip fracture diagnosis. The overall hospital acquired delirium rate baseline dropped by 50% every year. The overall hospital acquired delirium rate at baseline in 2018 was 6%. The rate of hospital acquired delirium decreased yearly resulting in a rate of 0% in 2021. There was one case of hospital acquired delirium in 2022 resulting in a rate of .5%. Hospital acquired delirium diagnosed prior to surgery was 3.7% at baseline in 2018, and has been eliminated in our hip fracture population since 2020. Provider staffing, patient care protocols prior to surgery, and hip fracture hospitalization order sets did not change during this time.
Patient Population Demographics.

Secondary Outcomes
In addition to the primary outcome measures, there were secondary outcome findings related to the implementation of the ED nerve block program for hip fracture patients that were not anticipated. Patients who received a pain block in the ED were less likely to develop delirium when compared to patients who did not receive a pain block in the ED (Figure 1). The hip fracture discharge to home rate has doubled to 33% (Figure 2). The average length of stay for patients who had an ED administered nerve block averaged 18 hours less in 2022 when compared to patients who did not receive a nerve block (Figure 3). The hip fracture discharge to home rate has doubled to 33% (Figure 2). Delirium rate comparison for patients who received ED nerve block and patients who did not. Hip fracture average length of stay FY 2018-2022. Percentage of hip fracture patient population discharged home.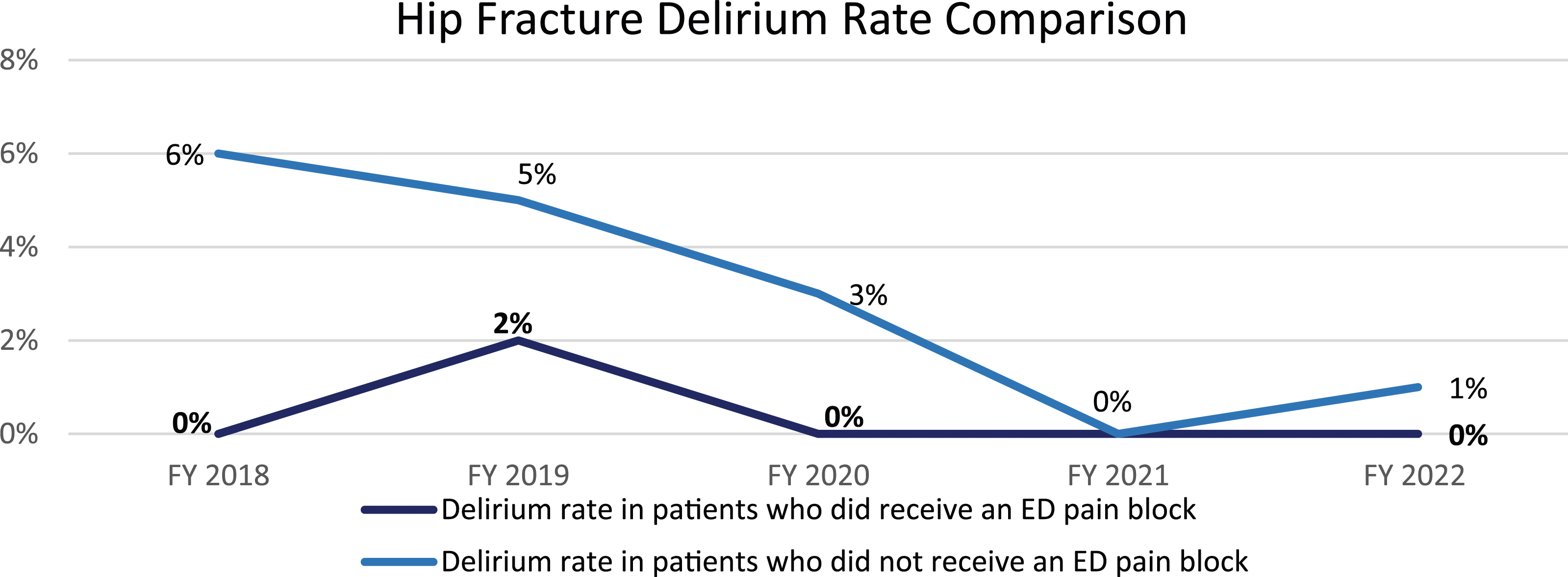


Limitations
The development of postoperative delirium is multifactorial and this study is limited due to the fact that factors such as age, socioeconomic status, and comorbidities are not taken into effect. The retrospective analysis of the data also presents the opportunity for selection bias. However with regards to this study, all patients that received the regional hip block procedure presenting to the ED were included in the patient population for study.
Discussion
While there are foreign research articles on junior doctors performing fascia iliaca blocks for pain management with hip fracture patients, ED providers and residents utilizing fascia iliaca blocks is a novel approach in our region.
Within our system, ED physicians are empowered to make the decision to utilize a fascia iliaca block prior to orthopedic consultation once a hip fracture has been diagnosed by x-ray. During the initial discussions which occurred prior to implementation of this project; the anesthesiology department voiced concerns regarding a lack of follow up by ED physicians once patients are admitted. This was addressed by the ED providers agreeing to re-assess the patient on the unit as needed for complications or any other needs related to the fascia iliaca block.
The adverse effects of high doses of opioids, especially in the elderly, have been well documented. Common side effects to opioids include: sedation, cognitive impairment, respiratory depression, urinary retention, nausea, and constipation.2 2224 During this initiative, MMEs prior to surgery and daily average MME’s prior to surgery have both been reduced by over 50%. Our final results of average 18 MME prior to surgery and daily average MME of 14 are similar to the results of 17.4 MME prior to surgery and daily average MME of 13.3 found by Kolodychuk. 25 Accompanying the reduction of the average MME dose was a corresponding drop in the hospital acquired delirium rate. Hospital acquired delirium has been decreased by 90% and hospital acquired delirium prior to surgery has not been recorded in the last 3 years. Hospital acquired delirium was last recorded in a patient who received a fascia iliaca block in the ED in FY 2019. Hospital acquired delirium in hip fracture patients has been associated with poorer outcomes, including increased length of stay. 5
Recent research has also shown a correlation to the Covid-19 pandemic and a decreased length of stay for hip fracture patients.2 2226 Our reduction in overall average length of stay from 5.3 to 4.5 was consistent with, though not quite as significant as that noted in this research. Mitigating the effects of the Covid-19 pandemic is a direct comparison of the length of stay in hip fracture patients who received the fascia iliaca block vs hip fracture patients who did not receive a fascia iliaca block. On average, the length of stay was .5 days shorter in hip fracture patients who did receive a fascia iliac block vs those that did not. The greatest difference was recorded in FY 2022 when hip fracture patients who received a fascia iliaca block had a length of stay .8 days shorter compared to hip fracture patients who did not receive a fascia iliac block. While the percentage of hip fracture patients discharged home was no doubt influenced by the Covid-19 pandemic, the increased percentage of hip fracture patients discharged home did remain increased prior to and after the high point of the Covid-19 pandemic in our region.
Conclusion
Fascia iliaca blocks performed by emergency department providers on patients who present to the emergency department with an acute hip fracture can lead to reduced opiate usage prior to surgery. The reduction in opiate usage has also proven successful in decreasing the percentage of hip fracture patients who experience the complication of hospital acquired delirium. Utilization of the fascia iliaca block procedure can also positively impact length of stay and discharge home rate of the hip fracture patient population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.