
Abstract
Background:
Delirium in elderly orthopaedic patients poses an enormous medical, social and financial burden to the healthcare system, and causes significant distress to patients and their caregivers. We examined whether a Multi-component Care Bundle (MCB) could reduce the incidence of post-operative delirium (POD) in fractured hip patients.
Methods:
An observational study was conducted, analyzing 154 patients (mean age ± SD, 85 ± 7.8, 68% women) admitted to Queen Mary Hospital with hip fracture. Half of the patients were cared for in the control group before MCB was introduced, which included installation of orientation aids, introduction of a Caregiver Empowerment Program, and incorporation of ultrasound-guided Fascia Iliaca Block (FIB) into the analgesia protocol.
Results:
There were fewer patients with POD in the MCB group, compared with the control group (18/76, 23.4% v 34/76, 44.2%, p = 0.006). Patients in MCB group consumed less opioid ( 4/77 v 13/77, p = 0.048), experienced less post-operative dizziness (2/77, 2.6% v 13/77, 16.9%, p = 0.003) and had a shorter median day to start walking post-operatively (day 1 [IQR 1-2] vs day 2 [IQR 2-3]; p = 0.001) than the control group. Length of stay was not affected.
Conclusion:
MCB effectively reduces POD, postoperative dizziness, opioid consumption, and days to start mobilization postoperatively.
Keywords
Introduction
Most hip fracture patients need to be managed surgically followed by early mobilization in order to minimize complications such as deep vein thrombosis, pulmonary embolism, pneumonia and bed sore. Traditionally, post-operative mortality is about 8% at 1 month and 30% at 1 year. 1,2 Only one-third of patients return to their baseline premorbid functional level. 3 -5
Post-operative delirium (POD) is a common complication in these patients with a reported incidence of 70%. 6 POD is associated with increased mortality, increased length of stay and in the long-term, limitation in basic activities of daily living, increased level of dependency and increased risk of dementia.
The exact mechanism of POD is unknown, but it is hypothesized that peripheral inflammation from trauma and surgery is linked to neuroinflammation and neuronal injury. Imbalance between cholinergic and dopaminergic activity, ischemic brain injury and a breakdown of blood-brain barrier may each play a role in the development of POD. 7
Recommendations on management of POD include early diagnosis, correcting metabolic or physiological derangement, avoiding polypharmacy, minimizing use of lines, catheters and physical restraints, maintaining good sleep hygiene and providing adequate analgesic in addition to cognitive and sensory aids for re-orientation. 8
The aim of this study is to examine whether a multi-component care bundle (MCB) could reduce the incidence of POD in fractured hip patients.
Methods
This was a cross-sectional observational study. Data was collected from all patients admitted to the Department of Orthopaedics and Traumatology of Queen Mary Hospital for fractured hip since the introduction of MCB in July 2019 and was compared to historical controls who received care under the conventional fracture hip pathway. The data had either been routinely collected for auditing purpose or retrieved from the hospital computer-record system.
Patients younger than 65 years old, refused operation, did not require operation, had pathological fracture or old fracture (attended more than 48hours after fall) were excluded from both the MCB and control groups.
We followed up these patients and collected clinical data daily till post-operative day 5.
The primary outcome was the incidence of POD as measured by short Confusion Assessment Method (short CAM), which was used by trained nursing staff to assess delirium daily till post-operative day 5. Delirium detected by the short CAM on any day during the follow up is considered positive, regardless of the duration.
Secondary outcomes were pain at rest and during movement as measured by NRS (rest) and NRS (movement) respectively, use of additional analgesia, adverse reactions to opioid, incidence of block complications, days to start walking, postoperative complications and total length of stay.
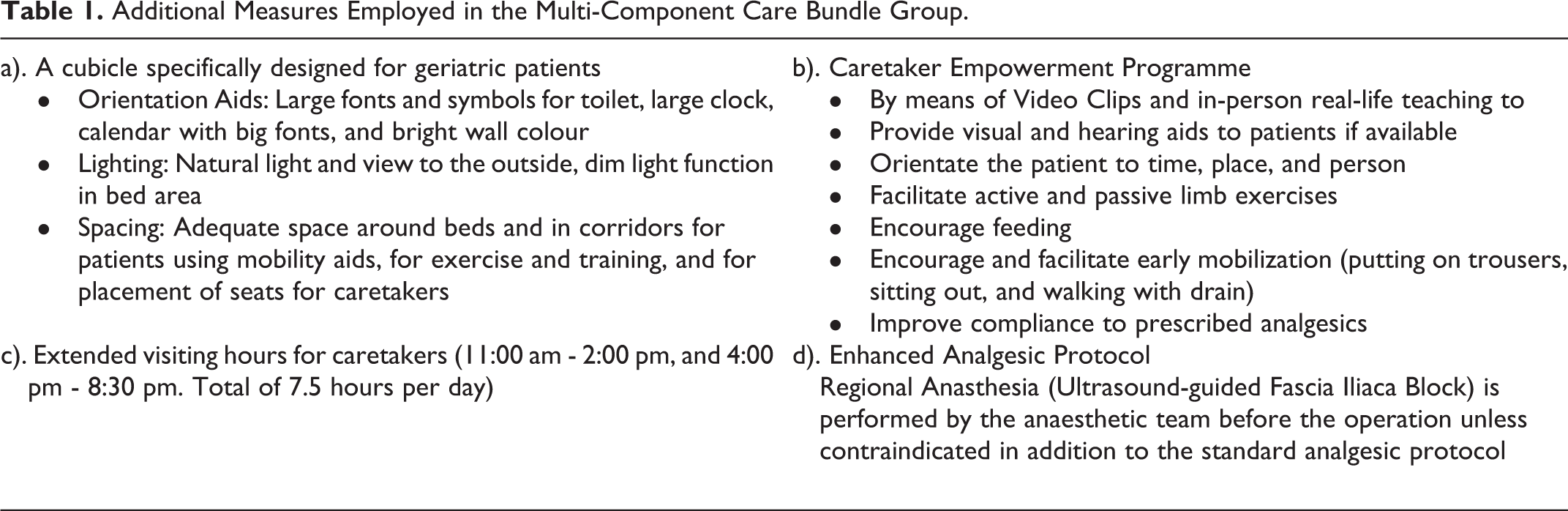
In addition to routine care, the MCB encompassed the installation of Orientation Aids, the incorporation of a Caretaker Empowerment Program, and an Enhanced Analgesic Protocol. (Table 1)
Additional Measures Employed in the Multi-Component Care Bundle Group.
Sample size was calculated based on a reported reduction in POD from 62.4% to 43.3% from previous trials (Marcantonio 2001, Lundstrom 2007). A total of 208 patients (104 in the control group and 104 in the MCB group) were required for a study power of 80% and a p value < 0.05. All analyses were performed based on intention-to-treat using SPSS version 21.0 software.
Results
A total of 154 patients were included in the observational study between July 2019 and July 2020. 200 patients were screened for eligibility, 7 were deemed ineligible and 39 were excluded to ensure equal sized groups. Half of the enrolled 154 patients were operated on and cared for in the control group (n = 77) and half were in MCB group (n = 77).
Baseline Demographics
The baseline characteristics were similar between the 2 groups (Table 2). The mean age, gender and place of residence were consistent with the nationwide demographics of hip-fracture non-participants [3]. The mean age was 84.8 (SD 7.8) in the control group and 85.7 (SD 7.9) in the MCB group. There were 48 (31%) men and 106 (69%) women in total. There was no statistically significant differences (p < 0.05) in any of the baseline characteristics examined apart from in the predicted functional status. More patients in the MCB group (63.5%) were predicted to require maximum assistance or become fully dependent, compared to 36 (48%) patients in the control group. These predictions came from an objective assessment, the modified Barthel Index, performed by occupational therapists. The control group had more bed/chair-bound patients but these differences were not statistically significant (p = 0.258).
Baseline Characteristics.a

Abbreviation: T, trend test.
a Data are Mean (SD), n (%), or Median (IQR).
b Significantly different between the 2 groups at 0.05 level.
Pre-Operative and Intra-Operative Management
Pre-operative fascia iliaca block (FIB) were administered to 69 (92%) patients in the MCB group and to none in the control group (p = <0.001) (Table 3). Spinal anesthesia was the more frequently chosen mode of anesthesia in both groups, with 84.4% in the control group and 78.7% of the MCB group.
Intra-Operation Measures.a

a Values in % (n) or % (n/total).
b Significantly different between the 2 groups at 0.05 level.
Primary Outcome Measures
There was a statistically significantly higher incidence of POD in the control group compared with the MCB group (34/76 (44.2%) vs 18/76 (23.4%), p = 0.006, relative risk (RR) = 1.89, CI 1.17-3.04). The odds ratio was 2.59 (95% CI 1.30-5.18) which implies patients in the control group are 2.59 times more likely to develop POD than those in the MCB group. Table 4 shows the prevalence of pre-operative delirium was also higher in the control group (15.8%) than the MCB group (3.9%). The rise in POD was higher in the control group, with an additional 22 patients (rise of 28.4%) compared to the MCB group rise of 15 patients (rise of 19.5%).
Primary outcomes.a
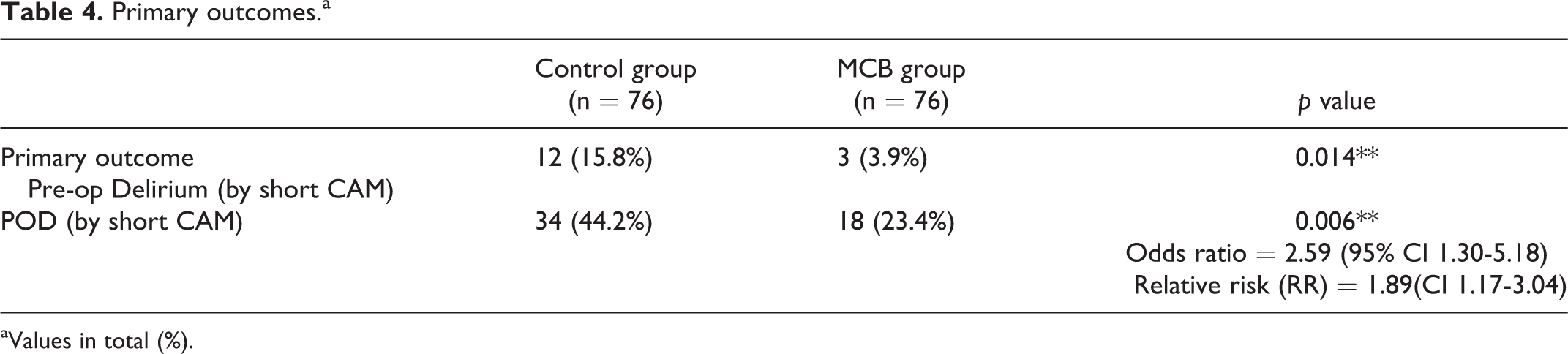
aValues in total (%).
Secondary Outcomes
There were fewer episodes of post-operative dizziness occurring in the MCB group than the control group (2 [2.6%] vs 13 [16.9%]; p = 0.003) . Patients in MCB group were faster to mobilize than those in control group (day 1 [IQR 1-2] vs day 2 [IQR 2-3]; p = 0.001; Table 9). More patients in MCB group were judged to have fair rehabilitation potential (64/77 vs 52/77, p = 0.041) compared to the control group. However the control group had more patients judged to have a good rehabilitation potential compared to the MCB group (17/77 vs 8/77). These rehabilitation potentials were assessed subjectively by a physiotherapist. The MBI score was hugely varied in both groups in the post-operative period, which were not statistically significant.
There was no difference in pain scores in non-delirious patients . Fewer patients in the MCB group needed other opioids for rescue such as tramadol or oxycodone (4/77 v 13/77, p = 0.048), which could be attributed to the high rate of FIB performed in this group.
There were more postoperative orthopaedic complications, such as DVT or revision surgery, in the control group (18 [23.4%] patients) than the MCB group (7 [9.2%] patients; p = 0.018). The 3 resulting deaths from this study were all infection-related (biliary sepsis, UTI or pneumonia).
Both groups have similar length of stays. This suggests that once delirium has occurred, multi-factorial interventions do not shorten the length of stay. There were no changes to the discharge destination in either groups (Table 5).
Postoperative Measures.a
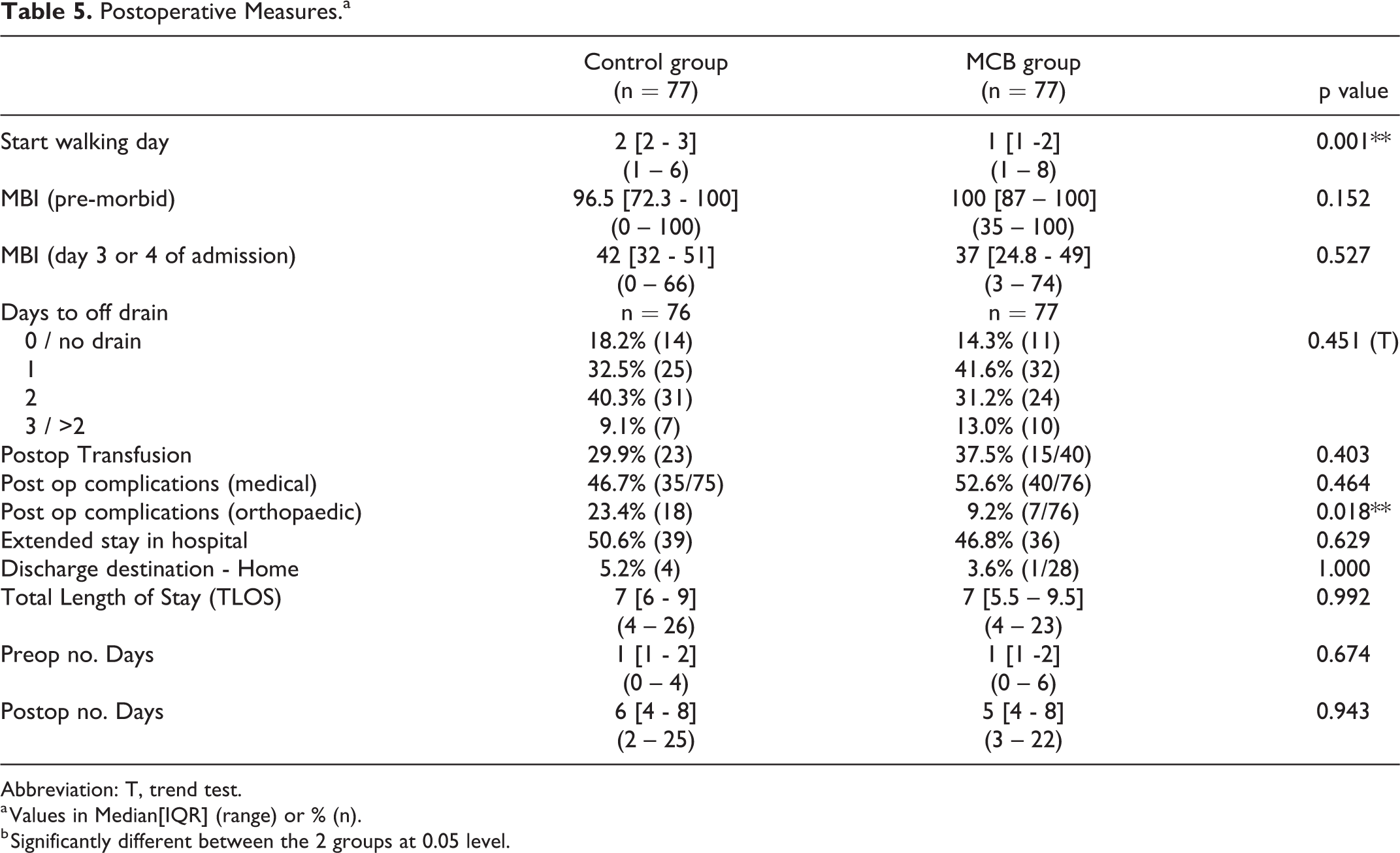
Abbreviation: T, trend test.
a Values in Median[IQR] (range) or % (n).
b Significantly different between the 2 groups at 0.05 level.
Discussion
MCB appears to reduce the risk of POD (OR 2.59), lower risk of post-operative dizziness and shorten start to mobilization compared to control. The median pain scores remained low and were comparable in both groups, but less opioids were consumed in the MCB group. This could be attributed to the higher rate of FIB performed in the MCB group than the control group.
Our observations are in accordance with an earlier randomised controlled trial (Marcantonio 2001) which showed a roughly 1/3 reduction in the incidence of POD in the intervention group. Our control group had 44.2% of POD, which was reduced to 23.4% in the MCB group. Marcantonio et al used specific protocols to address sleep hygiene, immobility, visual and hearing impairment. We have also addressed several of the same factors and achieved similar results.
There was a high rate of delirium pre-operatively in the control group (15.8%), which could be due to inadequate pain control. The control group had high pre-op NRS pain scores during movement and no FIB was given as an opioid-sparing low-risk alternative to other analgesia. The MCB group had 92% FIB rate and demonstrated an earlier walking day, which suggests that FIB does not cause a prolonged motor block or hinder post-operative recovery.
There was an encouraging number of caretakers who visited in the post-operative period in both groups. It is impossible to enforce mandatory caretaker hours during a patient’s hospital recovery but by offering longer visiting hours, this presents an opportunity for the primary caregiver to partake in the multi-component approach of tackling POD. Giving allied health professionals different assessments (both subjective or objective) means that a patient’s progress can be tracked more readily.
Our study was observational. This entailed that the patients did not follow a rigorous study protocol and also has a high risk of confounding bias from ward staff who are all involved in the implementation of a new system, which they are conscious is being audited. Because the control group data was collected first before the MCB was introduced, there can be some reporting bias (which is difficult to adjust for). It was a pragmatic study. Due to the logistical difficulty and limited physical space, it was not possible to have 2 separate wards to conduct a randomized controlled trial. We excluded 39 patients in order to ensure equally matched control and intervention groups, however this reduced our overall sample size and thereby undermined the power of the study.
A major strength of this study is that we used multiple simple and validated tools for diagnosing delirium or assessing functionality such as the short CAM or modified Barthel index. We carried out the short CAM score both pre-operative and post-operative as it is important to recognize that it is not just the operation and surgical stress response which contribute to delirium, but that these patients may already be brought into hospital confused from home.
Conclusion
The installation of Orientation Aids, introduction of Caretaker Empowerment Program, and incorporation of pre-operative FIB into the analgesic protocol are key elements of the MCB, which has been shown to effectively reduce POD in patients with hip fracture.
MCB group also demonstrated less opioid analgesic used, less postoperative dizziness and an earlier start to mobilization despite being predicted to be more functionally dependent postoperatively.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.