
Abstract
Introduction
Though hip fractures are associated with significant mortality and morbidity, increasing life expectancy in developed countries necessitates an analysis of mortality trends and factors predicting long term survival. The aim of this study is to identify the predictors of 10-year mortality as well as assess the correlation of Age-adjusted Charlson comorbidity index (ACCI) with 10-year mortality in a surgically treated Asian geriatric hip fracture population.
Materials and Methods
From January 1, 2007 to December 31, 2009, 766 patients who underwent surgery for hip fracture with a minimum follow up of 10-years were recruited to the study (92% follow-up rate). A review of the patient’s electronic hospital records was performed to glean the following data: patient demographics, pre-existing comorbidities, operation duration, length of stay, fracture configuration, as well as mortality data up to 10 years. CCI scores and individual co-morbidities were correlated with inpatient, 30-day, 1-year, 5-year and beyond 10-year mortality.
Results
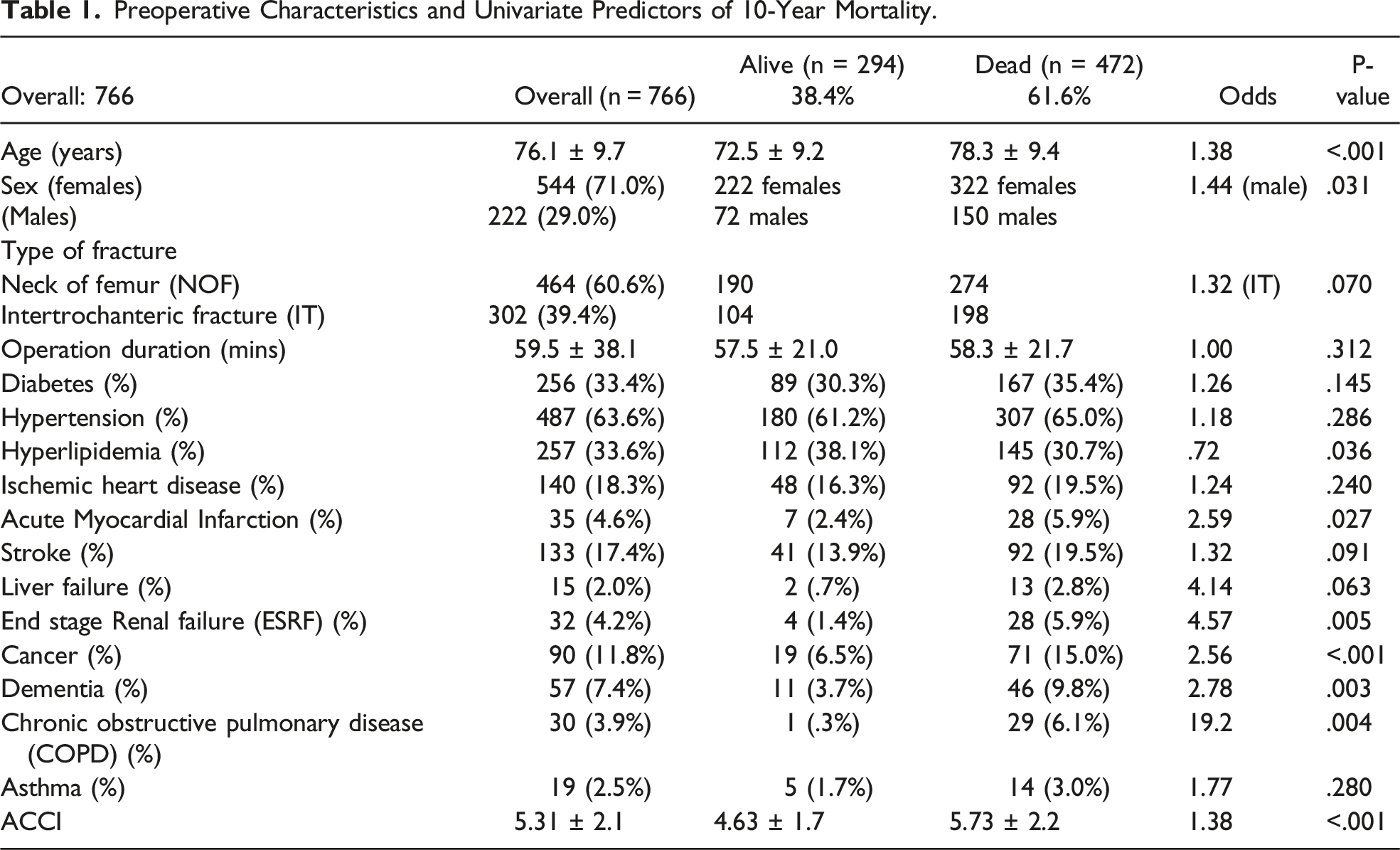
Of the 766 patients, the mortality rate for 30-day, 1-year, 5-year and 10-years was 2.9%, 12.0%, 38.9% and 61.6% respectively. The average ACCI was 5.31. The 10-year mortality for patients with ACCI ≤ 3, ACCI 4-5 and ACCI ≥ 6 are 29.4%, 57.4% and 77.5% respectively. End-Stage-Renal Failure (ESRF), liver failure and COPD were dominant predictors of mortality at 10 years, whereas cancer was the predominant predictor at 1 year.
Discussion
ACCI significantly correlates with the 10-year mortality after surgically treated hip fractures with a shift of the dominant predictors from cancer to ESRF and COPD. This could inform future health policy and resource planning. This data also represents recently available pre-pandemic survival trends after hip fracture surgery and serves as a baseline for post-pandemic outcome surveillance of interventions for fragility fractures.
Conclusion
This study demonstrates that ACCI correlated with 10-year mortality after surgical treatment of hip fractures.
Introduction
The rising incidence of hip fractures in the elderly coupled with the increasing life expectancy of the population has led to an increased burden on healthcare, especially in the Asian population. 1 By 2050, the percentage of the population aged older than 60 years old is projected to increase to 38%,2,3 with the Asia-Pacific region projected to be the most rapidly aging population in the world over the next 20 years. 4 Longevity is itself a marker of first world economic developments and advances in healthcare but brings with it new challenges in terms of disability associated with fragility fractures, of which hip fractures are one. Osteoporotic hip fractures are known associations with increased mortality and morbidity.
There is a paucity of literature evaluating the effect of comorbid diseases and other determinants of mid- to long-term mortality of patients who underwent surgery for osteoporotic hip fractures. Guzon-illescas et al studied 3992 patients with osteoporotic hip fracture over a 17-year period and identified the risk factors such as COPD, age over 75 years old, Charlson index >2, and congestive cardiac failure among many others. However, it did not study the mortality rate for surgically treated patients, which is the recommended management for the majority of patients currently. 5
While previously 20-35% of patients sustaining a hip fracture die within a year,6,7 survivorship after hip fractures has increased over the past decade. 8 Shifts in mortality trends with better peri-operative care and surgical intervention necessitates a re-look at current determinants of long-term mortality in surgically treated hip fracture patients. With the advent of Covid-19, mortality trends and excess mortality may have shifted. This study, which documents 10-year survivorship up to 2019 (which corresponds with the end of the pre-Covid period), forms an important baseline for comparison with post-Covid survival trends.
The authors hypothesize that patients with a higher ACCI are correlated with a higher risk of 10-year mortality. The aim of this study is to assess the correlation of the Age-adjusted CCI (ACCI) with 10-year mortality in a surgically treated Asian geriatric hip fracture population and compare the time to event between patients with varying ACCIs. A secondary aim is to determine co-morbidities which independently predict 10-year survivorship.
Materials and Methods
Our study was approved by the hospital’s ethics committee and carried out in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
From January 1, 2007, to December 31, 2009, 766 patients who underwent surgery for a unilateral, isolated hip fracture sustained after a fall from standing height with a minimum follow up of 10-years were included in the study (92% follow-up rate). Patients who suffered a high-energy mechanism of injury, polytrauma, pathological fractures and atypical femoral fractures were excluded from the study. All patients in this study were followed up for 10 years.
A retrospective analysis was performed on these patients and a review of the patient’s electronic hospital records were performed to glean the following data: patient demographics, pre-existing comorbidities, as well as inpatient, 30-day, 1-year, 5-year and beyond 10-year mortality data.
Individual co-morbid conditions were collected from available medical records. The Charlson comorbidity index (CCI) is the most widely used comorbidity index to predict mortality. 9 The CCI has also been adapted and modified to adjust for age as an additional variable as they found that every decade of age correlated with 1 comorbidity value. 10 Many studies have found that CCI is a strong predictor of 30-day, 1-year, 11 5-year mortality in hip fracture patients. 12 In this study, CCI scores were calculated using the data from pre-existing comorbidities and age-adjusted for this study. Age-adjusted CCI (ACCI) were further classified into ACCI category 1, 2, and 3 with an ACCI score of 0 to 3, 4 to 5, and 6 and above, respectively.
Statistical Analysis
Continuous data have been summarized by mean (standard deviation) or median (interquartile range) as appropriate and categorical data by frequency (%). The Mann- Whitney test or t test was used to evaluate differences in continuous predictors between the groups. The x2 test and Fisher exact test were used to evaluate associations between the primary outcome and categorical predictors of interest. Univariate logistic regression was used to assess the relationship between the outcome and the predictors of interest. A multiple logistic regression model was constructed to include the statistically and clinically significant predictors. Kaplan-Meier curves were plotted to assess the differences in 10-year mortality with respect to different categorical predictors of interest. The log-rank test was used to test for difference in survival. The Cox proportional hazards model was used to assess the relationship between 1,5 and 10-year survival and different predictors of interest.
Results
Preoperative Characteristics and Univariate Predictors of 10-Year Mortality.
Hazard Ratios of Predictors Over Varying Time Periods.
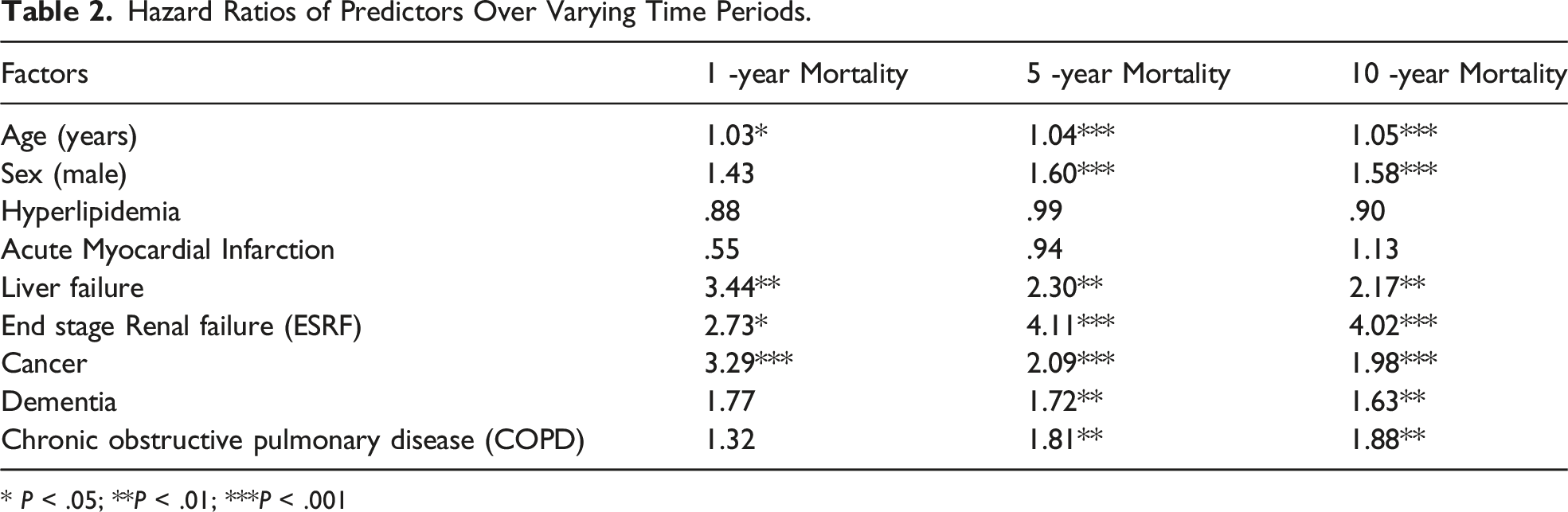
* P < .05; **P < .01; ***P < .001
Multiple Regression Model Using Gender and ACCI as Predictors of 10-Year Mortality.

30-Day, 1-Year, 5-Year and 10-Year Mortality Rates for Patients in varying ACCI Categories.


Kaplan-Meier survival curves of patients in the different age adjusted Charlson comorbidity index (ACCI) categories: ACCI category1: ACCI 3 and below; ACCI category 2: ACCI 4 to 5; and ACCI category 3: ACCI 6 and above.
A comparison of the predictors for mortality over time showed that Age and Gender remained fairly constant at around 1 (HR: 1.03-1.05) and 1.5 (HR: 1.43 – 1.60) respectively. Cancer however, decreased over time from HR 3.29 to 1.98. (Table 2)
Discussion
The 10-year mortality rate of 61.5% after hip fracture surgery was similar to other published studies. In a Finnish study, Tiihonen et al. evaluated 490 hip fracture patients over a 10-year follow-up and reported a 79.8% mortality. 14 In an American study, Nader et al. reported a slightly lower mortality at 75.3% in a cohort of 1109 patients. 15 Another Asian study found that the 5 and 10-year mortality data was 55 and 68% respectively. 16 The mortality rate reflects the high mortality burden of hip fractures, and the slight variation could be explained by regional variations in treatment of hip fractures, differing population demographics, comorbidities and social habits such as smoking, alcohol-consumption and recreational drug use.
For example, the smoking rate in Singapore is 16.5%, which is significantly lower than in the United States (25.1%) and slightly lower than in Finland (19.1%). 17 Similarly, on average, Singaporeans consume 2L of alcohol per year, in contrast to 9.97 L/yr in the United States and 10.65 L/yr in Finland. 18 According to a WHO report, Singapore had a 1.1 score on the Disability-Adjusted Life Years (DALYs) scale, which represent the number of healthy years of life lost to the use of illicit drugs, averaged across the country's entire population. In contrast, United States scored 6.7 and Finland scored a 3.3. 19 This is largely due to Singapore’s zero drug tolerance policy.
Although increased mortality after hip fractures could reasonably be attributed to the multi-morbidity of a hip fracture cohort, Liow et al found that excess mortality risk is conferred by a hip fracture and continues to persist 9 years post fracture, even after adjustment for comorbidity. 20 Similarly, a Singapore Chinese Health study by Koh et al found that after adjusting for comorbidities and risk factors, hip fractures cases had a higher all-cause mortality when compared to non-fracture cases. This excess mortality risk persisted after 5 years and was contributed by pneumonia, urinary traction infection and heart disease. 21
In similarity, our multi-ethnic Asian cohort of minimum 10-year follow-up showed that ACCI strongly correlates with mortality after surgical treatment of hip fractures. Patients with a high ACCI score ≥ 4 had a 3.79 to 9.37 times higher risk of mortality at 10 years post index surgery. We found that a cumulative index of comorbidities such as the ACCI is a more reliable predictor than individual comorbidities. These finding echoes that of a study by Jiang et al. who found that ACCI correlated with the 5-year mortality in surgically treated hip fracture patients but that individual comorbidities may not be as significant in their impact.22 Our study establishes that ACCI not only correlates with the 5-year mortality but correlates with the 10-year mortality as well.
When comparing the predictors of mortality over time, our study found that Age and Gender remained fairly constant throughout the years while cancer decreased over time. ESRF and COPD have shown to be progressively stronger predictors of mortality over time. Our study showed that COPD was found to be the strongest predictor of 10-year mortality (OR = 19.2) with ESRF trailing behind (OR = 4.57). This is consistent with a published paper that reported a 60-70% higher risk of death following hip fracture surgery with COPD than those without COPD. 23 However, the exact mechanism substantiating the association is unclear. The speculated reason behind this is that COPD not only affects multiple organ systems but has a huge burden on the patient in terms of mobility as these patients commonly experience shortness of breath on exertion. Cohorts of patients with COPD and ESRF without hip fractures have 5-year mortality rates at 25.4% 24 and 39.8% respectively. 25 While these values may be similar to our 5-year mortality rates, no direct comparison can be made with our study as the two groups differ in terms of demographics or disease severity. Nevertheless, COPD and ESRF have a high impact on mortality and morbidity, hip fracture or not.
These findings reflect the shifting importance of comorbidities on mortality along the lifespan of the patient. Those patients with cancer who are amenable to treatment are able to bring their survival curves back to that of the normal population whilst others with ESRF or COPD continue to be impacted by the disease burden. Cancer appears to impact early survival but not long-term survival. The authors of this study hypothesized that those with advanced cancer would have perished early in the follow-up. Patients with earlier stages of cancer responsive to treatment are likely to survive the subsequent years, and this will decrease the hazard ratio of cancer on long-term mortality.
In contrast to patients with higher co-morbidity, the mortality rates of CCI<3 at 29.4% is comparable to the 1-year mortality of earlier studies of hip fractures. Future analysis of hip fractures could take the ACCI into consideration as it is apparent the physiological fitness of this elderly cohort is distinctively different among subgroups with differing co-morbid burdens. The robust long-term survivorship implies prosthesis longevity, function and quality of life indices are important considerations in the management of a fitter cohort of patients undergoing hip fracture surgery.
Conversely, low energy hip fractures significantly impact long term survivorship in patients with CCI ≥ 4. Often overlooked due to polypharmacy, osteoporosis treatment for primary prevention is even more important in this cohort. In particular, future efforts could also be made to understand the impact of co-morbidity burdens such as COPD and ESRF to improve long term function and survivorship. This cohort also represents the most recent available long term survival data of a cohort of surgically treated hip fracture patients just before the onset of the Covid pandemic and forms the basis for comparison with future mortality trends. Though distinct from COPD, potential impacts of Covid on respiratory function could also impact outcome and survivorship of hip fracture patients post pandemic.
The Strength of this study is that it has a high follow-up rate 92% with a minimum of 10-year follow-up. To the authors' knowledge, there are very few or no published studies validating the use of ACCI in predicting 10-year mortality. The limitations of our study are that CCI does not allow for risk stratification based on disease severity. 26 For instance, a patient with a high CCI can have multiple comorbidities that are well-controlled resulting in a fairly good outcome.
Conclusion
ACCI significantly correlates with the 10-year mortality after surgically treated hip fractures with a shift of the dominant predictors from cancer to ESRF and COPD. This could inform future health policy and resource planning. This data also represents recently available pre-pandemic survival trends after hip fracture surgery and serves as a baseline for post-pandemic outcome surveillance of interventions for fragility fractures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.