
Abstract
Introduction
The associated mortality and morbidity in hip fracture patients pose a major healthcare burden for ageing populations worldwide. We aim to analyse how an individual’s comorbidity profile based on age-adjusted Charlson Comorbidity Index (CCI) may impact on functional outcomes and 90-day readmission rates after hip fracture surgery.
Materials and Methods
Surgically treated hip fracture patients between 2013 and 2016 were followed up for 1-year and assessed using Parker Mobility Score (PMS), EuroQol-5D (EQ-5D) and Physical and Mental Component Scores (PCS and MCS, respectively) of Short Form-36 (SF-36). Statistical analysis was done by categorising 444 patients into three groups based on their CCI: (1) CCI 0–3, (2) CCI 4–5 and (3) CCI ≥ 6.
Results
PMS, EQ-5D and SF-36 PCS were significantly different amongst the CCI groups pre-operatively and post-operatively at 3, 6 and 12 months (all P < 0.05), with CCI ≥ 6 predicting for poorer outcomes. In terms of 90-day readmission rates, patients who have been readmitted have poorer outcome scores. Multivariate analysis showed that high CCI scores and 90-day readmission rate both remained independent predictors of worse outcomes for SF-36 PCS, PMS and EQ-5D.
Discussion
CCI scores ≥6 predict for higher 90-day readmission rates, poorer quality of life and show poor potential for functional recovery 1-year post-operation in hip fracture patients. 90-day readmission rates are also independently associated with poorer functional outcomes. Peri-operatively, surgical teams should liaise with medical specialists to optimise patients’ comorbidities and ensure their comorbidities remain well managed beyond hospital discharge to reduce readmission rates. With earlier identification of patient groups at risk of poorer functional outcomes, more planning can be directed towards appropriate management and subsequent rehabilitation.
Conclusion
Further research should focus on development of a stratified, peri-operative multidisciplinary, hip-fracture care pathway treatment regime based on CCI scores to determine its effectiveness in improving functional outcomes.
Background
With the rising global incidence of hip fractures, the associated mortality and morbidity with this injury pose a major healthcare burden for the growing ageing population worldwide.1,2 Estimates suggest by 2050, 50% of hip fractures will occur in Asia. 3 Mortality after hip fractures is reasonably reported in recent literature, and the survivorship for these patients has been improving with better healthcare support in developed nations.3-7 To minimise post-fracture disability, hip fracture patients often undergo surgical treatment and subsequent intensive rehabilitation regime to return to pre-injury functional status. The interplay between patients’ comorbidities with post-operative functional outcomes is less understood, and is an area of increasing focus with more hip fracture patients surviving long after their index event.
In hip fracture patients, their post-operative recovery course after discharge can be complicated by adverse events such as readmissions. 30-day readmission rates have been used as a measuring stick for hospital performance and have been reported to range between 5 and 9% post-hip surgery.8-11 Causes of readmission range from both medical (infectious, cardiovascular, respiratory, genitourinary and gastrointestinal) and surgical causes, with medical complications being more common.8-10 Most literature focuses on 30-day adverse events, but the occurrence of these outcomes has been shown to still be quite significant beyond the early post-operative period, with studies showing 90-day readmission rates at 19% and mortality rates rising from 13.3% at 1 month to 15.8% in 3 to 6 months.12,13
Research has gone on to identify predictors for these adverse events, and exacerbation of active comorbid conditions is known to play a large role.12-14 The age-adjusted Charlson Comorbidity Index (CCI) has been shown to predict for post-operative complications, along with 30-day, 1-year as well as 5-year mortality rate in surgically treated hip fracture patients.15-17 A study by Lei Jiang et al revealed that patients of a higher CCI category (≥6) had an increased 5-year mortality rate compared to those with a CCI category of 3 and below. 17 Identification of patients at high risk for adverse events based upon their comorbidity profile could aid in better post-op recovery planning and the provision of a suitable level of care for individual patients, optimising functional outcomes and preventing complications, thereby lowering morbidity and readmission rates. 8
Studies on functional recovery after hip fractures are increasingly published. There remains a paucity of literature reporting the influence of specific CCI categorical scores on 90-day readmission rates and the subsequent impact of CCI and readmissions on functional outcomes after hip fracture surgery.
The aim of our study is to analyse and identify how an individual’s comorbidity profile – based upon the CCI scores – has an impact on functional outcomes after hip fracture surgery and 90-day adverse outcome events in relation to hospital readmissions. We also aim to evaluate the potential impact of 90-day readmission on functional recovery. We hypothesise that higher CCI scores are associated with increased 90-day readmission rates and poorer progress in functional recovery after hip fractures.
Materials & Methods
Patient Recruitment
The study was approved by the Centralised Institutional Review Board at our institution. Prospectively collected data were obtained from our institution’s hip registry covering all hip fracture patients treated surgically at our tertiary institution from January 2013 to December 2016. Our inclusion criteria covered unilateral hip fractures sustained amongst the geriatric patient population that were commonly due to low velocity osteoporotic fractures. Patients with a complete set of pre-operative medical records and a full-set of 1-year post-operative outcome data were included in our study. Excluded were patients with pathological fractures, polytrauma and incomplete data set (ie missed interval follow-up visits or mortalities within 1 year).
Surgical Method and Post-operative Rehabilitation
Upon admission, all hip fracture patients in our institution regardless of comorbidities or complexity are routinely managed pre-operatively by a multidisciplinary team which includes medical specialists such as geriatricians. Patients with undisplaced neck of femur fracture had cancellous screws fixation surgery and those with displaced neck of femur fracture received bipolar hemiarthroplasty. Patients falling into the category of basicervical neck of femur fracture underwent intramedullary nailing. Intertrochanteric fracture patients underwent intramedullary nailing or dynamic hip screw surgery, while those with subtrochanteric fracture were treated with intramedullary nailing.
Post-operatively, all patients had x-rays obtained to ensure implants alignment was satisfactory. Subsequently, patients were referred to physiotherapy for ambulation and will remain in hospital till they are cleared for safety of ambulation by the physiotherapists and are medically fit for discharge.
Data Collection
Clinical data collected included patient demographics, type of fracture, comorbidity profile, CCI score at time of surgery, 90-day adverse outcome events and 1-year post-operative functional outcome assessment data.
Patients’ comorbidity profile data were taken to be the presence or absence of the specific comorbidity as previously diagnosed and recorded on their past medical history provided on our anaesthetist’s electronic records database. The anaesthetist pre-operative routine inpatient review provides the most updated information of patients’ active comorbidities at the time of surgery. CCI was developed in 1987 as a method of classifying comorbidity conditions that might affect mortality risk in the long run. 18 The comorbidities included cardiovascular, pulmonary, neurological, endocrine, renal, gastrointestinal and malignancy conditions. Each comorbidity is assigned a point weightage ranging from 1 to 6, and a summation of the scores will give rise to the overall CCI score. 19 For age-adjusted CCI score, additional points are assigned to different subset of age groups, with higher age groups garnering more weightage. Its application has been vast over the years, as it has been used worldwide as a prognostic indicator of mortality in a variety of fields encompassing both medical and surgical circumstances.20-24
All functional outcomes data were obtained via our institution’s fractures outcome database collated by the Orthopaedic Diagnostic Centre. Patients were evaluated pre-operatively (based on re-call of pre-fall functional status at admission) and assessed post-operatively at the following intervals of 3 months, 6 months and 1 year. For patients with severe dementia who have difficulty with re-call, their primary caregivers assisted in their assessments to obtain the most accurate reflection of their functional outcome assessments. From our hip fracture database cohort, our patient follow-up at 6 months was noted to be 76%. 1-year mortality rates were approximately 6–7% in each year from our gathered mortality data available. Within our country, post-hip fracture 1-year mortality rates are less than 15%.17,25,26 A recent study by Yong et al 27 showed that there has been a significant decrease in absolute hip fracture mortality by 20% to 40% over the past 15 years in Singapore.
A range of functional outcome assessments were used such as the Parker Mobility Score (PMS), EuroQol-5D (EQ-5D), as well as Short Form-36 (SF-36) health survey.
The PMS characterised in 1993 has been seen as a reliable assessment for mobility in hip fracture patients. 28 The range of score for PMS is from 0 to 9, with 9 being a reflection of higher mobility. 28 It evaluates patient’s ability to move within the house, outside the house or in the community setting such as shopping malls.
EuroQol-5D is a health-related quality of life assessment used to measure generic health status that can be useful for healthcare economic analyses. 29 EQ-5D questionnaire includes 5 dimensions of ‘mobility’, “pain”, ‘self - care’, ‘activity’ and “anxiety”, of which a score of 1 to 3 may be indicated for each section. 30 This creates a 5-digit health status profile which is converted into a single summary index that indicates how good or poor a health state is. The single summary index has a maximum score of 1 depicting the best outcomes. 30 In Singapore, it has been used to assess patients with rheumatic disorders and Parkinson’s disease.31,32 It has also been used prior in the orthopaedic field to evaluate outcomes of upper limb surgeries and spine surgeries.33,34
The SF-36 health survey has been widely used in the orthopaedic literature as a measure for rehabilitation outcomes, encompassing both a physical component summary (PCS) and a mental component summary (MCS).35-37
Statistical Analysis
Statistical analysis was carried out by categorising the patients into 3 groups based on their CCI scores: (1) CCI = 0–3, (2) CCI = 4–5 and (3) CCI ≥ 6. These score categories were similar to Jiang et al’s study analysing CCI score cut-offs in determining mortality. 17 A univariate analysis with a one-way ANOVA with Tukey post-hoc test was used to compare the 3 groups for quantitative variables while the Pearson chi-square test was used for categorical variables. Significant predictors were identified and subsequently included in a multivariate analysis. A P-value of <.05 was considered statistically significant. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 22 (IBM Corp., Armonk, New York).
Results
Patient Demographics
Patient Demographics, Clinical Data Summary and Analysis of CCI Scores With 90-Day Readmission Rates.The table above summarises the clinical data used in this study, indicating the patient demographics in each CCI score category, the type of fractures and the results of the univariate analyses looking into 90-day readmissions.

Adverse Outcomes
The 90-day readmission rate was 9%, 16.5% and 25.2% in the CCI 0–3, CCI 4–5 and CCI ≥ 6 groups, respectively (P = .002) (Table 1).
Univariate Analysis - Functional Outcomes
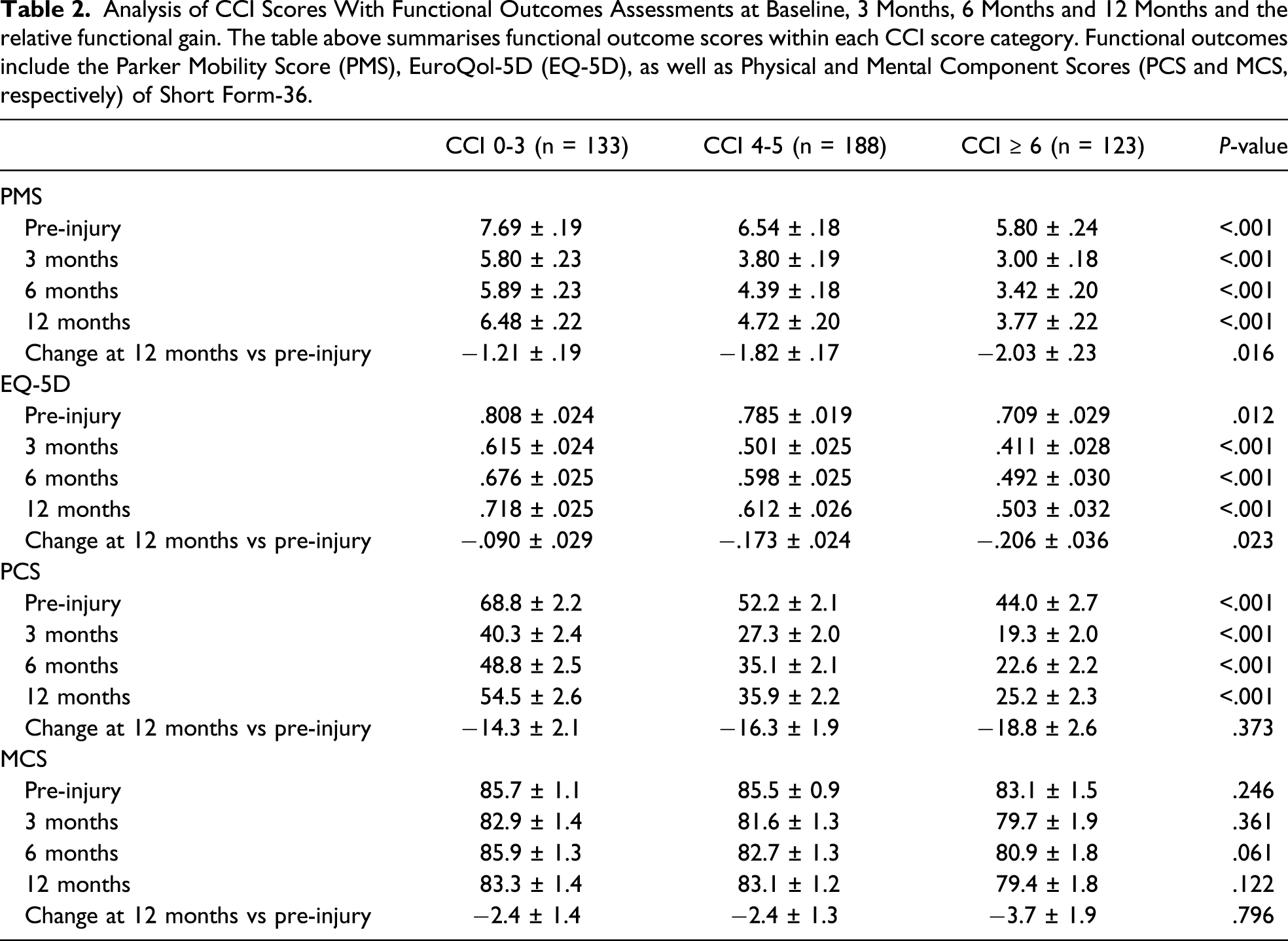
Analysis of CCI Scores With Functional Outcomes Assessments at Baseline, 3 Months, 6 Months and 12 Months and the relative functional gain. The table above summarises functional outcome scores within each CCI score category. Functional outcomes include the Parker Mobility Score (PMS), EuroQol-5D (EQ-5D), as well as Physical and Mental Component Scores (PCS and MCS, respectively) of Short Form-36.
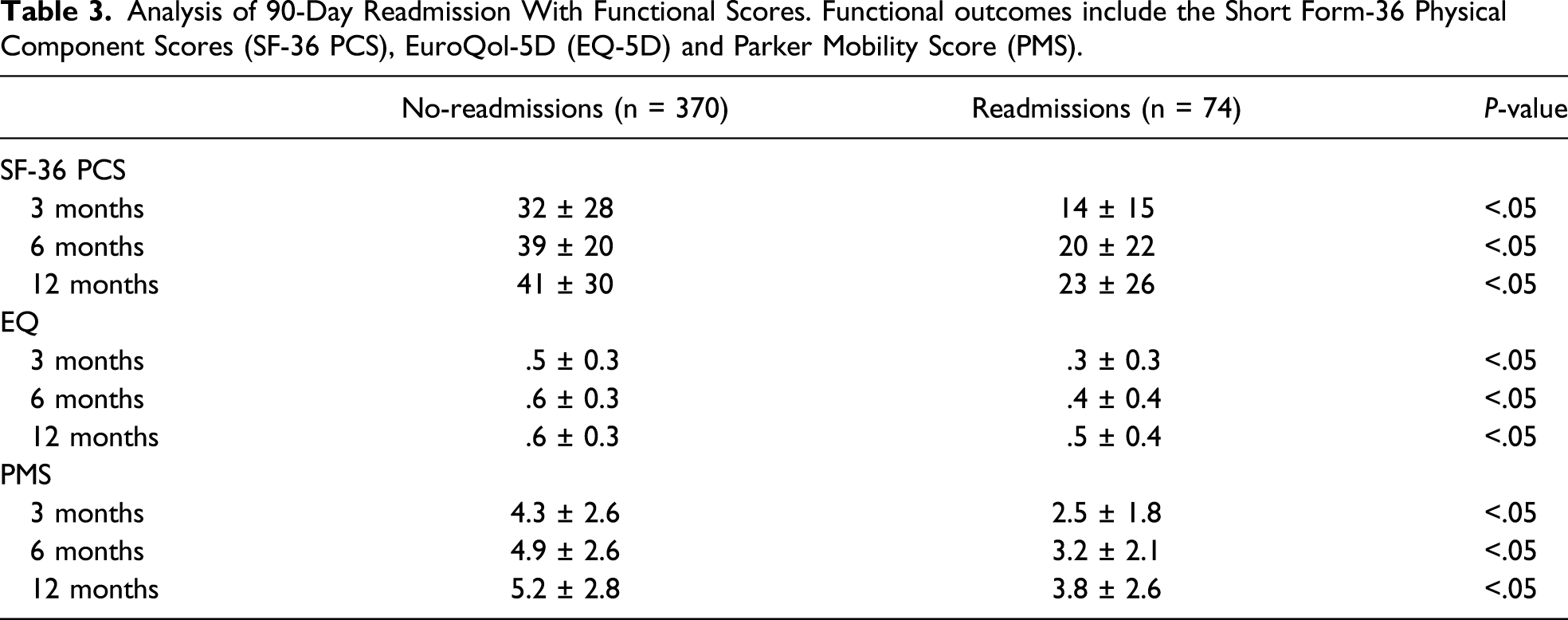
Analysis of 90-Day Readmission With Functional Scores. Functional outcomes include the Short Form-36 Physical Component Scores (SF-36 PCS), EuroQol-5D (EQ-5D) and Parker Mobility Score (PMS).
Multivariate Analysis - Functional Outcomes
Multivariate Analysis of SF-36 Physical Component Summary (PCS) Scores. 90-day Readmission Rates and CCI Categorical Groups were Included in the Multivariate Analysis of SF-36 PCS. Reference Group: CCI = 0–3.

Multivariate Analysis of Parker Mobility Scores (PMS). 90-day Readmission Rates and CCI Categorical Groups were Included in the Multivariate Analysis of PMS. Reference group: CCI = 0–3.

Multivariate Analysis of EuroQol-5D (EQ-5D). 90-day Readmission Rates and CCI Categorical Groups were Included in the Multivariate Analysis of EQ-5D. Reference group: CCI = 0–3.

* statistically significant
Discussion
While there have been previous studies that show higher CCI scores influence mortality and readmissions in the field of orthopaedics surgeries, there are few that depicted which categorical range of CCI scores is significant in predicting for 1-year functional outcomes and its effect on quality of life. The main finding of our study highlights that patients having a CCI score ≥6 generally have significantly higher 90-day readmission rate, poorer quality of life and perform functionally poorer at 1-year, compared to patients with CCI scores 0–3 and 4–5.
To our knowledge, this is the largest series in current literature reporting the significance of CCI scores and 90-day readmission rates on post-operative patient reported outcomes and quality of life scores in surgically treated hip fracture geriatric patients.
With regards to functional mobility score, notably PMS, patients with a CCI score of ≥6 predicted for poorer functional outcomes in terms of absolute scores for throughout the 1-year post-operative period. This subgroup of patients also started off at significantly poorer pre-injury baseline scores. It has been shown that a lower pre-fracture functional level concurs a strong influence on subsequent functional prognosis.38,39 We additionally compared delta change in functional gain to account for the varying baseline pre-injury status and found that patients with CCI ≥ 6 remained to have a larger decline in PMS after 12 months. In our multivariate analysis, higher CCI remains an independent predictor of poor functional outcomes PMS at each time intervals of 3, 6 and 12 months. In a 2016 prospective study by Gonzalez-Zabaleta et al, amongst age, gender, type of hip fracture and comorbidity, the best predictor of PMS post-hip fracture remains to be comorbidities; the average CCI score within the study was 6. 40
For SF-36 outcome measures of PCS and MCS, a high CCI score predicted for poorer physical functional outcomes of SF-36 PCS; however in terms of mental health score component, there were no significant differences between the CCI categorical groups. Studies that have evaluated SF-36 PCS post-hip fracture surgery had previously identified the following predictive factors: pre-fracture functional status, musculoskeletal comorbidity (as part of the cumulative index rating scale for geriatrics), nutritional status such as low albumin and gender.41-43 A 2016 study done by Huang et al in Taiwan recognises increased comorbidities as a negative impact on psychological mental health outcome scores amongst geriatric hip fracture patients. 44 However, in our study, CCI scores did not have a significant impact on SF-36 MCS. Further research needs to look into various psychosocial factors that may be involved in the management of patients who have sustained hip fractures.
90-day readmission rates were significant in predicting for worst SF-36 PCS and PMS outcomes, in both univariate and multivariate analyses. The readmission rates were significantly high at 25% for those patients with more severe comorbidities (CCI score ≥ 6). Patient-related characteristics such as age, comorbidities and pre-injury functional status have been shown to predict strongly for readmission post-surgery, compared to hospital-related factors. 10 As such, it is integral to address these patient factors with greater attention to be given to those of CCI ≥ 6. This subgroup of patients may be more prone to being readmitted for infections such as pneumonia, UTI or exacerbation of their comorbidity condition following stressors of undergoing a major hip surgery; these common readmission causes had been highlighted in prior studies.10,45,14 A CCI score of approximately 2–4 had been identified as an independent predictor for 30-day readmission post-hip surgery.9,37 However, the effect of some comorbidities such as cirrhosis and chronic kidney disease have been known to predict for orthopaedic readmission rates for far beyond 30 days.46-48
A number of geriatric studies have looked into the concept of frailty through a variety of frailty indexes such as the Chinese – Canadian Study of Health and Aging Clinical Frailty Scale (CSHA-CFS) or modified Frailty Index (mFI-11) and the impact of frailty on healthcare outcomes.49-53 These indexes act as comprehensive geriatric assessments covering frailty-related characteristics that briefly include activity level, presence of diseases or functional status.51,52 A study by Chen et al in 2019 53 aimed to look into temporal association between frailty and adverse outcomes, showing frailty has long-term effects on 1-, 3- and 6-month mortality and readmissions. Our study findings of the association between 90-day readmissions and increased CCI scores seek to be consistent with the outcome studies on frailty.
In the context of quality of life assessments, hip fractures are associated with poorer health-related quality of life (HrQoL), with deterioration in self-care, daily activities and mobility. 54 This is consistent in our study that shows a general decrease in EQ-5D in all our patients at the end of 1 year. Domains of self-care and both basic and independent activities of daily living are commonly areas that are most affected. 55 Factors such as pre-fracture CCI, institutionalisation prior to injury, functional limitations prior to fracture, MMSE scores, psychosocial factors, depression and type of intervention were shown to affect EQ-5D following a hip fracture.55,56 For our study, both high CCI scores and 90-day readmission rates were significant in predicting for poorer quality of life 1-year post-treatment for hip fractures.
Our study shows that higher CCI score ≥6 and 90-day readmission rates prove detrimental to 1-year post-operative functional scores and quality of life. Surgical teams should work in conjunction with corresponding medical specialists for optimisation of patients’ comorbidities in the peri-operative period. Such multidisciplinary approach should entail medical optimisation of patient’s comorbidities not only throughout their inpatient stay but also post-hospital discharge to ensure patients have appropriate outpatient follow-ups with the relevant speciality involved such that their active comorbidities remain well managed beyond discharge with an aim to reduce readmission rates.
Specific physiotherapy regimes to accommodate not only to patient’s age group but also to cater to each categorical CCI score groups could be implemented, with greater attention paid to those with a higher CCI score. With earlier identification of patient groups at risk of poorer functional outcomes, appropriate planning can be taken to account for possible prolonged physiotherapy rehabilitation that requires further rehabilitation at community hospitals, additional collaboration with dieticians and occupational therapists through multimodal interventions such as nutrition or arrangement of home rehabilitation post-discharge that seeks to improve physical function.57,58 Further research should focus on the development of a stratified, peri-operative multidisciplinary, hip-fracture care pathway treatment regime based on CCI scores to determine its effectiveness in improving functional outcomes.
Hip fractures are serious injuries that entail an important decision-making process as to whether to proceed with surgical treatment. Those with severe comorbidities (higher CCI scores) should be counselled accordingly pre-operatively in particular with regards to the likelihood of having poorer functional gain and higher complications such as readmissions. Emphasis should also be placed on primary prevention of hip fracture via incorporation of public health education towards falls risk factors and associated fall-prevention strategies, focus of physiotherapy exercises for improvement of general strength and balance amongst elderlies or pertinent home modifications that can aid to minimise fall hazards. 59
Limitations of the Study
Our study data were collected for a duration of 1-year post-operation. Obtaining outcome measures at 2 years and beyond will allow for more extensive analysis on longer term outcomes. Earlier studies have established CCI as a dominant predictor in mortality. 26 However, due to the variable periods of mortality and subsequent inconsistency in availability of functional assessments, patients with 1-year mortality were excluded from analysis based on incomplete data sets. In this aspect, comorbidity data and functional outcomes for patients with incomplete follow-ups or mortalities within 1 year could potentially be further looked into to compare the relationship of CCI scores and functional outcomes within this group vs those having complete 1-year follow-up. Third, comorbidities have been shown to significantly affect cost of hospitalisation following hip fractures. 60 Further collation of data on the socioeconomic factors involved may assist in identifying presence of social confounders that could affect one’s orthopaedic rehabilitation outcome. 61
Conclusion
CCI scores ≥6 predict for higher 90-day readmission rates, poorer quality of life and show poor potential for functional recovery within 1 year of surgical treatment in hip fracture patients. 90-day readmission rates are also independently associated with poorer functional outcomes. Multidisciplinary peri-operative care should be emphasised upon in hip fracture patients with comorbidities. With healthcare systems going towards value-driven care, further research can be done with regards to implementation of a stratified hip-fracture pathway treatment regime based on CCI scores which could assist in improving functional outcomes and reducing readmission rates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.