
Abstract
Introduction:
This study aims to assess the correlation of the age-adjusted Charlson comorbidity index (ACCI) with 5-year mortality in a surgically treated hip fracture population.
Materials and Methods:
A retrospective analysis was performed on 1057 patients aged 60 years and above who underwent surgery for hip fracture with a minimum of 5-year follow-up (92.2% 5-year follow-up rate) in a tertiary hospital. Manual review of patients’ electronic hospital records was performed to record demographic data, comorbidities, and length of stay. Mortality data were extracted from the hospital’s electronic medical records and corroborated with the National Electronic Health Record.
Results:
Of the 1057 patients, 283 (26.8%) were male. The majority of patients were 80 years of age and above (42.5%), with the oldest patient operated on age 102 with a mean age of 77.8 (8.6) years. Four hundred eighteen (39.5%) patients sustained extracapsular intertrochanteric fractures. The mean follow-up duration was 8 years and 3 days with an overall survivorship of 37.2%. A multiple regression model constructed with ACCI, age, gender, and fracture pattern demonstrated satisfactory predictive ability with a concordance statistic of 0.68. Patients with a higher ACCI category (≥6) had an increased 5-year mortality rate (41.8%) with an odds ratio of 13.6 (6.7-31.8, P < .001) compared to those with an ACCI category of 3 and below (89.3%).
Discussion:
The study demonstrates that ACCI correlated with 5-year mortality after surgical treatment of hip fracture. This information is pertinent in the counseling of patients with regard to their midterm survival following hip fracture surgery and may inform policy makers of the varied midterm survival rates in patients with differing ACCI scores and educate the allocation of health-care resources.
Conclusion:
The ACCI correlates with 5-year mortality after surgical treatment of hip fracture.
Introduction
Osteoporotic hip fracture is a leading health problem associated with significant mortality, estimated to range from 14% to 58% 1 year after sustaining the injury. 1 -3 With the proportion of older individuals rising throughout the globe driven by increased life expectancy, 4 the incidence of hip fracture is expected to rise from 1.66 million in 1990 to 6.26 million by 2050. 5 The burden is especially acute in developed Asian countries, and by 2050, more than 50% of all osteoporotic fractures will occur in Asia. 6 Given the rising burden of osteoporotic hip fractures on the public health system, prognosticating factors not only assist clinicians and patients in making informed decisions regarding their managements but also aid in the distribution of public health resources. 7
The Charlson comorbidity index (CCI) was first developed to evaluate a weighted series of comorbid disease to estimate the probability of death within 1 year. 8 It has since been modified in 1994 to adjust for age as an additional weighted variable by Charlson et al. 9 The CCI has been demonstrated to accurately predict in-hospital deaths, 10 30-day mortality, 11 and 1-year mortality. 12 In addition, various authors have correlated CCI with other outcome measures including length of stay and readmission rates after orthopedic surgery. 13 The use of CCI has also been expanded to predict long-term survival up to 5 years in patients with non-small cell lung cancer 14 as well as type 2 diabetic nephropathy. 15
The deleterious effects of a hip fracture persist beyond the oft-studied 1-year postfracture period. A meta-analysis by Haentjens et al demonstrated that the excess annual mortality persists over time in both men and women, 16 a finding that corresponded to a similar 22-year postfracture study. 17 The long-term mortality of patients with hip fracture highlights the need to consider factors such as comorbidities to optimize the long-term outcome of patients and prognosticate their survival. These findings warrant studies that evaluate mortality predictive indices to stratify patient populations. There is a paucity of literature evaluating the effect of comorbid diseases on mid- to long-term mortality in patients who underwent surgery for osteoporotic hip fractures.
The aim of this study is to assess the correlation of the age-adjusted CCI (ACCI) with 5-year mortality in a surgically treated geriatric hip fracture population in a developed Asian country and compare the time to event between patients with varying ACCIs. The authors hypothesize patients with a higher ACCI are correlated with a higher risk of 5-year mortality.
Materials and Methods
A retrospective cohort study was conducted at a tertiary orthopedic practice in an academic center. From January 1, 2007, to December 31, 2009, 1147 patients who were aged 60 and above and underwent surgery for hip fracture were recruited for our study. Patients who had a high-energy mechanism of injury, multiple fractures of the femur, and those with pathological lesions in other areas of the femur were excluded from the study. In addition, only patients with a minimum of 5-year follow-up or were died during this period were analyzed, leaving 1057 patients available for final analysis as shown in Figure 1. The average follow-up duration was 8 years and 3 days.

Patient selection process and exclusion criteria.
Manual review of patients’ electronic hospital records was performed to obtain demographic data, comorbidities, and length of stay data. Inpatient, 30-day, 1-year, and beyond 5-year mortality data were extracted from the hospital’s electronic medical records and corroborated with the National Electronic Health Record. 18 The ACCI 9 was obtained directly from the medical records and the patients were classified into ACCI category 1, 2, and 3 with an ACCI of 0 to 3, 4 to 5, and 6 and above, respectively. Institutional review board approval was obtained for this study.
Statistical Analysis
Continuous data have been summarized by mean (standard deviation) or median (interquartile range) as appropriate and categorical data by frequency (%). The t test or the Mann-Whitney test as appropriate was used to evaluate differences in continuous predictors between the groups. The χ2 test and Fisher exact test as appropriate were used to evaluate associations between the primary outcome and categorical predictors of interest. Univariate logistic regression was used to assess the relationship between the outcome and the predictors of interest. The multiple logistic regression model included the statistically and clinically significant predictors. The Hosmer-Lemeshow goodness-of-fit test was used to check for model adequacy.
Kaplan-Meier curves were plotted to assess the differences in 5-year mortality with respect to different categorical predictors of interest. The log-rank test was used to test for difference in survival. The Cox proportional hazards model was used to assess the relationship between 5-year survival and different predictors of interest.
Results
Of the 1057 patients, 283 (26.8%) were male. The majority of patients were 80 years of age and above (42.5%), with the oldest patient operated on age 102. Four hundred eighteen (39.5%) patients sustained extracapsular intertrochanteric fractures. The mean duration of operation was 62 (60) minutes. The most prevalent comorbid conditions were hypertension (66.1%), high cholesterol (35.8%), and diabetes mellitus (30.3%), reflected in the baseline characteristics in Table 1.
Preoperative Characteristics and Univariate Predictors of 5-Year Mortality.

Univariate analysis was performed to identify predictors of 5-year mortality as listed in Table 1. Multivariate analysis revealed that age group (odds ratio [OR]: 2.33, 1.65-3.34, P < .001), male gender (OR: 2.08, 1.54-2.81, P < .001), intertrochanteric fracture pattern (OR: 1.30, 1.00-1.70, P = .05), and the comorbidities identified in Table 2 were significant predictors for 5-year mortality. Significantly, the OR of 5-year mortality was almost 10 times higher in patients with end-stage renal failure, superseding that of cancer (OR: 2.53, 1.70-3.81) and dementia (OR: 2.10, 1.27-3.51) in our population.
Multivariate Analysis of Univariate Predictors of 5-Year Mortality.

A multiple regression model constructed with ACCI, age, gender, and fracture pattern as factors demonstrated satisfactory predictive ability with a concordance statistic of 0.68 and the respective ORs are described in Table 3. For the multiple regression analysis, we did not include age group as it is collinear with CCI. Patients with an ACCI category of 3 and below, 4 to 5, and 6 and above had a 5-year survivorship of 89.3%, 62.1%, and 41.8%, respectively. The mortality rates of patients in the varying ACCI categories at 30 days, 1 year, and 5 years are also described in Table 4.
Multiple Regression Model Using Gender, Fracture Pattern, and ACCI as Predictors of 5-Year Mortality.

Abbreviation: ACCI, age-adjusted Charlson comorbidity index.
30-Day, 1-Year, and 5-Year Mortality Rates for Patients in Varying ACCI Categories.
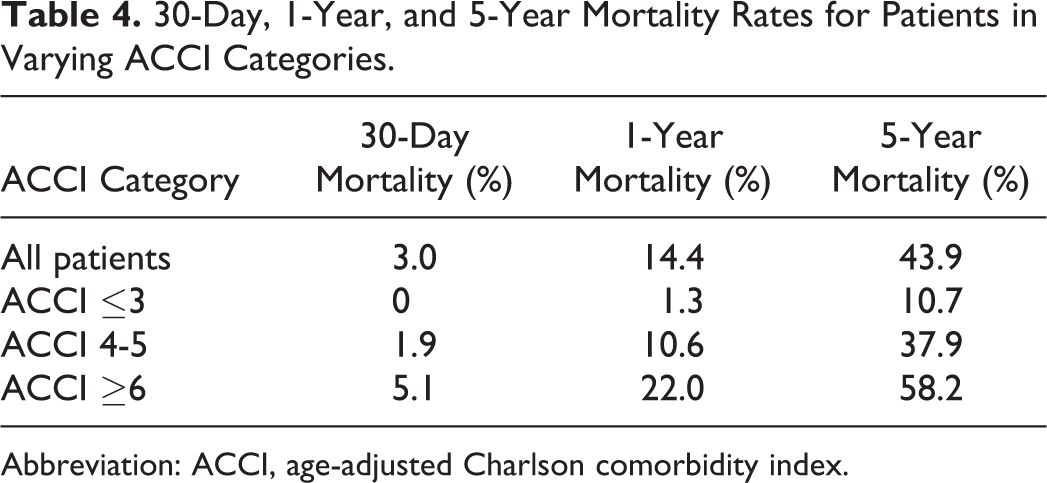
Abbreviation: ACCI, age-adjusted Charlson comorbidity index.
The Kaplan-Meier curves by ACCI categories in Figure 2 demonstrate differences in 5-year mortality. The log-rank test was statistically significant for testing differences in survival by all the above predictors.

Kaplan-Meier survival curves of patients in the different age-adjusted Charlson comorbidity index (ACCI) categories: ACCI category 1: ACCI 3 and below; ACCI category 2: ACCI 4 to 5; and ACCI category 3: ACCI 6 and above.
Discussion
The study demonstrated that the ACCI correlated with 5-year mortality after surgical treatment of hip fracture in a geriatric population. Recent studies have demonstrated that the CCI correlates with 1-year mortality after hip fracture surgery in an Asian population, 19 but the study has shown that the correlative abilities of the ACCI extend to 5-year mortality. This information is particularly vital in an aging population with greater access to health care as the proper identification and management of higher risk patients can reduce mortality. 20 This is especially pertinent with studies demonstrating that hip fracture mortality after surgery has in fact increased in certain populations. 21
The 5-year mortality rates are similar to previously published studies 22 in Asian populations and reflect previous identification of hip fracture as an independent predictor of 5-year mortality in a similar population. 23 The relatively high 5-year mortality rates reflect the frailty of the osteoporotic fracture population and highlight the importance of identifying hip fractures as sentinel events limiting the longevity of geriatric patients. Although there is insufficient high-quality evidence to conclude that surgery affects hip fracture mortality, 24 some retrospective studies have shown that surgically treated patients had lower mortality rates, 25 decreased mobility, 26 and quality of life indices. 27 The information derived from this study will be useful in the targeted counseling of patient and family members prior to surgery.
The ACCI was chosen as it was demonstrated as the most predictive score in a study by Neuhaus et al. 10 While the updated score proposed by Quan et al 28 reflected a reweighted score based on advances in disease management, this did not translate into greater predictive ability for mortality after hip fracture surgery.
Besides the ACCI, the study also revealed other factors that correlated with 5-year mortality. Males were at higher risk of mortality, a finding echoed by previous studies. 29 The finding of increased 5-year mortality rates in patients with intertrochanteric versus neck of femur fractures is more controversial in existing literature, with some describing an increased mortality rate in patients with intertrochanteric fracture patterns owing to differences in intrinsic prefracture factors 30 but other studies have disputed this in univariate analyses. 31
Although diabetes, hypertension, and high cholesterol were the most prevalent comorbid conditions, their ORs did not demonstrate a correlation with 5-year mortality. The authors opine that the cumulative effect of multiple comorbidities and their complications were more important than the presence of these common individual comorbidities, thus highlighting the importance of a weighted comorbidity index in stratifying patients.
Of particular interest is the clinically significant OR of 5-year mortality in patients with end-stage renal disease detected in our study. The increased mortality post-hip fracture has been described previously, 32 and even in patients with chronic kidney disease not requiring dialysis. 33 However, the OR reported in our population exceeds those reported in other study populations, prompting future studies to determine whether this is due to greater mobility of patients with end-stage renal failure leading to hip fractures in our population or whether there is a genuine differential in post-hip fracture care in this fragile patient group leading to higher mortality rates.
Instead of using administrative data for the calculation of the CCI, the study reported CCI from manual review of patient medical records which improve the accuracy and sensitivity of the scoring, 34 eliminating errors encountered during coding. In addition, the national health-care database has enabled a centralized record of mortality data, leading to a low dropout rate, largely due to the inclusion of patients from different countries. Lastly, the study has included data from multiple surgeons of varying seniority to reflect the reality of hip fracture patients admitted to a busy tertiary practice in an academic center.
The authors acknowledge several limitations of the study. As a retrospective study, the use of OR may exaggerate the estimated relative risk, especially when the mortality rates increase at the 5-year follow-up. The study also did not include patients who were treated nonsurgically, the inclusion of which would have provided a control arm to determine differences in 5-year mortality rates. Lastly, the study was not able to control for other potential confounding factors such as initial injury severity scores, premorbid quality of life indices, and caregiver arrangements.
Conclusion
In conclusion, the ACCI has been shown to correlate with 5-year mortality in a surgically managed hip fracture population. Besides affecting the management of individual patients, the results may inform policy makers of the varied midterm survival rates in patients with differing ACCI scores and educate the allocation of health-care resources.
Footnotes
Authors’ Note
L.J., A.C., T.H., and J.K. contributed to study concept and design. L.J., C.N., and Y.C. did acquisition of data. Analysis and interpretation of data was done by L.J., N.N., and J.K. L.J., T.H., and J.K. drafted the manuscript. L.J., T.H., and J.K. did critical revision of the manuscript for important intellectual content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was made possible by funding support from the Singhealth Foundation Grant (grant number: SHF/HSRAg001/2015).