
Abstract
Introduction:
Low-energy proximal femur fractures are common in the aging population and the ability to identify patients at increased mortality risk provides surgeons information to improve informed decision-making with patients and families. We evaluated for gender differences in 1-year mortality after sustaining low-energy proximal femur fractures with subgroup analysis to identify the impact of fracture location, age, and comorbidities on mortality.
Materials and Methods:
Patients ≥40 years of age sustaining a low-energy proximal femur fracture identified at our institution between January 1, 2014, and December 31, 2017. International Classification of Diseases, Ninth Revision and International Classification of Diseases, Tenth Revision codes were used to identify comorbidities for calculation of the age-adjusted Charlson comorbidity index (ACCI). The county clerk database was searched to identify mortality within 1 year of injury. One-year mortality rates were calculated and multiple comparisons were made between genders controlling for age, fracture location, and/or ACCI.
Results:
Women presented with low-energy proximal femur fractures at a rate of almost 3:1 to men at our institution (P = .001). Men demonstrated a significantly increased ACCI at presentation (5.35 ± 2.55 vs 4.86 ± 1.77, P = .03). Men had an increased 1-year mortality rate for all (31.3% vs 21.5%, P = .004) and intertrochanteric (IT) fractures (36.2% vs 22.9%, P = .008). Controlling for ACCI, gender, and fracture location, men demonstrated increased mortality rate with IT fractures (P = .002) and trended toward but did not reach significance with femoral neck fractures (P = .07).
Discussion:
Men presenting with low-energy femur fractures are at an increased mortality risk compared to women. On average, men present with an overall worse health status as identified by ACCI, which could predispose these patients not only to fractures themselves but also impair their ability to recover from injury.
Conclusion:
Men are at an increased 1-year mortality risk after sustaining proximal femur fractures.
Keywords
Introduction
Pathologic fractures secondary to osteoporosis in the aging population are common occurrences throughout our health-care system. While hip fractures only account for approximately 20% of these fractures, they exhibit a substantial impact on patient mortality and morbidity. 1 As our population continues to grow in number and age, a subsequent increase in low-energy hip fractures is expected, with predictions reaching as high as 1 037 000 by 2050. 2 Continued investigation into identifying opportunities to modify and improve care for these patients provides investigators an opportunity to impact a significant portion of the health-care system moving forward.
Well-described physiologic differences between the genders places females at a significantly increased risk of developing osteoporosis. 3 In conjunction with other anatomical and biomechanical differences, fragility fractures also remain more common in women. 4 Thus, when these fractures occur in men, it may be a result of various comorbidities affecting the osseous and global health of the patient. Studies grounded in orthopedics, as well as across the medical field, have utilized variations in comorbidity calculators and frailty indices to evaluate for association between health status and mortality rates. 5 -9 We aim to further delineate the role specific patient characteristics play in mortality rates after sustaining a pathologic fracture of the hip secondary to osteoporosis.
Extensive evidence exists regarding the impact of low-energy proximal femur fractures on patient mortality. 5,6,10 -12 Continued investigation into femur fracture location, gender, and associated patient characteristics and their role in mortality are required to provide the most accurate information for patients and families. Our primary investigation is to evaluate for a gender difference in 1-year mortality after sustaining a low-energy proximal femur fracture. Secondary investigations include subgroup analysis for differences in 1-year mortality rates between genders by (1) age, (2) fracture location, and (3) comorbidities through use of the age-adjusted Charlson Comorbidity Index (ACCI).
Materials and Methods
After obtaining institutional review board approval, a retrospective analysis of low-energy proximal femur fractures occurring at a single level II regional hospital between January 1, 2014, and December 31, 2017, was conducted using International Classification of Diseases, Ninth Revision (ICD-9) diagnostic codes 820, 821 and 827 as well as International Classification of Diseases, Tenth Revision (ICD-10) diagnostic codes S72.0, S72.1, S72.2, S72.8, and S72.9. A total of 1434 patients were initially identified. Exclusion criteria included age <40 years, high-energy mechanism (such as motor vehicle accidents or fall from >3 ft), chronic fractures, and periprosthetic fractures. Subtrochanteric and greater trochanteric fractures were also excluded as their occurrences in lower energy mechanisms available in our retrospective review were rare. If the patient sustained a contralateral femur fracture within 1 year of initial injury, only the first fracture was considered for mortality analysis as there is only one mortality event possible. If a patient sustained a contralateral femur fracture greater than 1 year from the prior injury, they were included as a new patient.
Patients were divided into 2 groups based on femoral neck or intertrochanteric (IT) fracture. Initial diagnoses of greater trochanter fracture on plain films further identified as IT fracture by advanced imaging (computed tomography or magnetic resonance imaging) were included in the IT group. Age at the time of injury, date of birth, date of admission, and gender were obtained from the hospital medical record. Medical comorbidities for calculation of ACCI were obtained from the hospital database based on ICD-9 and ICD-10 codes. 13,14 Death records were obtained through a search performed using a local, county clerk’s database according to name and birthdate. Mortality rates were calculated within 1 year of injury.
Overall descriptive statistics were calculated with means and standard deviations for continuous data and frequencies for categorical data. Associations for dichotomous variables were calculated by odds ratios and tested for significance with χ2 analysis at a P value of ≤ .05. Differences between genders for continuous data were tested by Student t test for independent groups at P ≤ .05. Associations on mortality adjusted for morbidity and age was determined by logistic multiple regression using stepwise model loading. Power was calculated at 90% or greater to detect a 25% effect size as significant at P < .05. A total of 800 patients were needed to achieve power.
Results
Patient Demographics
A total of 1434 patients were identified by diagnostic code search. After exclusion criteria were imposed, a total of 807 patients were included in the study population, with women (590) presenting significantly more frequently than men (217), P = .001. The average age was 80.7 ± 10.5 for men and 78.1 ± 11.1 for women (P < .001). Men were significantly more likely to present with several comorbidities including myocardial infarction (11.1% vs 5.3%, P = .004), congestive heart failure (28.6% vs 17.8%, P = .001), peripheral vascular disease (16.6% vs 9.0%, P = .002), liver disease (3.2% vs 0.8%, P = .013), and metastatic cancer (2.8% vs 0.7%, P = .017). No other comorbidities included in the ACCI were found to be significantly different between the genders. Men presented with a significantly higher ACCI score (5.35 ± 2.55 vs 4.86 ± 1.77, P = .03). Women and men were most frequently calculated to have an ACCI in the 3 to 5 range; however, a significantly greater portion of women were in this category compared to men (61.5% and 48.8%, respectively, P = .009). While men had a higher percentage of patients in the ≥9 ACCI score group (12.4% vs 3.4%), this did not reach statistical significance (P = .12). There was no significant difference in percentage of men and women calculated in the 0 to 2 and 6 to 8 ACCI groups (P = .51 and P = .98; Table 1).
Study Population Demographics.a
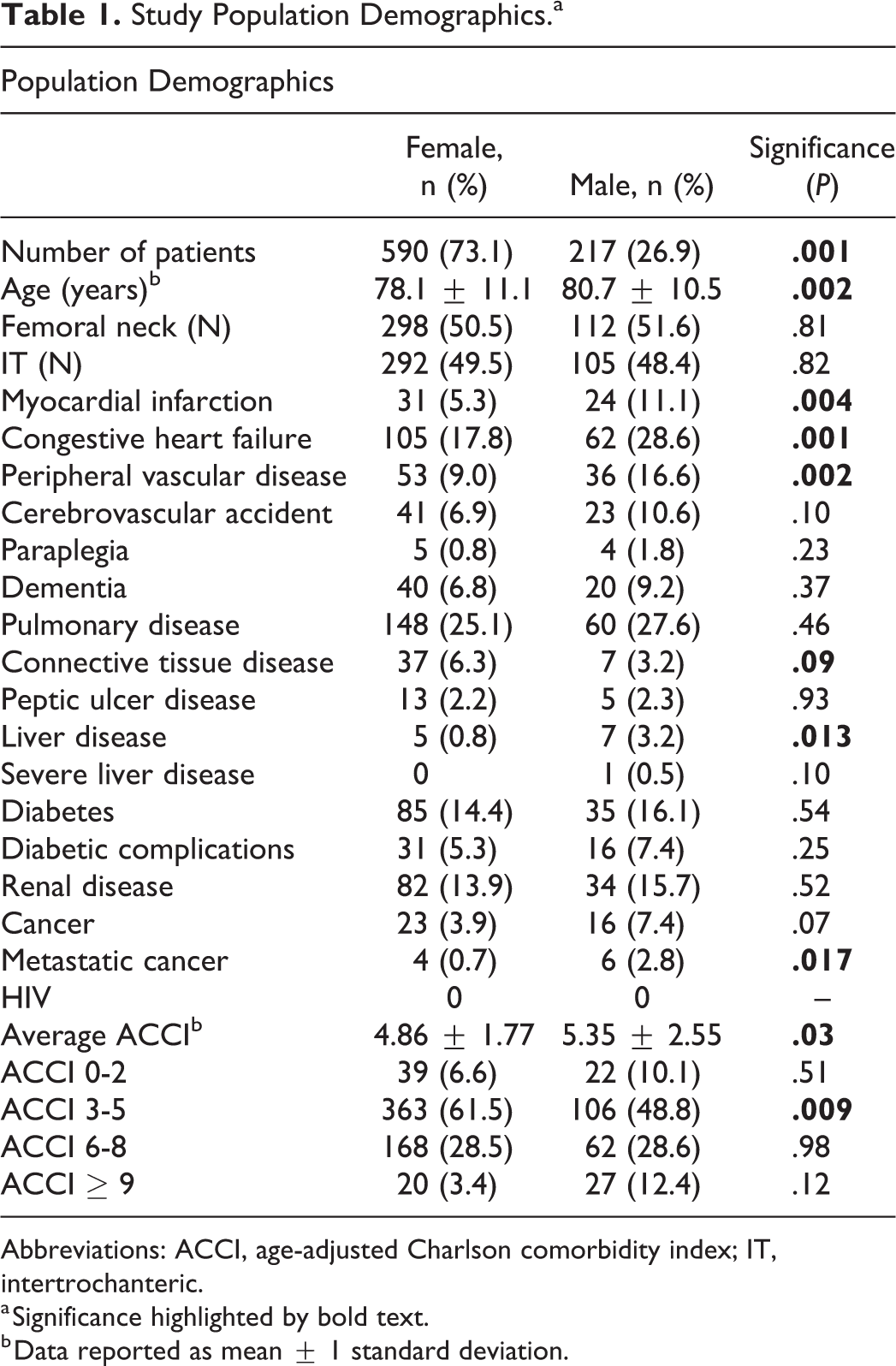
Abbreviations: ACCI, age-adjusted Charlson comorbidity index; IT, intertrochanteric.
a Significance highlighted by bold text.
b Data reported as mean ± 1 standard deviation.
Fractures
Of the 217 men included in our study, 112 (51.6%) sustained a femoral neck fracture while 105 (48.4%) sustained an IT fracture. Of the 517 women included in our study, 298 (50.5%) sustained a femoral neck fracture while 292 (49.5%) sustained an IT fracture (Table 2). There was no statistical difference in rate of femoral neck versus IT fractures for men and women with P values of .81 and .82, respectively.
One-Year Mortality Rate by Fracture Type, Age Decade, or ACCI.
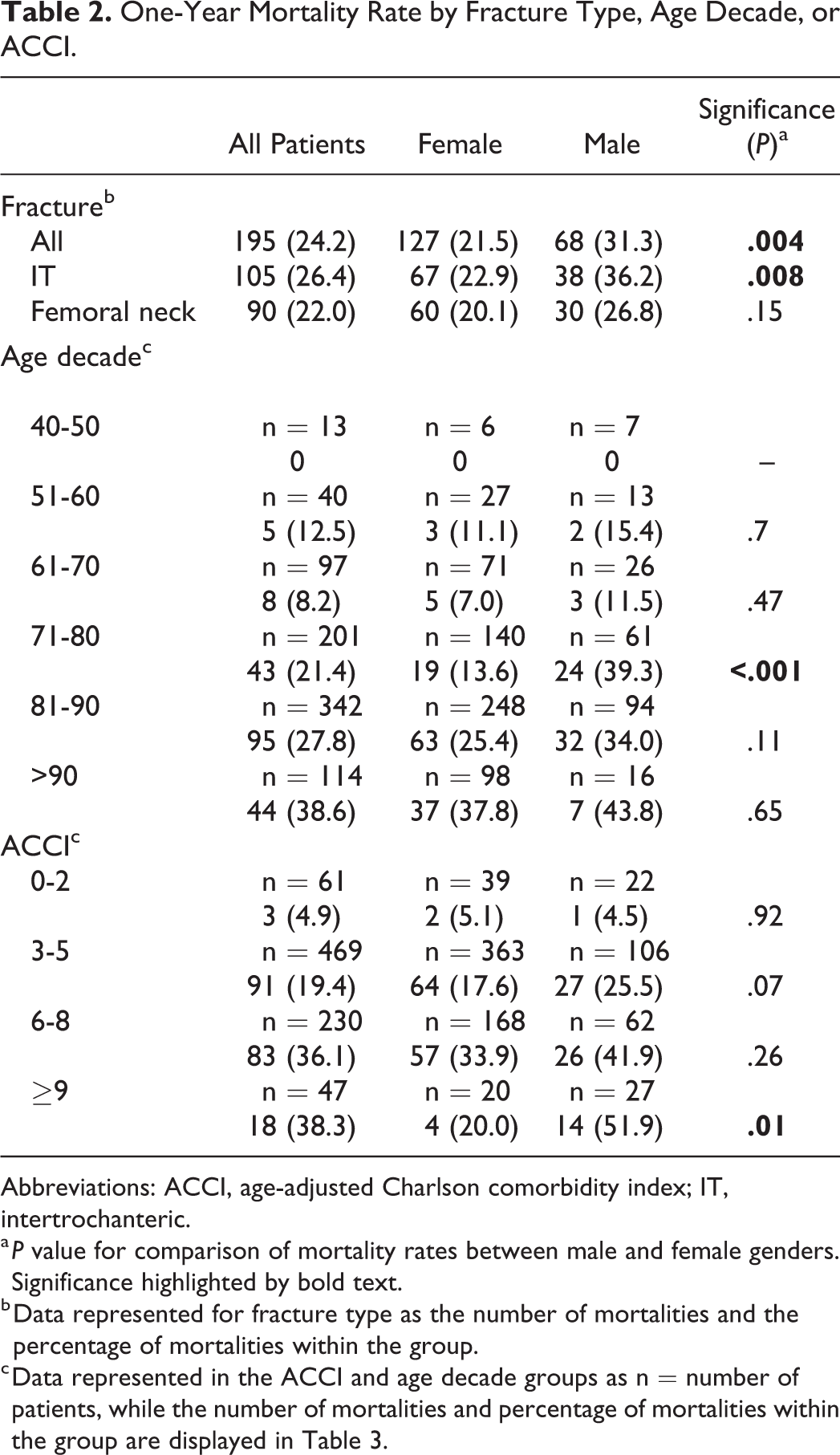
Abbreviations: ACCI, age-adjusted Charlson comorbidity index; IT, intertrochanteric.
a P value for comparison of mortality rates between male and female genders. Significance highlighted by bold text.
b Data represented for fracture type as the number of mortalities and the percentage of mortalities within the group.
c Data represented in the ACCI and age decade groups as n = number of patients, while the number of mortalities and percentage of mortalities within the group are displayed in Table 3.
One-Year Mortality
Men demonstrated an increased 1-year mortality rate for all fractures (31.3% vs 21.5%, P = .004) and for IT fractures (36.2% vs 22.9%, P = .008). Men trended toward but did not reach a significant increased rate of mortality for femoral neck fractures (26.8% vs 20.1%, P = .15; Table 2). One-year mortality rates were significantly different by decade of life at 0%, 12.5%, 8.2%, 21.4%, 27.8%, and 38.6% for the fourth through ninth decades, respectively, for both genders (P < .0001; Table 2). Controlling for gender and age showed significance for increased male 1-year mortality in the 71- to 80-year-old age-group (39.3% vs 13.6%, P = .0001) and trended toward but did not reach significance in the 81- to 90-year-old age-group (34% vs 25.4%, P = .11). There were no significant differences when controlling for age and gender in the other decades of life. Controlling for age and fracture location for all patients showed no significant differences in 1-year mortality rates, while mortality increased by decade for each fracture type except between the fifth and sixth decade for IT fractures (Table 3).
One-Year Mortality by Age Decade and Fracture Location for All Patients.a

a P value for comparison between fractures types.
Controlling for age and medical comorbidities utilizing the ACCI demonstrated an increased rate of 1-year mortality for men in the ≥9 group (51.9% vs 20%, P = .01) for all fractures. Men trended toward an increased 1-year mortality rate in the 3 to 5 (25.5% vs 17.6%, P = .07) and 6 to 8 (41.9% vs 33.9%, P = .26) ACCI groups; however, this did not reach statistical significance (Table 2).
Finally, controlling for gender, fracture location, and medical comorbidities utilizing the ACCI, there was a significant increase in 1-year mortality for males with IT fractures (P = .002). Femoral neck fractures trended toward an increased 1-year mortality for men but did not reach statistical significance (P = .07; Figure 1).

One-year mortality rates by gender, age-adjusted Charlson comorbidity index (ACCI), and fracture location. Presented as percentage mortality for each ACCI score group. Female = solid line, male = dotted line. A, Femoral neck fractures. Increased mortality rate for men trended toward but did not reach statistical significance (P = .07). B, Intertrochanteric fractures. Men demonstrated a significantly increased rate of mortality (P = .002).
Discussion
Our study provides several interesting findings into the 1-year mortality risk for aging patients sustaining fragility fractures of the proximal femur when stratified for comorbidities, gender, and fracture location. Consistent with several previous studies, females presented significantly more frequently to our institution with low-energy proximal femur fractures at a ratio of almost 3:1. 15 -17 Several biomechanical and physiologic differences of bone morphology between the genders places females at a greater risk for osteoporotic fragility fractures. 1 A previous report demonstrated that bony architecture of the proximal femur differs between genders, with females tending to exhibit greater femoral anteversion, decreased cervicodiaphyseal angle, and less femoral offset. 18 Additional investigations have linked these differences, in addition to numerous other proximal femoral geometric findings, to low-energy hip fractures. 19 -21 Interestingly, while women presented more frequently with hip fractures to our institution, both genders presented with an almost identical 1:1 ratio of IT and femoral neck fractures.
Men were found to be at an increased risk of 1-year mortality across several different measures in our study. Prior to controlling for age, fracture location, and comorbidities, men demonstrated significantly increased mortality rates for all fractures as well as IT fractures, while femoral neck fractures trended toward but did not reach statistical significance. When controlling for age and gender, men were found to be at an increased risk of mortality in the 71 to 80 age-group and trended toward increased risk in the 81 to 90 age-group. These age groups accounted for over 51% of the total study population, 417 patients, and represent a significant portion of the patients presenting with these fractures. One-year mortality was higher for males in the other decades as well; however, numbers were likely too low in those age groups to detect a significant difference. Utilizing the ACCI to control for age, gender, and comorbidities, men showed significantly increased 1-year mortality rate for the ≥9 group and trended toward increased mortality in the 3 to 5 and 6 to 8 groups. These findings are consistent with a prior study using a similar ACCI model finding increased mortality rates at 1 year for both males and patients with increased ACCI. 5 When examining our findings in comparison to the multiple comorbidities found to be significantly more common in males presenting with low-energy hip fractures, it suggests that a decreased overall health status possibly predisposes these men to sustaining the fractures, as well their ability to recover from the injury.
Several other studies have also utilized comorbidity indices in a similar fashion. Schnell et al found a Charlson score of 4 or greater was predictive of 1-year mortality. 22 Their findings also mirrored our study showing men had an increased 1-year mortality rate compared to women. Conversely, their investigation included independence for activities of daily living (ADLs) and Parker mobility score, demonstrating increased mortality as independence and mobility decreased. Additionally, another study utilizing a different index (5-factor modified frailty index) found elevated mortality rates for patients with increasing comorbidities and decreasing independence for ADLs but did not evaluate for variation between genders. 6 While our study did not include mobility scores or evaluation of ADL independence, we recognize the impact these factors have on a patients’ ability to function after a hip fracture and their role in mortality. Ultimately, it is continually reproduced in the literature that decreasing health status is associated with increasing mortality rates for hip fracture patients across a variety of comorbidity and functional indices.
Furthermore, controlling for fracture location in addition to the ACCI and gender, we found a significant increase in 1-year male mortality for IT fractures and a trend toward significance for femoral neck fractures. Interpretation of these findings does not necessarily suggest that proximal femur fracture location imposes different mortality risks on the genders. Rather, that by controlling for the many confounding variables presented in data analysis regarding low-energy hip fractures in a diverse patient population, we find men continue to be at an increased mortality risk. This is similar to a previous study performed by Kannegaard et al, where despite controlling for fracture location and comorbidities, men continued to demonstrate a significant increased risk of mortality. 15 While interpretation of the study could lead to focusing solely on the increased rate of mortality for men, it is important to note the risk for 1-year mortality remains substantial for both genders.
The overall 1-year mortality rate for all patients was 24.2% for all fractures, 26.4% for IT fractures, and 22.0% for femoral neck fractures, which is consistent with a previous systematic review of randomized controlled trials in North America between 1981 and 2012. 12 Mortality rates for all patients increased by age, except for the 51 to 60 to 61 to 70 decades. The slight decrease, although not significantly different, could be attributed to the relatively low number of patients in the fifth decade of life who present with low-energy femur fractures. Conversely, significant medical comorbidities could account for patients presenting with low-energy femur fracture in this age-group and present challenges for recovery. We attempted to control for this phenomenon by utilizing the ACCI, which showed increased mortality rates with increasing ACCI for men and women except for the female >9 ACCI group. The utilization of ACCI, other risk stratifying indices, or at the very least, an in-depth evaluation of patients’ comorbidities at presentation provides surgeons the opportunity to identify patients of both genders at increased risk of 1-year mortality.
Currently, in our institution, hip fractures patients are admitted to the orthopedic service unless extenuating circumstances (ie, already admitted to another service, multiple injuries resulting in trauma evaluation, etc) are present. Standardized protocol including medical management, nutritional, case management, and physical/occupational therapy consults is placed. Additional consults of other medical services are obtained on a case-by-case basis. The opportunity provided by our study and other investigations of a similar design utilizing various comorbidity and frailty indices is for the surgeon to identify specific patients at increased mortality risk and create protocols which further allow patient specialization of care to improve outcomes. A previous study evaluated a hip fracture program and its successful impact on complication rates and mortality. 23 Other investigations have aimed to identify various prognostic factors for recovery as well as in-hospital and community interventions to reduce morbidity and mortality with varying levels of success. 24 -26 Further investigation in our patient population is required to evaluate if extending our standardized protocol to include formal in-hospital consultation, confirmed postdischarge follow-up with various medical specialties or confirmed expanded community services could optimize the patient’s health status and reduce their 1-year mortality risks.
There are several limitations associated with our study. While our study population reached an adequate level determined by power analysis, limited patient numbers in several subgroups could have limited our ability to find significant findings in our comparative analysis. As several of these investigations trended toward but did not reach statistical significance, expanded study with increased patients within the subgroups could lead to further demonstration of the links between comorbidities and 1-year mortality after sustaining a low-energy proximal femur fracture.
Additionally, the retrospective design of our study and use of electronic medical records (EMRs) for data collection depends on provider documentation at the time of injury. Our study spanned a change in our EMR from ICD-9 to ICD-10 coding for admitting fracture diagnosis and patient comorbidities. It is possible some comorbidities and fractures were inappropriately coded and missed by our data collection, leading to underreporting. We used broad, encompassing codes provided by Sundararajan et al to maximize our ability to collect comorbidity data. 13 We also utilized multiple codes for femoral fractures extending beyond IT and femoral neck fractures and then implemented our exclusion criteria to limit the number of missed fractures as a result of inappropriate coding.
Finally, collecting mortality data required using a local government database. Patient mortality events from patients not residing in the general area (ie, visiting the area, tourism, etc) would likely be missed. However, we are a community level II trauma center, with the majority of our patients residing in the local area. Although unable to estimate the number of patients missing mortality from the local database, a significant gender differential is not likely.
Conclusion
Men were identified to be at a significantly increased risk for 1-year mortality after sustaining a low-energy proximal femur fracture. While men were at an increased mortality risk, these fractures demonstrated a significant impact on 1-year mortality for both genders, consistent with previous reports. Utilization of the ACCI showed a general propensity for increased mortality rates for patients of decreased health status. Further investigation is required in our patient population if identification of patients at elevated risk for mortality would benefit from expanded in-hospital and postdischarge resources to optimize their health and decrease their mortality risk.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Published with funding provided by Ascension Genesys Hospital Graduate Medical Eduction fund.