
Abstract
Introduction
The purpose of this study was to identify the timing and nature of complications associated with distal femur fracture surgery in patients aged 65 and older using the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database.
Methods
The ACS NSQIP database was queried for adults aged 65 and older who received surgical treatment for a distal femur fracture between 01 January 2015 and 31 December 2021. Cox regression models and risk tables adjusted for baseline clinical characteristics were created for 14 complications (Superficial Surgical Site Infection (SSI), Deep SSI, Organ/Space SSI, Pneumonia, Pulmonary Embolism (PE), Deep Venous Thrombosis (DVT), Urinary Tract Infection (UTI), Stroke/Cerebrovascular accident (CVA), Myocardial Infarction (MI), Renal Failure, Cardiac Arrest (CA), Re-operation, Sepsis, and Death within 30 days of surgery). Model summaries were used to identify significant variables with a Bonferroni correction applied.
Results
A total of 3956 adults met inclusion criteria and were included in analysis. The most common complications were UTI (5.2%), death (4.1%), and pneumonia (3.4%). Complications typically occurred within 14 days after surgery, except for SSI, which occurred between post-op days 11 and 24.
Conclusions
Distal femur fractures are a substantial source of morbidity and mortality in the older adult population. Our findings underscore the need for comprehensive preoperative risk assessment and patient management strategies to mitigate the impact of identified risk factors in this vulnerable population.
Keywords
Introduction
Fragility fractures of the lower extremity are a substantial source of morbidity and mortality for the U.S. aging population. 1 Distal femur fractures account for 4%-6% of fragility fractures of the femur, with an annual incidence of 4.5/100.000 in the general population and more than half occurring in individuals aged over 70 years. These injuries typically result from low-energy trauma, such as ground-level falls, and the 1 year post-operative mortality rate ranges from 13.4% to 35%, similar to hip fractures.2-6 The management of distal femur fractures can be challenging. The fractures are often comminuted, intra-articular, periprosthetic, and involve osteoporotic bone. The high incidence of comorbidities in the older adult population may also impact operability, recovery, and survival. Addressing these multifaceted issues requires a multidisciplinary approach. Innovative interventions, such as geriatric fracture centers and multidisciplinary geriatric fracture programs, have shown promise in improving patient outcomes and reducing mortality rates.
Most previous studies involving distal femur fractures have focused on the technical aspect of patient care with limited data on perioperative complications.5,7-14 In particular data are scarce regarding the timing of common local and systemic complications of operative-managed distal femur fractures in older adult patients. 15 Adequate evidence on local and systemic complications is crucial to set expectations appropriately for healthcare providers and patients. 16
This study aims to determine the timing and rates of perioperative complications in older patients with isolated low-energy distal femur fractures. By analyzing complication timing, providers can optimize care strategies and improve patient outcomes. The study utilized a national multi-center surgical database to evaluate the timing of complications after surgery for distal femur fractures in older patients and whether complications were associated with patient factors.
Methods
We conducted a retrospective cohort study using data from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP), a database of patient demographics, comorbidities, intraoperative data, and 30-day postoperative patient outcomes undergoing a broad range of surgeries across surgical subspecialties. The database includes data from over 600 hospitals with standardized data definitions for over 200 perioperative variables. The data are collected by trained surgical and clinical reviewers, with audit reports showing an inter-reviewer disagreement rate below 2%.17,18 Outcomes are collected from the medical record or by contacting patients after discharge, including the incidence of 30-day postoperative morbidity and mortality.
Patients
Baseline Clinical Characteristics.

an (%).
Frequencies of Complications Occurring Before or on the Day of Discharge.

Cox-regression models and risk tables were created for each complication, adjusting for baseline clinical characteristics such as age, gender, BMI, CPT code, and co-occurring conditions (diabetes, smoking status, functional status, COPD, CHF, hypertension medications, steroids, bleeding disorders, disseminated cancer, dialysis, and pre-operative sepsis). Only complications with a sample size of more than 30 were included in both the figure and the table. Model summaries were generated to identify significant variables. Since 24 risk factors for each complication were tested, we applied a Bonferroni correction to control for multiple hypothesis testing, considering P-values ≤.002 (.05/24) as statistically significant.20,21 All statistical analyses were conducted using R-4.3.0 (R Core Team, Vienna, Austria). 22
Results
A total of 3956 patients met inclusion criteria and were included in the study (Figure 1). Most of the patients were female (82.0%), independent before surgery (78%), and in the age group of 70-79 years (35.0%). Source and filter flow chart.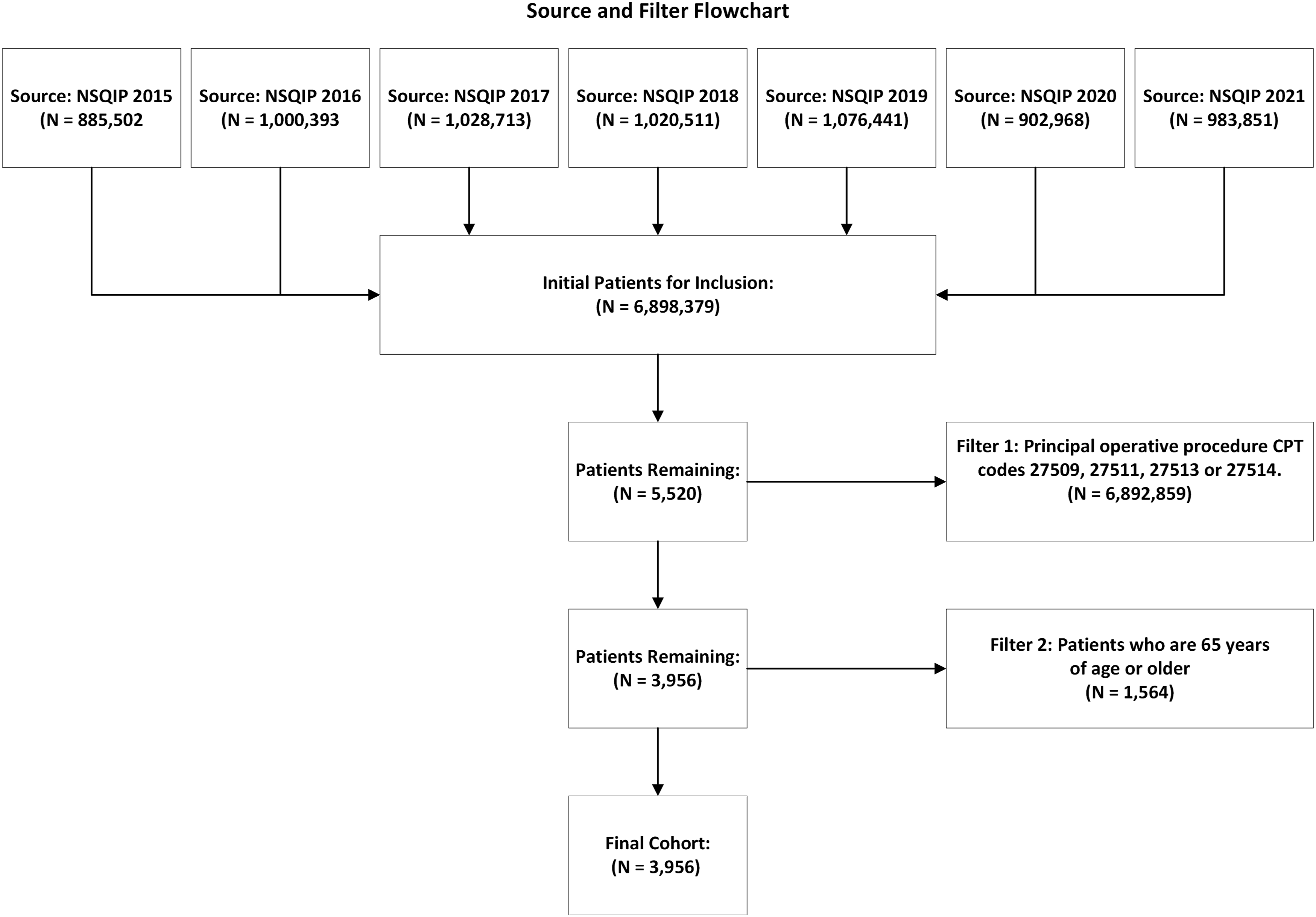
Frequencies and Median Day of Diagnosis of Post-Operative Complications.

aMedian [Interquartile Range].
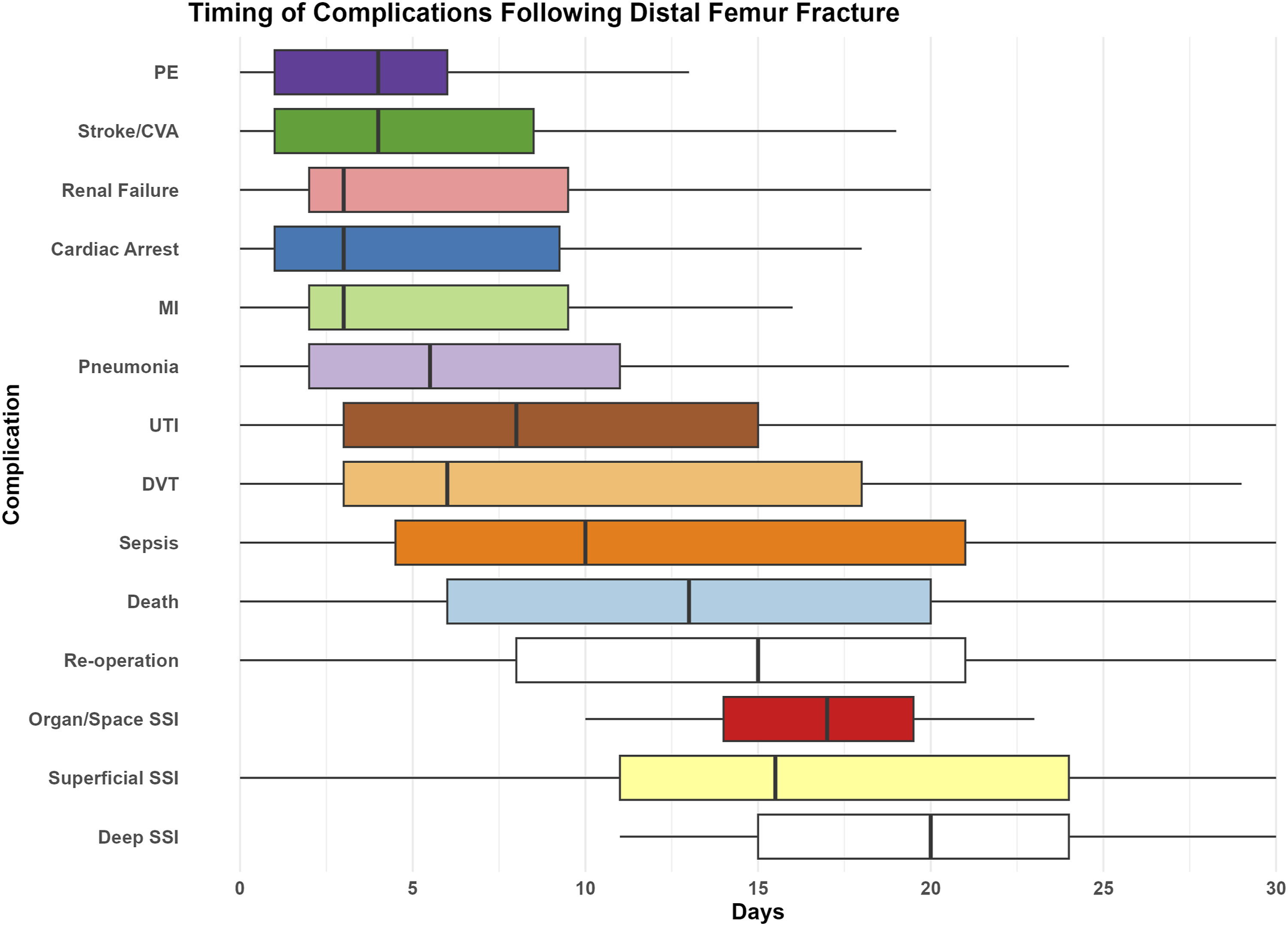
Timing of complications following distal femur fracture.
The median days from surgery to discharge were 4.0 days. The 5 most common postoperative complications diagnosed before discharge was renal failure (78.3%), stroke/CVA (69.2%), cardiac arrest (68.8%), pulmonary embolism (67.9%), and pneumonia (61%), while SSI (superficial and deep) were primarily diagnosed following discharge (Table 2).
Risk factors for each complication were listed in Table 5 (Appendix). It is worth noting that bleeding disorder was a significant risk factor for SSI (P = .002), pulmonary embolism was associated with disseminated cancer (P = .002), and smoking was a risk factor for re-operation (P = .002). Poor functional status (totally dependent) (P < .001) and congestive heart failure (CHF) (P < .001) were significant risk factors for death.
Individual Cox-regression survival models, adjusted for baseline clinical characteristics, are illustrated in Appendix Figure A1.
Discussion
Distal femur fractures in older adults pose significant challenges for management due to comorbidities, osteoporosis, and periprosthetic fractures. In recent years the introduction of improved implants has expanded available options for operative treatment. These include intramedullary nailing with various distal locking features, lateral locking plates, and primary distal femoral arthroplasty. The availability of these implants and techniques has significantly increased the treatment options for distal femur fractures. 23
Despite extensive research on distal femur fractures, comprehensive evaluations of perioperative complications and mortality rates are still lacking. Using a large-scale national surgical database, the current study characterizes the timing of common complications following distal femur fracture surgery in geriatric patients. This study found that complications primarily manifested within 14 days post-surgery, except for SSIs (superficial and deep), which presented later in the postoperative course. Close patient follow-up during this vulnerable period may help identify these adverse events and enable timely interventions by providers.
The median days of diagnosis for several complications in distal femur fractures and hip fractures using a similar dataset showed that while the median days of diagnosis for most complications were similar between the 2 groups, the timing of DVT diagnosis was earlier in distal femur fracture patients (median 6 days) than in hip fracture patients (median 9 days). 18 The differences in timing may be due to variations in thrombo-prophylaxis protocols between the 2 groups. However, the interpretation of the findings is limited by the lack of data on post-operative venous thromboembolism prophylaxis in the ACS NSQIP database.
The findings of Table 2 highlight the importance of identifying risk factors for postoperative complications to inform patient care and improve outcomes. Several studies have identified risk factors that can increase the likelihood of SSIs following distal femur surgery. Lu et al 24 discovered that open fractures, obesity, smoking, and diabetes mellitus were risk factors associated with SSIs after distal femur fracture surgery. Similarly, Bai et al 25 found that independent risk factors for SSI after distal femur fracture surgery were open fracture, temporary use of external fixation, obesity, smoking, diabetes mellitus, and preoperative reduced albumin level. While our study identified bleeding disorder as a significant risk factor for superficial SSI, the exact mechanism underlying this association is not fully understood. However, previous research has demonstrated that increased blood loss is associated with an elevated risk of SSI.26,27 Additionally, our results suggest that septic shock may be a common risk factor for both UTI and sepsis, which is supported by previous research demonstrating the association between preoperative septic shock and subsequent infections in orthopedic trauma patients. 28 Concerning pulmonary embolism, individuals with disseminated cancer were identified as high-risk groups. Patients with disseminated cancer are associated with a hypercoagulable state, which increases the likelihood of DVT and pulmonary embolism.29,30 Overall, identifying risk factors for postoperative complications can aid in developing targeted interventions to improve patient outcomes. Our findings underscore the need for comprehensive preoperative risk assessment and patient management strategies to mitigate the impact of identified risk factors.
Previous research has shown that distal femur fractures in elderly patients have a high 1 year mortality rate ranging from 13.4% to 35%. 31 Age over 85 years is among the most significant risk factors, with mortality rates of up to 33% after 12 months and 50% after 5 years.5,32 The ACS NSQIP data does not provide data beyond 30 days following the procedure, and we could not report 1-year mortality. However, our study reported a 30-day mortality rate of 4.1%, within previously reported 30-day mortality ranges of 2% to 4.5%.31,33 The risk factors for high mortality included totally dependent pre-fracture function status and history of CHF. Similarly, Moloney et al 5 reported a higher Charlson Comorbidity Index (CCI), which includes CHF as a variable, as a predictor of 1 year mortality.
Co-management strategies play a crucial role in identifying and reducing complications in older adults with distal femur fractures. Given the challenges posed by comorbidities, osteoporosis, and periprosthetic fractures in this patient population, a collaborative approach involving multiple healthcare professionals can optimize patient care and outcomes. Close patient follow-up during the vulnerable postoperative period, particularly within 14 days, can aid in timely identification of complications, enabling prompt interventions by healthcare providers. Identifying risk factors for postoperative complications allows for the development of targeted interventions and preventive measures to mitigate the impact of these factors.
Limitations
One of the primary constraints of ACS NSQIP is that the data are limited to the first 30 postoperative days, which may not fully capture long-term outcomes, functional recovery, or quality of life for older patients with fractures. Additionally, the database does not include specific variables related to fracture types, surgical techniques, or implant choices, which are essential factors in understanding surgical outcomes. Specific to distal femur fractures, the ACS NSQIP database does not distinguish between native femur and periprosthetic fractures. Although a study in 2018 reported no significant differences in overall mortality between native bone and periprosthetic fractures, intramedullary nail or open reduction internal fixation, or across Orthopaedic Trauma Association fracture classifications, further studies are warranted to investigate implant/fracture type outcomes. 1 Furthermore, the ACS NSQIP data are collected from participating hospitals, which might not represent the broader healthcare landscape, leading to potential selection bias. This limits the generalizability of the findings. Finally, as a retrospective observational database, ACS NSQIP does not allow for establishing causal relationships, making it challenging to infer the direct impact of specific interventions or patient characteristics on surgical outcomes.
Conclusions
This study characterized the timing of the most common complications following distal femur fracture repair in older patients. The findings provide important information for healthcare teams that treat these patients to be aware of the highest risk periods for complications after distal femur fracture surgery to prevent adverse events.
Supplemental Material
Supplemental Material - Timing of Complications Following Surgery for Distal Femur Fractures in Older Adults
Supplemental Material for Timing of Complications Following Surgery for Distal Femur Fractures in Older Adults by Naoko Onizuka, Samuel Farmer, Jessica M. Wiseman, Gabriel Alain, Catherine C. Quatman-Yates, and Carmen E. Quatman in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Acknowledgments
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP provided the data used in this article; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions reached by the authors.
Author Contributions
NO and CEQ designed the study. NO and GA analyzed the data, and NO, SF, and JMW prepared the manuscript. All authors contributed to the review and revision of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging under the Paul B. Beeson Emerging Leaders Career Development Award in Aging (K76AG068435).
Ethical Approval
This study was exempt from approval by our Institutional Review Board.
Supplemental Material
Supplemental material for this article is available online.
Appendix
Cox-regression survival plots for death (A), deep venous thrombosis (B), myocardial infarction (C), pneumonia (D), pulmonary embolism (E), re-operation (F), sepsis (G), septic shock (H), superficial surgical site infection (I), and urinary tract infection (J).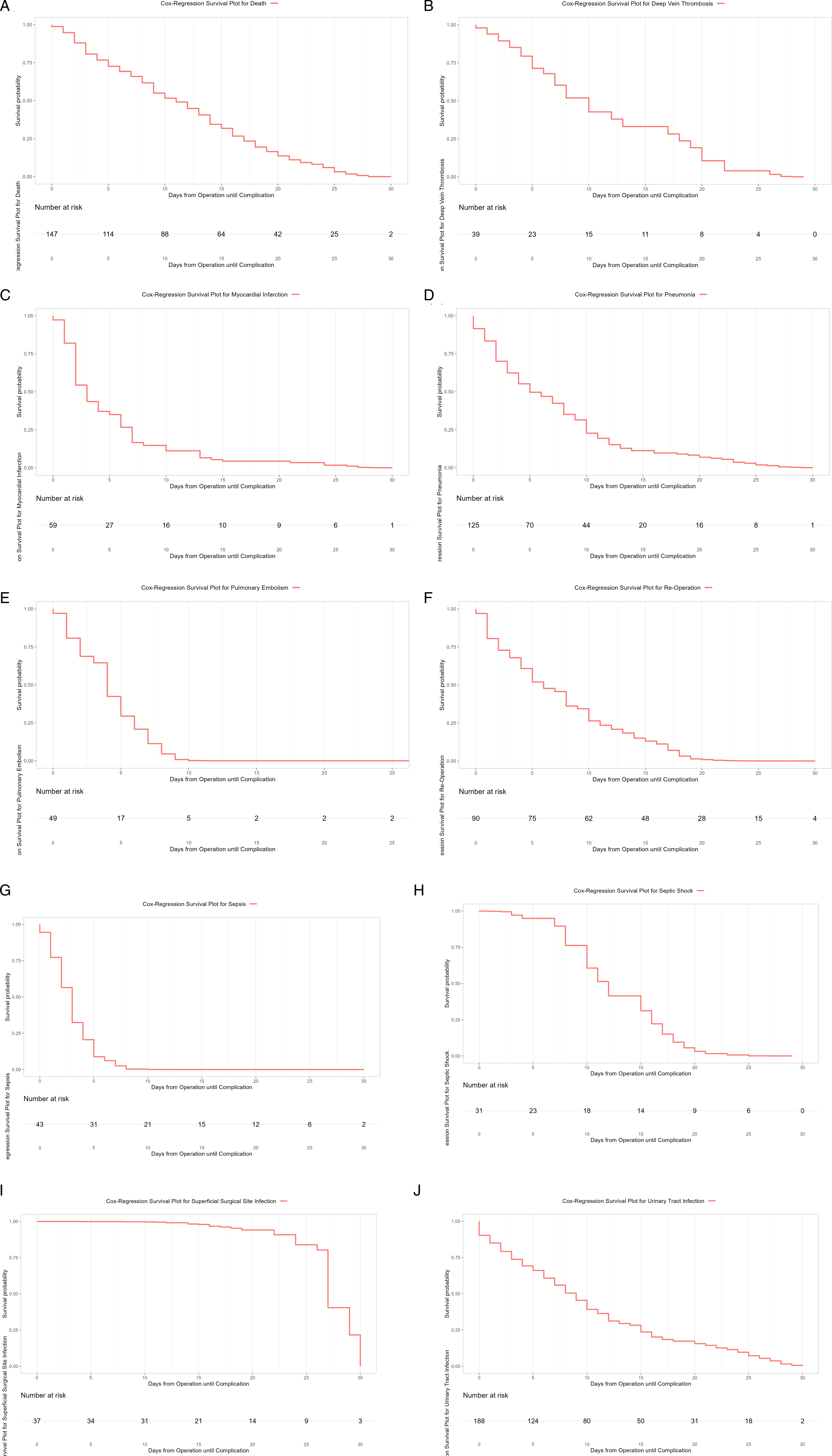
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.