
Abstract
Introduction
When performing intramedullary nailing for atypical femoral fractures (AFF), especially in lateral bowing femurs, a medial opening wedge-shaped gap in the fracture site may occur after nailing. We intended to analyse and compare clinical outcomes according to the medial gap in AFF cases after intramedullary nailing.
Keywords
Introduction
Atypical femoral fracture (AFF) has several unique characteristics that are distinct from usual femoral fractures. 1 It is important to understand the characteristics of AFF morphologically and biologically to treat them appropriately.1,2
The mainstay of treatment of complete AFF is surgical fixation of the whole femur length using long intramedullary nails. 2 However, if a fracture occurs in the femur accompanied by bowing, intramedullary nailing is technically challenging. 3 In most cases of AFF with femoral bowing, anterolateral bowing is problematic, and a medial opening wedge-shaped gap can occur after the nailing due to a mismatch between the nail and the femur geometry.4,5 Several studies have reported useful surgical methods to overcome this problem.6-9 Although several skilful tips have been reported, there is a lack of research regarding whether clinical results differ according to the occurrence of the medial gap.
We hypothesised that there would be a difference in post-operative outcomes according to the occurrence of the medial gap in AFF. In the present study, we analysed and compared radiologic and functional outcomes according to the medial gap in AFF cases treated by nailing.
Materials and Methods
After obtaining the approval of the Institutional Review Board of our institute, electronic medical records and radiographic images of 38 consecutive patients who underwent intramedullary nailing for complete AFF from December 2018 to March 2021 were retrospectively reviewed. The diagnosis of AFF was based on the diagnostic criteria of the American Society of Bone and Mineral Research. 1 Of the 38 patients, those who could be followed up for more than 12 months were included in the final study. Even if follow-up time was less than 12 months, if it was judged that the treatment for the fracture was completed by achieving bone union and restoring the pre-operative level of ambulation before the fracture, these patients were included in the study subject. In total, 22 patients were included in the study.
Surgical Technique and Post-operative Protocol
The surgery was performed by a single surgeon who is specialised in orthopaedic trauma surgery. The patient was placed on the fracture table under general or spinal anaesthesia, and closed reduction and internal fixation using intramedullary nails were performed in the usual manner. A total of 3 laterally bent nails at proximal area were used: Expert A2FN (Synthes, Oberdorf, Switzerland), Gamma3 Long Nail (Stryker, Schönkirchen, Germany) and Femoral Recon Nail (FRN) (Synthes, Oberdorf, Switzerland). The nail was inserted from the tip of the greater trochanter according to the usual procedure. Considering the morphology of the patient’s femur and the size of the targeted nail, the nail was inserted after over-reaming by 1–2 mm according to the operator’s judgement, if necessary. The nail was inserted using manual force, not a hammer, and if it was not inserted well, additional reaming was performed serially in units of .5 mm and repeated attempts were made.
Because of the biomechanical fragility of AFF,1,2 careful consideration of the biomechanical aspect was emphasised during the entire surgical procedure. Additional biological damage was minimised by refraining from incising and direct manipulation of the fracture site. In terms of stability, although proximal interlocking screws to the femoral head and distal interlocking screws in the mediolateral direction were routinely used, additional blocking screws 10 or multi-axial interlocking screws were inserted when stability was judged to be insufficient. In addition, even if the medial gap occurred, in order to minimise distraction in the vertical direction of the fracture, after fixing the proximal interlocking screws to the femoral head, the fracture site was sufficiently compressed before fixing the distal interlocking screws.
From the first day after the surgery, wheelchair mobilisation was started, and from the second day, ambulatory rehabilitation was performed within tolerable range using a walker. For approximately 2 months after the surgery, walking using a walker or cane was recommended; later, if the patient could tolerate it, independent ambulation without walking aids was allowed. From a pharmacological point of view, the previous use of bisphosphonates was stopped. Daily teriparatide injection was used if deemed necessary to maintain osteoporosis medication and if the patient could tolerate it.
Investigated Variables
Age, sex, height, weight, body mass index, the American Society of Anesthesiologists classification, 11 Charlson comorbidity index, 12 bone mineral density (BMD), prodromal symptom, medication of pre-operative bisphosphonates, pre-operative ambulatory ability (Koval grade) 13 and post-operative use of teriparatide were recorded. Fracture location and lateral femoral bowing grade were investigated as fracture characteristics. The fracture location was divided into 3 parts by referring to the AO Foundation/Orthopaedic Trauma Association classification. 14 The middle one-third was classified as isthmic fracture, and the proximal or distal one-third were classified as supra- or infra-isthmic (non-isthmic) fractures. Lateral femoral bowing was evaluated using a simple radiograph of the anteroposterior view of the contralateral femur, and the classification method suggested by Park et al. was used. 8
Evaluation of Post-operative Clinical Outcomes
In anteroposterior and lateral simple radiographs taken immediately after the surgery, medial, lateral, posterior and anterior gaps at the fracture site were measured, and the ratios between medial and lateral gaps and between posterior and anterior gaps were defined as ML gap ratio and PA gap ratio, respectively Figure 1. The mechanical axis of the lower limb was evaluated on the hip–knee–ankle (HKA) angle using whole lower limb anteroposterior teleoroentgenogram image taken in a standing position at least 3 months after the surgery. In addition, leg length discrepancy (LLD) was also evaluated in the whole lower limb image Figure 2. In terms of bone union, when bone bridges were formed in at least 3 cortices in both anteroposterior and lateral simple radiographs, it was deemed that bone union was established. In addition, the Radiographic Union Score for Tibial fractures in the last follow-up was used to evaluate the degree of radiographic bone union.
15
For functional evaluation, ambulatory ability was evaluated through Koval grade at the last follow-up. In atypical femoral fracture with anterolateral bowing, a medial and posterior opening wedge-shaped gap at the fracture site is confirmed after performing intramedullary nailing (A, B). In anteroposterior and lateral simple radiographs, medial (a), lateral (b), posterior (c) and anterior (d) gaps at the fracture site were measured (C, D). The ML gap ratio was defined as a/b, and PA gap ratio was defined as c/d. In a standing anteroposterior whole lower limb teleoroentgenogram, the hip-knee-ankle (HKA) angles were measured on both sides (α and β, A). The varus alignment was interpreted as a positive value, and the valgus alignment was interpreted as a negative value. The difference between the HKA angles on both sides (ΔHKA) was defined as the value obtained by subtracting the contralateral side from the fracture side (α−β). Leg length discrepancy was evaluated using the length from the tibia plafond to the upper end of the femoral head on both sides and was measured as a comparison; if the fracture side was long, it was interpreted as a positive value (B).

Statistical Analysis
Based on the ML gap ratio which indicated the degree of a medial opening wedge-shaped gap, the cases were divided into 2 groups: cases of ratio ≥3 were classified as the large medial gap (L-MG) group, and cases of ratio <3 were classified as the small medial gap (S-MG) group. The statistical comparison of the variables between the 2 groups was analysed using SPSS 21.0 (SPSS, Inc., Chicago, IL, USA). The Mann–Whitney U test was used to compare continuous variables, and Fisher’s exact test was used to compare dichotomous or trichotomous variables. When the P value was <.05, it was considered that there was a statistically significant difference.
Results
Patient and fracture characteristics.

BMI, body mass index; ASA, the American Society of Anesthesiologists classification; CCI, Charlson comorbidity index; BMD, bone mineral density; BP, bisphosphonate. All continuous variables were described as means [range].
In terms of fracture characteristics, the rate of isthmic fractures was significantly higher in L-MG group, and the severity of bowing was also significantly higher (Table 1). The mean degree of over-reaming was 1.7 mm (range, 1.5–2.5, n = 15), and the mean over-reaming was significantly different between the 2 groups (2.1 mm [range, 1.5–2.5, n = 8] vs 1.4 mm [range, 1–2, n = 7], P = .006). Except for 7 patients of previous total knee arthroplasty, the HKA angle of the contralateral normal side showed a significant difference between 9 patients with femoral bowing of grade 0 or 1 and 6 patients with grade 2 or 3 (1.9° [range, −5–8] vs 8.3° [range, 5–11], P = .003). That is, in the cases of severe lateral femoral bowing, there was a tendency towards more varus lower limb alignment.
Post-operative clinical outcomes.

HKA, hip-knee-ankle; ΔHKA, HKA angle of the fracture side–HKA angle of the contralateral side; RUST, Radiographic Union Score for Tibial fractures; LLD, leg length discrepancy; ΔKoval grade, Post-operative Koval grade–Pre-operative Koval grade. All continuous variables were described as means [range].
Bone union was confirmed in all patients, and the mean duration for bone union was 5.5 months (range, 3–10). There was no significant difference in bone union time between the 2 groups (5.4 months vs 5.6 months, P = .628). In terms of functional outcomes, there was no significant difference in the recovery of ambulatory ability (Table 2).
In one patient with an isthmic fracture in the S-MG group, a distal interlocking screw was pulled out at post-operative 2 months, and stability was strengthened by removing the screw and fixing blocking screws and an interlocking screw in the anteroposterior direction to the distal portion. Bone union was confirmed 4 months after the second operation.
Discussion
Although it is challenging to perform intramedullary nailing in complete AFF accompanied by anterolateral bowing, various surgical tips such as using the opposite nail, lateral entry nailing and external rotation of the nail have been introduced to overcome these difficulties.6-9 In fact, the clinical results in these previous clinical studies have been favourable. All these studies attempted to reduce the wedge-shaped gap and to restore the original shape of the femur. However, in the experience of the authors of the present study, a certain amount of gap is often unavoidable, especially when bowing is severe. In this process, we questioned whether clinical results of the cases with a medial opening wedge-shaped gap would be different from a case without the gap. A comparative analysis was performed on whether clinical results differ according to the medial gap occurring at the fracture site in cases of intramedullary nailing for complete AFF. The present study provides a clinical comparative analysis according to the medial gap, with a comprehensive evaluation through the measurement of whole lower limb alignment rather than just the femur itself.
Results showed that bone union was successfully obtained in all cases regardless of the medial gap, and there was no significant difference between groups regarding the timing of the union. Lim et al. reported that anterior and lateral gap after performing intramedullary nailing for complete AFF is a factor associated with delayed union or nonunion, 16 and the study recommended avoiding distraction at the fracture site decreasing the anterior and lateral gap. The lateral side of the femur is a tensile side, especially in femurs accompanied by a lateral bowing, which can be exaggerated and vulnerable to bone healing; this is also recognised as one of the pathomechanisms of the AFF.17,18 On the other hand, the medial side is the compressive side on the femur, so even if there is some inevitable wedge-shaped opening gap in the compressive side on the premise of proper reduction without distraction on the tensile side, there seems to be no significant problem in terms of bone union.
To assess the effect of the medial gap on functional aspect, it is necessary to evaluate the whole lower limb rather than just the femur. In terms of LLD, Shon et al. reported that the average LLD was measured by 5.7 mm after surgery in AFF with lateral bowing when the medial gap was reduced using the contralateral side nail. 9 In the present study, the average leg length was increased by 3.6 mm after the surgery. However, there was no significant difference between the 2 groups in terms of LLD. In addition, despite the objective LLD in radiographic images, there were no cases where the patient subjectively perceived LLD and complained of discomfort. To evaluate the difference between the objective LLD and the patient’s perception, various confounding factors including gender, age, body status, spinal problem, etc. should be considered. 19
A wedge-shaped opening gap in lower limb long bone can also change mechanical lower limb alignment.
20
In fact, in cases of L-MG due to severe lateral bowing, lower limb alignment changed relatively to a more valgus pattern post-operatively as the femur was straightened. However, in most cases with lateral bowing, the patient’s own lower limb alignment showed varus alignment; in contrast, the straightening of the femur after the surgery was closer to neutral alignment than the existing condition. In terms of lower limb alignment, it can be interpreted as a change towards a more ideal direction.21,22 Even so, if neutral alignment is maintained after previous total knee arthroplasty, the alignment might change to valgus alignment after intramedullary nailing for AFF with lateral bowing, which may adversely affect the long-term prognosis of prosthetic knee due to coronal malalignment Figure 3.
23
Therefore, in these cases, if information on the alignment can be obtained before nailing, it should be checked and considered in pre-operative planning. If patients have a neutral lower limb alignment after previous total knee arthroplasty, it would be appropriate to maintain the patients’ own femoral geometry without creating a wedge-shaped opening gap when addressing the alignment. A 71-year-old female patient with a laterally bowed femur had maintained neutral lower limb alignment after previous total knee arthroplasty (A). Due to an atypical femoral fracture of her right femur isthmus area, intramedullary nailing was performed. After the nailing, straightening of the femur with a medial opening wedge-shaped gap occurred, and lower limb alignment of right side showed valgus alignment at post-operative 5 months (B).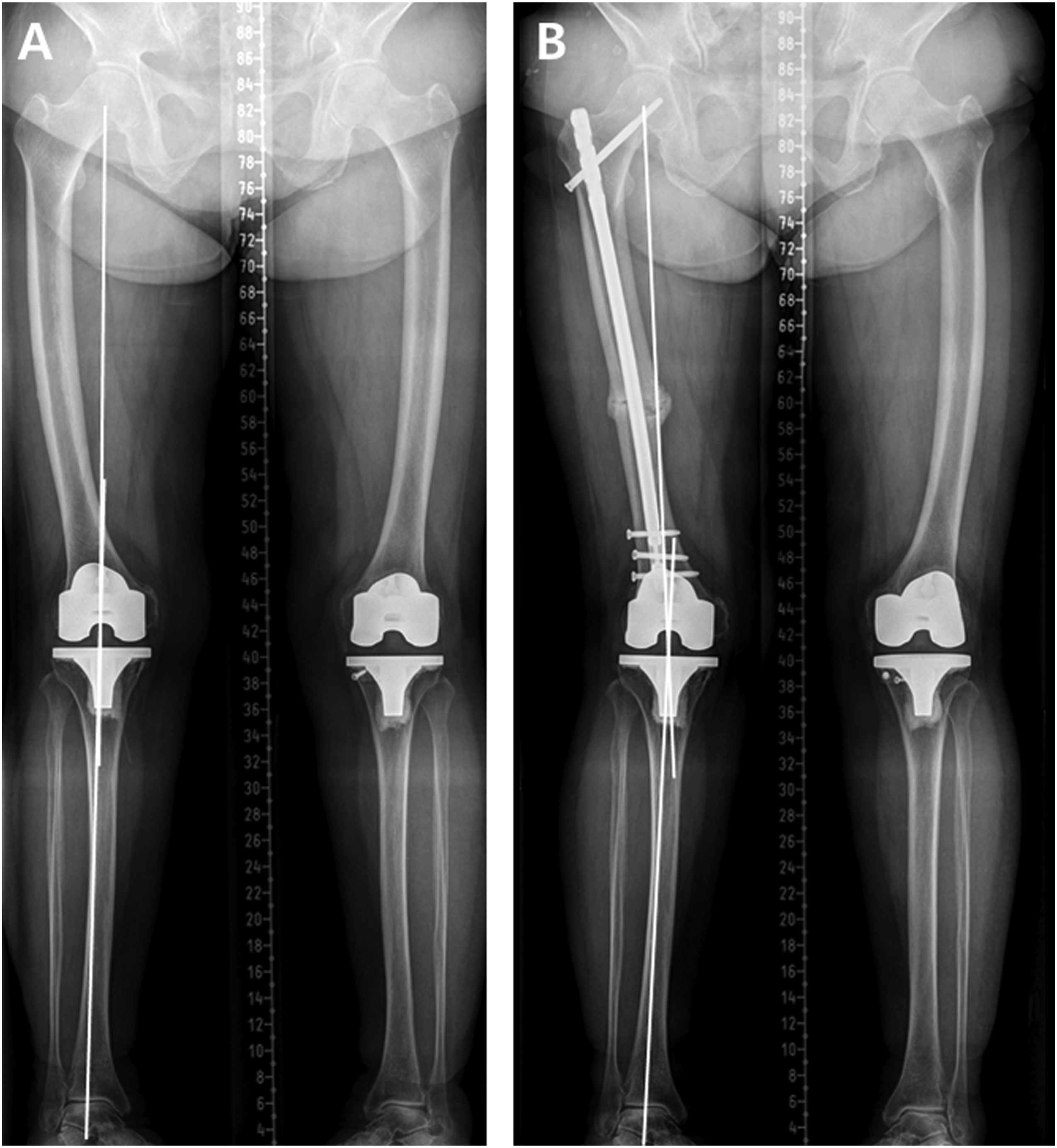
There are several limitations in the present study. First, it is a retrospective study with a small number of cases, which can also be attributed to the rarity of AFF itself. 24 However, the authors tried to maintain consistency with patients who were operated on by the same surgeon using the same procedure in a single centre. It is recommended that a larger, longer-term follow-up study is conducted for more reliable results in the future. Second, although lower limb alignment was evaluated, the long-term subsequent results were not evaluated, and the prognosis was indirectly estimated from existing research. As shown in the present study, as there are often patients with AFF who undergo previous total knee arthroplasty, it is also necessary to conduct a study on the long-term effect of the changed lower limb alignment on the prosthesis after treatment for AFF.
Conclusion
When performing intramedullary nailing in complete AFF with lateral bowing, bone union seems to be acceptable even if there is a medial opening wedge-shaped gap. In addition, in terms of LLD and lower limb alignment, the medial gap does not seem to have a significant adverse effect. However, if previous total knee arthroplasty is performed and neutral alignment is maintained, care should be taken as the occurrence of the gap may result in lower limb malalignments.
Footnotes
Author’s Note
This study was approved by the Institutional Review Board in our institute (KNUH-2021-08-025).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.