
Abstract
Objectives
To investigate the value of a post-operative gait training program to improve pelvic obliquity (PO) and decrease leg length discrepancy (LLD) for patients with Crowe type I developmental dysplasia of the hip (DDH) undergoing unilateral total hip arthroplasty (THA).
Methods
The prospective group consisted of 35 patients who underwent one-stage unilateral THA. Pre- and post-training PO and LLD were measured for the radiological assessment and Harris Hip Score (HHS) was used for the functional assessment.
Results
The HHS improved from 55.54 ± 10.61 pre-operatively to 84.97 ± 7.63 after surgery. The mean post-training PO angle for grade 0, grade 1, and grade 2 were 2.66 ± 1.42, 2.94 ± 1.42, and 5.60 ± 1.90, respectively, compared with pre-training values of 1.42 ± 0.58, 4.17 ± 0.90, and 6.96 ± 0.46. The mean post-training LLD for grade 0, grade 1, and grade 2 were 0.83 ± 0.91, 0.56 ± 0.48, and 0.36 ± 0.30, respectively, compared with pre-training values of 0.70 ± 0.23, 1.25 ± 0.90, and 1.46 ± 1.60.
Conclusion
Gait training following unilateral THA can improve PO and decrease functional LLD in grade I DDH patients. This method may have moderate success for grade 0 DDH patients and provide limited benefit for grade II patients. Appropriate release of the soft tissues may be required for grade II DDH patients to obtain a better walking gait.
Keywords
Introduction
As one of the most common hip disorders, developmental dysplasia of the hip (DDH) influences the patient’s physiological and psychological status and even social interaction.1,2 As with late-stage osteoarthritis, THA is an excellent treatment option to help them relieve pain and improve hip function in those with DDH. 1 However, THA for these patients is even more challenging, as they have an increased chance of suffering from lower leg length discrepancy (LLD) after surgery.3,4
LLD is one of the most common complaints after THA. 4 Previous studies showed that LLD more than 1.5 cm can cause asymmetric gait, back pain, and even failure of the implants.5,6 LLD can be divided into supra-pelvic obliquity, intra-pelvic obliquity, and infra-pelvic reasons, and it can also be divided into bony and functional LLD.7,8 Bony LLD is also called true LLD, and it is a skeletal anomaly and an absolute discrepancy of the legs. Functional LLD is also called apparent LLD, and most LLD after THA surgery is functional. This type of discrepancy is caused by scoliosis or pelvic obliquity (PO). 8
PO may result from tightness of the soft tissues such as the capsule and gluteus medius muscle around the hip joint.8,9 During THA surgery, the femoral head was removed and part of the soft tissue was released, so we hypothesized that the functional PO could be corrected by gait training after THA in DDH patients.
Although several studies have shown that pre-operative strength or gait training can help DDH patients obtain better function and gait patterns, few studies have focused on gait training following THA.10–13 The purpose of this study was to evaluate the value of a post-operative gait training program to improve PO and LLD for Crowe type I DDH patients undergoing unilateral THA.
Materials and methods
From March 2011 to December 2016, one-stage unilateral THA procedures were performed on DDH patients at the First Affiliated Hospital of Guangzhou University of Traditional Chinese Medicine. This retrospective study was approved by the Ethics Committee of Guangzhou University of Traditional Chinese Medicine (no. 2019123) and followed the principles of the Declaration of Helsinki. All patients provided written informed consent. This group included unilateral DDH patients who suffered from hip dysfunction and pain. The exclusion criteria included previous invasive hip surgeries, tumors, scoliosis, hip infections, inability to follow post-operative training programs, and flexion or extension contractures.
Surgical procedures and prosthesis
One surgical team and Dr. Zeng Yirong performed the hip replacements under combined spinal-epidural anesthesia. The standard posterolateral approach was used for all patients. All patients were recommended a LINK (Hamburg, Germany) cementless prosthesis. We claimed no financial support for our study. In one patient a S-ROM stem was used, in 15 patients ribbed stems were used, and in 19 patients LCU stems were used. No patients required a subtrochanteric femoral shortening osteotomy.
Gait training following THA
All of the patients scheduled for THA were trained to use the walker under the guidance of one well-trained doctor the day before surgery because it is easier to learn how to walk pre-operatively than immediately after a THA. All patients took part in the true gait training program 24 hours after the operation. After the surgery, isometric contraction of the quadriceps muscles was encouraged immediately, and full weight-bearing was allowed starting the day after surgery with a walker in all cases. Patients were stood upright to ensure vertical alignment of the body and avoid angulation towards the non-operative side. After moving the walker one step, patients raised the non-operative leg, kept the knee flexed to 90 degrees and held it for 3 seconds, then moved the walker another step, raised the operative leg, and kept the knee flexed to 90 degrees and held it for another 3 seconds (Figure 1). Patients repeated this cycle 20 to 30 times during every training procedure. It is essential to ensure that the patients maintain a vertical posture and avoid inclining towards the non-operative side in both the standing and walking phases. All patients took part in the walking rebuilding program 3 to 6 times every 24 hours during their hospitalization. One month after surgery, patients were encouraged to practice without the walker and to climb stairs 6 weeks after THA under the guidance of the doctor.

A 60-year-old patient completed the gait training program with a walker.
Radiological measurements and HHS scores
Pre- and post-operative pelvic anteroposterior x-rays were used for radiological measurements. The PO angles were measured as described in previous studies. 14 A line connecting the iliac crests was drawn and another line was drawn along the bottom of the fourth lumbar vertebra. The angle between these two lines was measured as the PO angle (Figure 2). An angle ≥3 degrees was considered PO positive. We divided the PO angle into three grades. An angle of less than 3 degrees was considered grade 0, between 3 and 6 degrees was considered grade I, and more than 6 degrees was considered grade II. The LLD was measured as described previously. 15 Briefly, the trans-teardrop line was drawn and the perpendicular distance from the lesser trochanter to the inter-teardrop line was measured, and the difference between the two sides was the anatomical LLD (Figure 2). Both the LLD and PO were measured three times by different researchers and the average value was used. Pre-and post-operative HHS scores were used to assess their functional results.

Anteroposterior image of a patient illustrating how the PO and anatomical LLD are measured. A line connecting the iliac crests was drawn (ab), and another line was drawn along the bottom of the fourth lumbar vertebra (ac). The angle between ab and ac was measured as the PO angle. The trans-tear drop line was drawn (AB), the tip of lesser trochanter was marked (C,D), and the difference in perpendicular distance between CAB and DAB was the LLD. PO, pelvic obliquity; LLD, leg length discrepancy.
Statistical analysis
Functional improvement of HHS scores was analyzed using the Wilcoxon test and the Mann–Whitney U test for inter-group pre-operative baseline and post-operative difference analysis. The demographic continuous data were described as mean ± SD. All data were processed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA) and a P-value less than 0.05 was considered statistically significant.
Results
Overall, 35 patients with unilateral DDH were included. According to our PO grade classification, 13 patients were grade 0, 17 patients were grade 1, and 5 patients were grade 2. The HHS improved from 55.54 ± 10.61 pre-operatively to 84.97 ±7.63 after surgery (P < 0.05) (Table 1). The mean post-training PO angle for grade 0, grade 1, and grade 2 was 2.66 ± 1.42, 2.94 ± 1.42, and 5.60 ± 1.90, respectively, compared with 1.42 ± 0.58,4.17 ± 0.90, and 6.96 ± 0.46 pre-training (P < 0.05, P < 0.05, P = 0.3413) (Table 2). The mean post-training LLD for grade 0, grade 1, and grade 2 were 0.83 ± 0.91, 0.56 ± 0.48, and 0.36 ± 0.30, respectively, compared with 0.70 ± 0.23, 1.25 ± 0.90, and 1.46 ± 1.60 pre-training (P = 0.62, P < 0.05, P = 0.08) (Table 3).
Pre- and post-operative HHS scores.

HHS, Harris Hip Score.
Pre- and post-training PO angle.
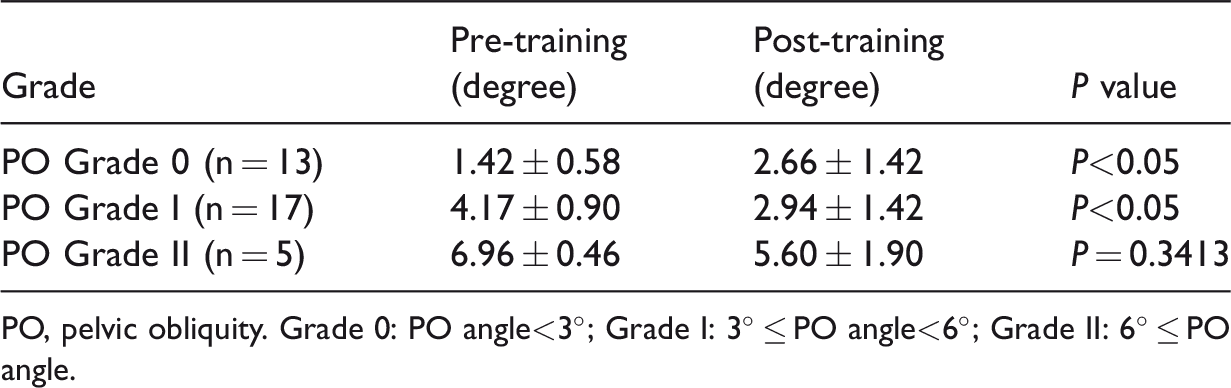
PO, pelvic obliquity. Grade 0: PO angle<3°; Grade I: 3° ≤ PO angle<6°; Grade II: 6° ≤ PO angle.
Pre- and post-training LLD.

LLD, leg length discrepancy.
The PO angle of the grade 0 group increased after training but was still less than 3 degrees, so we considered this group to be post-operative PO negative. The grade I group PO angle improved to negative after gait training because the elevated side of the pelvis was pulled down to a new balanced level during training. The PO angle of the grade II decreased, but there was no significant difference. Changes in the PO angle can affect functional LLD. The post-training LLD of the grade 0 group increased but there was no significant difference. For the grade I and grade II groups, their post-training LLD decreased, but there was no significant difference for the grade II group.
Discussions
In this research, we investigated the efficacy of gait training to improve post-operative PO and to decrease functional LLD for grade I DDH patients who underwent unilateral hip arthroplasty. This method may not be appropriate for grade II patients and it does not make the results of grade 0 patients better or worse. Moreover, the rehabilitation program and THA procedure all contributed to the improvement in post-operative HHS scores.
LLD following unilateral THA is usually functional because the bony deformities have been corrected during surgery. This type of LLD can be caused by several factors and PO acted as one of the most important reasons. 8 PO can be caused by the stiffness of the soft tissue between the femur and acetabulum.8,9 During the THA surgery, the femoral head was removed, and part of the soft tissue was released. The legs were equally lengthened after surgery, but the pelvis became unbalanced with the “longer” leg and patients had an asymmetric gait. We trained patients in order to pull the elevated side of the pelvis to the normal position during this procedure. In our study, the pre-training PO value of group 0 was negative. After training, the PO value increased but was still less than 3 degrees. Furthermore, post-training LLD did not increase significantly. We concluded that this method had a moderate effect on Crowe type I DDH patients. For the grade II group with PO more than 6 degrees, it was hard to correct this deformity with a rehabilitation program. The results indicated that appropriate release of the lateral and medial soft tissues may be required for grade II DDH patients to obtain a better walking gait.
Various types of techniques have been used to minimize post-THA LLD.16–18 These techniques are based on pre-operative planning and clinical or radiological measurements during surgery. Lakstein et al. 16 reported that careful pre-operative templating may reduce LLD in patients undergoing THA due to intracapsular hip fractures. Naito et al. 17 found that the intraoperative measurement using a Steinman pin and an adjustable caliper was more reliable than the Shuck test. Similar results were obtained by Shiramizu et al., 18 who concluded that this method was extremely accurate in predicting changes in limb length due to surgery. However, these techniques can predict LLD only before or during THA. Little is known about how to prevent post-operative LLD except for revision surgery. Gait training after surgery is one method to correct functional LLD.
Gait training for DDH patients is challenging, as it takes more time for them to get used to the “longer” leg and regain their walking ability. We trained all DDH patients pre-operatively because it is easier and more feasible for them to practice at this time. Although several studies have shown that pre-operative strength or gait training can help DDH patients increase function and strength,10,11 few studies have focused on gait training following THA. A study from Japan indicated that one walking assistive device can be used to improve early hip function and gait patterns for patients who underwent THA. 12 However, this research was a single-subject study and this training device is expensive and difficult for widespread use. Yoshikawa et al. 13 reported that wearable robot system training after knee arthroplasty can improve the gait and muscle strength compared with physical therapy, but this device is heavy and it is unclear whether it can be used in THA patients. In our study, we trained patients with the walker because it is cheaper and more feasible to complete the training program. Moreover, patients can hold the walker while walking in case of a fall in the early post-operative period. Last, patients can be re-trained easily with our method if they did the wrong procedure.
In this paper, post-operative HHS scores of the three groups increased significantly compared with the pre-operative baseline. The rehabilitation program and the THA procedure both contributed to the pain relief and hip function improvement. Our training program may help patients shorten their recovery time.
There were several limitations of this study. First, the surgical procedure may contribute to the change in post-operative radiological LLD. In most cases, lower leg length was judged by touching the bony landmarks such as the greater trochanter, patella, and heel, and this technique depends on the surgeon’s experience and is not accurate. Previous studies showed that intra-operative femur adduction or abduction can lead to a measurement error in leg length. We measured intra-operative LLD both in the lateral and supine positions by two doctors to minimize this bias. Second, this work was a retrospective study and the sample size was relatively small. Because of the relatively low incidence after THA, there were only five cases included in the PO grade II group, and more cases are needed in future research. However, to our knowledge, this is the first study to evaluate the value of post-THA gait training to improve PO and decrease LLD for Crowe type I DDH patients. Finally, we did not use the lower leg full-length x-rays to exclude deformities of the femur and tibia. As reported by Zhang et al., 19 a small portion of unilateral DDH patients present with LLD that may be derived from both the femur and the tibia. We plan to investigate this in more detail in the future.
In conclusion, gait training following unilateral THA can improve PO and decrease functional LLD for grade I Crowe type I DDH patients. This method may have a moderate effect in grade 0 patients and may be limited in grade II patients. Appropriate release of the soft tissues may be required for grade II DDH patients to obtain a better walking gait.
Footnotes
Acknowledgement
We would like to show our appreciation for the Department of Orthopedics of the first affiliated hospital of Traditional Chinese Medicine of Guangzhou University.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study received financial support from the National Nature Science Fund of the People’s Republic of China (Grant number is 81273784).