
Abstract
Objective
To examine the imaging evidence of the use of percutaneous compression plate (PCCP) in promoting femoral neck fracture healing compared with cannulated screws (CS).
Methods
This retrospective study enrolled patients with femoral neck fractures undergoing internal fixation procedures. The patients were divided into a PCCP group and a CS group with imaging as the primary outcome and Harris hip score (HHS) as the secondary outcome.
Results
This study included 162 patients: 80 in the PCCP group and 82 in the CS group. There were no significant differences between the patients in their preoperative baseline characteristics. Patient follow-up ranged from 24–56 months (mean 30.7 months). Differences in reduction quality, screw slipping, neck shortening and avascular necrosis (AVN) were not significant between the two groups. There were significant differences between the treatment groups in bone absorption, nonunion, healing time, screw withdrawal and fixation failure in favour of the PCCP group. Postoperative HHS at 6 and 12 months were significantly better for the PCCP group than the CS group, but the differences were not significant at 24 months and last follow-up.
Conclusion
Stable internal fixation with dynamic compression was the key to PCCP promoting femoral neck fracture healing.
Keywords
Introduction
Femoral neck fractures account for 3.8% of all fractures and internal fixation in the primary treatment choice for physiologically younger and nondisplaced elderly patients. 1 , 2 However, there is still no consensus on the best internal fixation device to use. The reported incidence of nonunion and avascular necrosis (AVN) of the femoral head was 15–40% after conventional cannulated screws (CS) and dynamic hip screw (DHS),3–6 which may be related to the defects of traditional internal fixation devices. Recent reports from some surgeons suggest significantly improved treatment efficacy when femoral neck fractures are treated with new internal fixators such as the locking proximal anatomic femoral plate, Targon FN system, percutaneous compression plate (PCCP) and the femoral neck system (FNS).7–11 Among these devices, PCCP had the least reported incidence of nonunion complications (1%–2%).7–11 However, the mechanism and imaging evidence for the use of PCCP in promoting femoral neck fracture healing with few nonunions has not been appropriately reported. The objective of this current study was to explore the imaging evidence of PCCP use in promoting femoral neck fracture healing relative to the use of CS.
Patients and methods
Study population
This study was a retrospective review of prospectively collected data at two level 1 trauma centres: Department of Orthopaedics, Wuxi No. 9 People’s Hospital Affiliated to Soochow University, Wuxi, Jiangsu Province, China and Department of Orthopaedics, Jiangnan University Affiliated Hospital, Wuxi, Jiangsu Province, China. Data were collected from all consecutive patients that sustained femoral neck fractures treated with internal fixation between June 2010 and December 2018. The inclusion criteria were as follows: (i) age ≥50 years; (ii) recent femoral neck fractures; (iii) repaired via closed reduction and internal fixation; (iv) no history of hip disease; (v) fixation before 2014 using CS and fixation after 2014 using PCCP; (vi) duration of follow-up > 2 years. The exclusion criteria were as follows: (i) incomplete fractures; (ii) incomplete case or imaging data; (iii) old or pathological fractures; (iv) bilateral fractures; (v) postoperative hormone use. Patients meeting the inclusion criteria were included in either the PCCP group and or the CS (control) group. All patients underwent X-ray and/or computed tomography (CT) scanning of the affected limbs. The demographic characteristics and clinical profiles including age, sex, fracture type (Garden classification), course (time from injury to surgery), Singh index, fracture side and co-existing diseases were recorded.
The study was approved by the Ethics Committees of Wuxi No. 9 People’s Hospital Affiliated to Soochow University (no. YN-0020057) and Jiangnan University Affiliated Hospital (no. JN-202000145). The study was performed in accordance with the Declaration of Helsinki with written informed consent obtained from each patient covering their participation and publication of any potentially identifiable images or data included in this article.
Surgical procedure and postoperative protocol
On admission to hospital, tibial tubercle or skin traction was performed in patients with displaced fractures. T-sharps were used in patients with non-displaced fractures. After general or spinal anaesthesia, the patients were placed in the supine position on a traction table. Standard anteroposterior and lateral images were obtained by C-arm fluoroscopy to confirm fracture reduction and internal fixator placement. For displaced fractures, satisfactory reduction can usually be achieved via longitudinal traction and internal rotation. An X-ray was taken immediately after the operation.
For the CS group, three K-wires, parallel and inverted as possible, were inserted into the femoral neck and head under C-arm fluoroscopy. Then three hollow compression screws were placed through a small incision among the K-wires. Patients were confined to rehabilitation in bed for 6 weeks, then ambulated with crutches, and partial weight bearing was permitted for another 6 postoperative weeks according to specific conditions. Those with poor newly-formed bone or loosening and failure of internal fixation were recommended to extend the non-weight-bearing period. Partial to full loading was added under professional guidance.
For the PCCP group, the PCCP plate was introduced to the lateral aspect of the femur after subperiosteal dissection through a 2-cm incision inferior to the greater trochanter. Thereafter a 3-cm distal incision of the plate was made and the plate was fixed to the femoral shaft with a bone hook. The distal neck screw was first placed near the calcar femoral, then, screws in the proximal, middle and distal areas of the femoral shaft were placed, and finally the proximal neck screw was fixed. Patients were instructed to ambulate with walking sticks or a walker within 3 days of surgery. This was followed by a gradual increase to full weight bearing by postoperative 1–2 months. The partial weight-bearing time for patient with displaced Garden type IV or Pauwels type III fractures was limited in the early recovery stage (< 2 h/day).
Postoperative follow-up
All patients received an initial monthly follow-up to assess fracture healing and thereafter every 3 months until 1 year when follow-up intervals were increased to 6 months. X-ray examination was routinely performed each follow-up. When it was difficult to judge fracture healing on an X-ray and the patient complained of coxalgia or X-ray films showed suspicious abnormal changes, timely CT and/or magnetic resonance imaging (MRI) examinations were undertaken. Clinical and radiological evidence was available for each patient included in the study.
Evaluation of femoral neck fracture healing
Healing of the femoral neck fracture in each patient was evaluated using the following measures: (i) reduction quality was defined as previously described using the Garden alignment index from 1 week postoperative as determined from the X-ray examination; 12 (ii) bone resorption was defined as widening of the gap at the fracture site or obvious fracture as determined from the X-ray examination; (iii) screw slipping was defined as the screw tip had slipped >2 mm toward the cortex of the lateral side of the femoral shaft as determined from the X-ray examination; (iv) screw withdrawal was defined as the head of the screw had slipped out > 2 mm from the cortex of the lateral side of the femoral shaft as determined from the X-ray examination; (v) neck shortening was defined as the distance between the tip of the femoral head and the caudal end of the lesser trochanter had shortened ≥ 5 mm on the affected side compared with the opposite side as determined from the X-ray examination; (vi) nonunion was defined as persistence of a fracture line more than 8 months after surgery; (vii) fixation failure involved obvious displacement or hip varus at the fracture site (displacement parallel to the fracture line ≥2 mm or angle ≥10°); 11 (viii) AVN was based on the 2012 Chinese adult expert consensus guidelines; 13 (ix) functional recovery was evaluated using the Harris hip score (HHS). 14
Statistical analyses
All statistical analyses were performed using the SPSS® statistical package, version 17.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Basic descriptive statistical analyses were used to describe the study population. For comparison between the two groups, Student’s t-test was used for continuous variables. χ2-test was used for categorical variables except when the expected counts were <5 when Fisher’s exact test was used. A P-value < 0.05 was considered statistically significant.
Results
This retrospective data analysis included 162 patients that met the inclusion criteria: 80 patients in the PCCP group and 82 patients in CS (control) group. Of these patients, 75 were further evaluated by CT and 26 cases were further evaluated by MRI. The preoperative baseline demographic and clinical data for the two groups are shown in Table 1. There were no significant differences in the preoperative baseline demographic and clinical data between the two groups. The mean ± SD operative times and intraoperative bleeding for the CS group were 1.12 ± 0.17 h (range 0.69–1.31 h) and 86.19 ± 12.28 ml (range 50–155 ml), respectively, compared with the PCCP group, which were 1.34 ± 0.17 h (range 0.85–1.63 h) and 126.19 ± 11.28 ml (range 85–305 ml), respectively. There were no significant differences in these two measures between the two groups.
Preoperative baseline demographic and clinical characteristics of the patients (n = 162) included in a study that examined the imaging evidence of the use of percutaneous compression plate (PCCP) compared with cannulated screws (CS) in promoting femoral neck fracture healing.

Data presented as mean ± SD or n of patients (%).
Continuous data were compared between the groups using Student’s t-test; and categorical variables were compared using χ2-test except when the expected counts were <5 when Fisher’s exact test was used; no significant between-group differences (P ≥ 0.05).
All patients received follow-up of their fracture healing for 24–56 months (mean 30.7 months). Reduction quality was scored as excellent and acceptable for 71 and 11 patients, respectively, in the CS group, while these scores were 68 and 12 cases, respectively, for the PCCP group (Table 2); with no significant differences between the two groups. Fractures healed in a mean ± SD of 5.04 ± 1.00 months in the CS group compared with a mean ± SD of 4.64 ± 0.74 months in the PCCP group (P = 0.034). There were 10 nonunion patients in the CS group, but none of the patients in the PCCP group had nonunion (P = 0.001). There were no significant differences in the incidence of screw slipping, neck shortening and AVN between the two groups. In contrast, bone absorption, screw withdrawal and fixation failure occurred in a significantly higher proportion of patients in the CS group compared with the PCCP group (P = 0.007; P = 0.016; P = 0.003, respectively). Among the 61 patients with neck shortening, 22 started from the surgical procedure and 39 after the rehabilitation; 14 cases were shorted by 6–10 mm, 17 by 11–15 mm, 12 by 16–19 mm and 18 by ≥20 mm. Among the 55 patients with complications, 26 had revision surgery, 25 patients of malunion and four patients with AVN (two in each group) were conservatively treated.
Comparison of the imaging findings between the two groups of patients (n = 162) included in a study that examined the imaging evidence of the use of percutaneous compression plate (PCCP) compared with cannulated screws (CS) in promoting femoral neck fracture healing.

Data presented as mean ± SD or n of patients (%).
aContinuous data were compared between the groups using Student’s t-test; and categorical variables were compared using χ2-test except when the expected counts were <5 when Fisher’s exact test was used; NS, no significant between-group difference (P ≥ 0.05).
The HHS for the PCCP group at 6 and 12 months postoperatively was significantly better than for the CS group (P < 0.001 for both comparisons) (Table 3). There were no significant differences in the HHS between the two groups at postoperative 24 months and the last follow-up. Representative patients are presented in Figures 1 and 2. The dynamic sliding compression ability of PCCP is shown in Figure 3.
Comparison of the Harris hip scores between the two groups at each postoperative time-point.
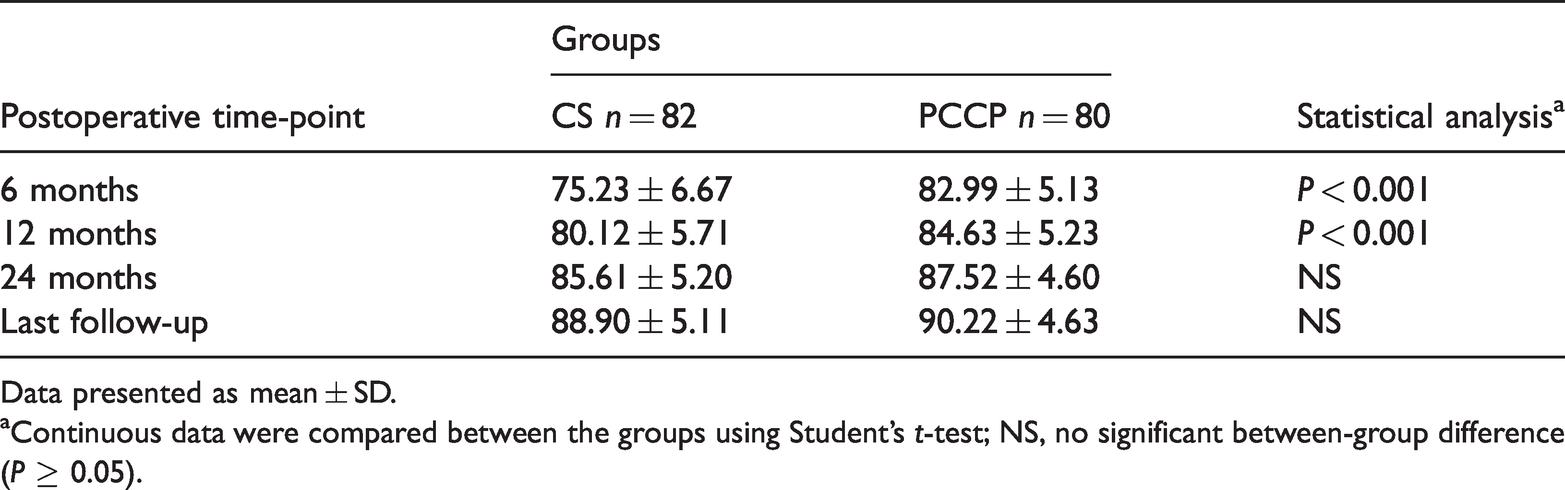
Data presented as mean ± SD.
aContinuous data were compared between the groups using Student’s t-test; NS, no significant between-group difference (P ≥ 0.05).
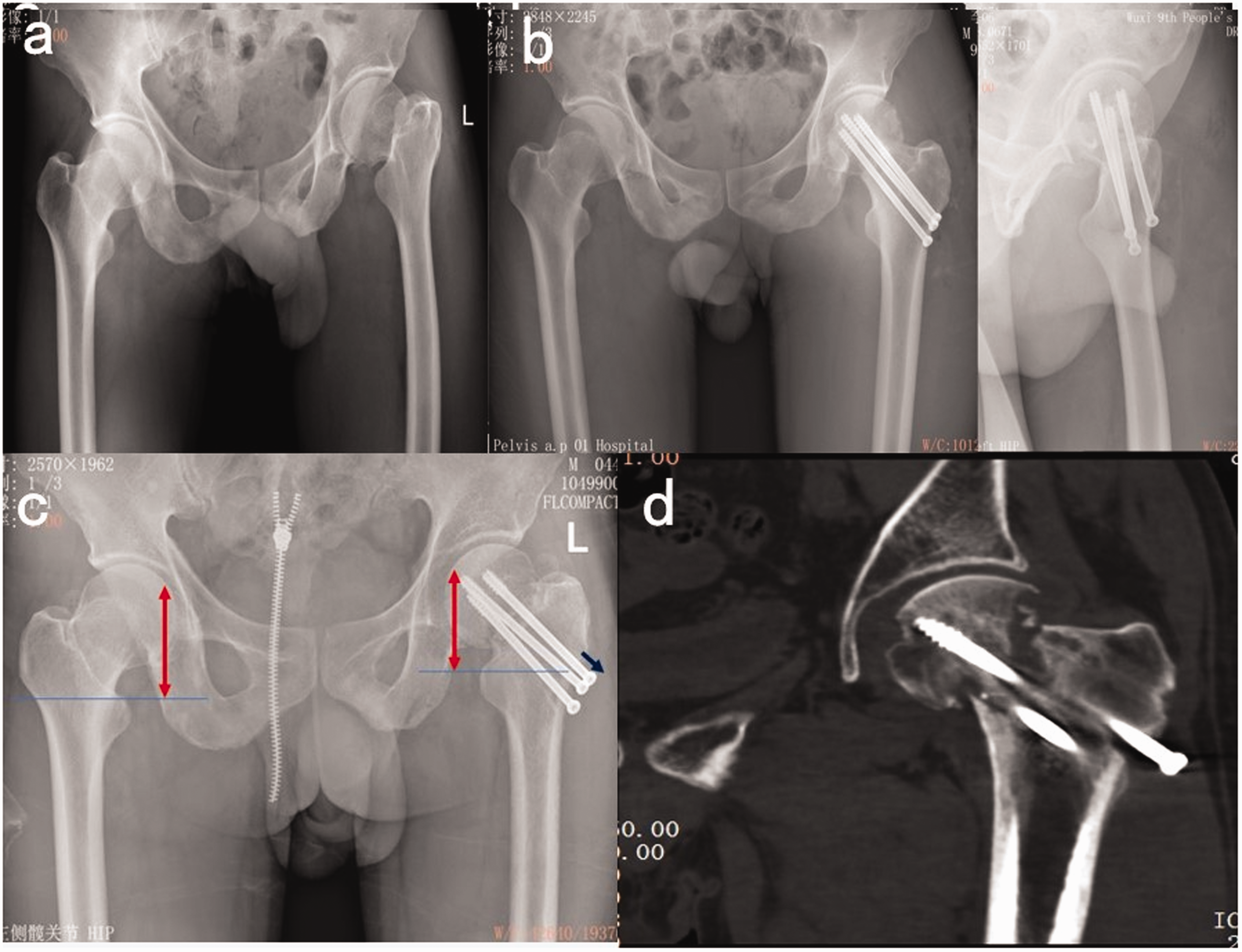
A 43-year-old male patient with femoral neck fractures fixed with cannulated screws: (a) preoperative X-ray showed left femoral neck fractures, Garden IV; (b) X-ray imaging showed excellent reduction quality at postoperative 2 weeks; (c) X-ray imaging showed neck shortening (red arrow), screw slipping and screw withdrawal (blue arrow), as well as nonunion at postoperative 6 months; (d) computed tomography showed neck shortening, screw slipping, screw withdrawal and nonunion at postoperative 9 months. The colour version of this figure is available at: http://imr.sagepub.com
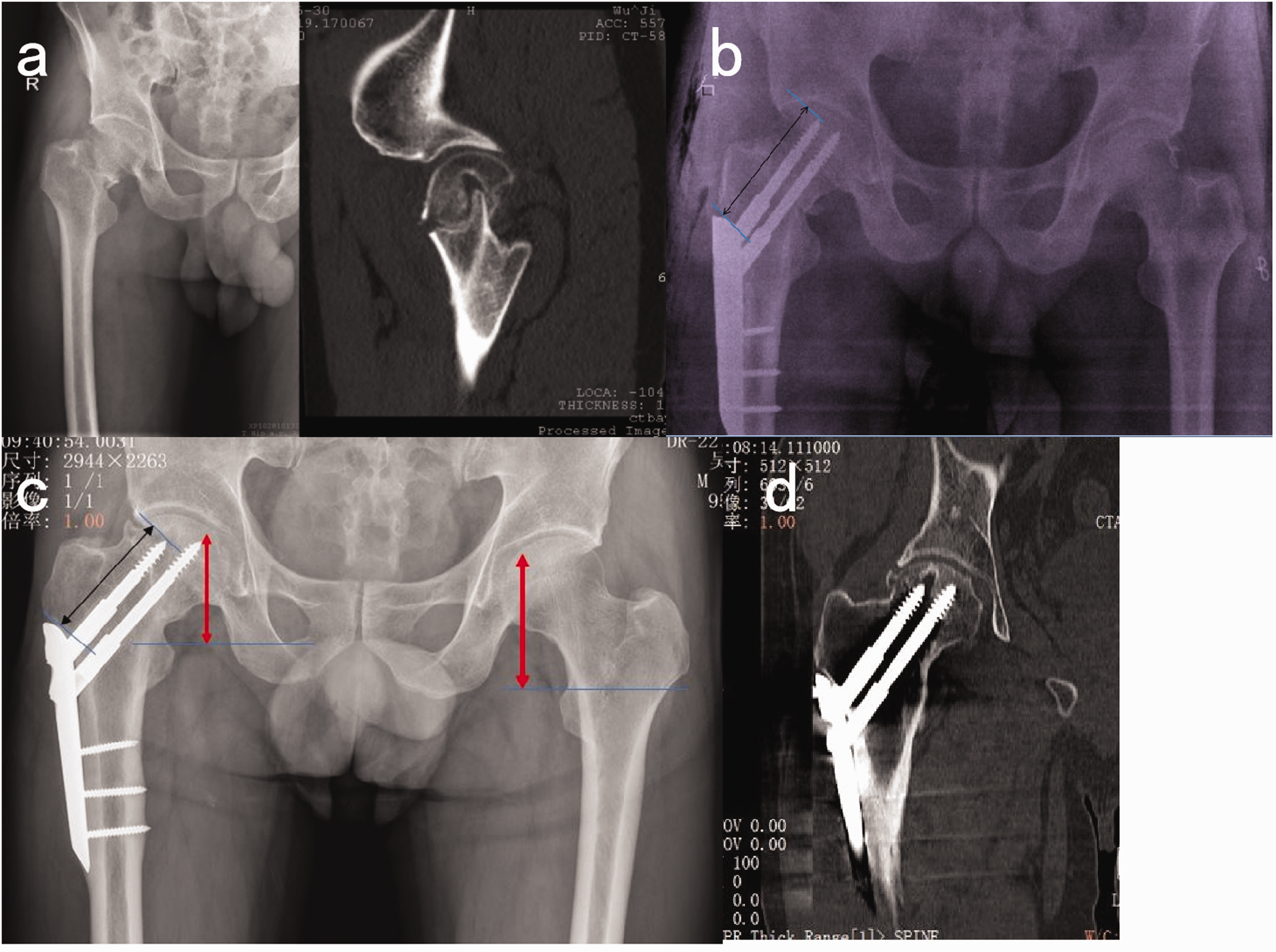
A 49-year-old male patient with femoral neck fractures fixed with percutaneous compression plate (PCCP): (a) preoperative X-ray and computed tomography (CT) imaging showed right femoral fractures, Garden IV; (b) X-ray imaging showed excellent reduction quality immediately after the operation fixed with PCCP; (c) X-ray imaging of screw slipping (black arrow) and shortened healing (red arrow) at postoperative 8 months; (d) CT scans of fracture healing at postoperative 18 months. The colour version of this figure is available at: http://imr.sagepub.com

Schematic diagram showing the dynamic sliding compression ability of a percutaneous compression plate.
Discussion
There are two kinds of healing phenomenon encountered after femoral neck fracture: non-shortening healing and shortening healing.15–17 For femoral neck fracture, the incidence of shortening healing (neck shortening) is high, which relates to the characteristic anatomical structure of the femoral neck involving mainly cancellous bone together with the mechanical environment.16,17 Regarding the latter, compression and resorption due to compression screw or contraction of muscles and the effects of gravity on the limbs at the fracture site are common, which make neck shortening common, especially in patients with osteoporosis and comminuted fractures.15,17 Indeed, shortening healing accounts for 17–65% of patients and is related to fracture type, sex, age, degree of osteoporosis, reduction quality and activity size. 5 ,15–17 In this current study, neck shortening was found to be similar in both treatment groups, accounting for 37.8% of CS patients and 37.5% of PCCP patients. Therefore, shortening healing is a common mechanism of femoral neck fracture healing and occurs independently of the internal fixation device used. Moreover, although the incidence of neck shortening can be considered high in the current study, neck shortening < 20 mm accounted for 70.5% of patients (43 of 61 patients), which was similar to that found previously. 15 The current study also found that limb functional recovery for most patients was not adversely affected by neck shortening.
The ideal internal fixator for a femoral neck fracture should have reliable stability to provide anti-compression, anti-shear and anti-rotation, as well as continuous dynamic compression ability. The former is conducive to postoperative early rehabilitation and weight-loading of patients, while the latter is conducive to fracture healing. 7 , 17 , 18 Although DHS also has dynamic compression ability, its anti-rotation stability is poor since there is only one sliding screw. PCCP has two thicker screws in the neck-head (φ7.5 mm) and an angular locking connection between the screw and plate. It not only has reliable stability in all directions, but also has dynamic compression ability. It has been reported that the composite force of anti-compression and anti-rotation of PCCP is superior to DHS and CS, i.e. all directional stability that guarantees postoperative rehabilitation and weight-bearing without fixation failure. 19 Furthermore, dynamic compression on the basis of stability can reduce the gap at the fracture site caused by bone absorption or a comminuted defect. 7 , 11 So although screw sliding and neck shortening both occur in PCCP, the incidence of bone absorption is relatively rare (Figure 3). 7 , 11 Therefore, the use of PCCP can always achieve satisfactory fracture healing and functional recovery in patients with comminuted or simple fractures, good or poor bone condition and excellent or accepted reduction quality. Consistent with this current study, three other studies including 149 patients have reported no incidence of nonunion or screw withdrawal in femoral neck fractures treated with PCCP.7,11,20
The current study demonstrated no significant differences in screw sliding and neck shortening between the two treatment groups. However, CS fixing lacks the holding force on the femoral shaft side as it has no screw thread. Once neck shortening occurs, the screw can slide out and loosen, making the fixation prone to failure. Therefore, CS has no reliable stability and stable dynamic compression ability, which functions against early postoperative weight bearing, affecting fracture healing or predisposing the fracture to nonunion. Nonetheless, CS can achieve satisfactory fixation in patients with good bone condition, stable fracture type and satisfactory reduction quality. 1 However, for patients with poor bone condition, unstable or comminuted fractures, bone absorption, early and excessive postoperative activity, CS cannot obtain a satisfactory fixation effect, and screw withdrawal and fixation failure are relatively common.11,20 Most CS patients were instructed to reduce rehabilitation activities or extend bed rest time, which resulted in closure difficulties, longer healing times or higher risk of nonunion, and unsatisfactory functional hip recovery. 3 , 5 , 6 Therefore, the healing time and healing rate in the CS applications were inferior to the PCCP group in the current study.
Following the application of PCCP, patients can undertake earlier postoperative rehabilitation and weight-bearing with less complications because it has better stability performance with a dynamic compression effect.11,20 In the current study, the HHS at postoperative 6 and 12 months for the PCCP group were significantly better than those for the CS group. Following revision surgeries for fixation failure and nonunion, the hip function improvements measured by HHS showed no significant differences between the two groups postoperatively at 24 months. There was also no significant difference in the prevalence of AVN between the two groups. Head necrosis is mainly related to the degree of fracture injury, type of fracture, reduction timing and head blood supply disorder,1–3, 21 but why the internal fixation method does not influence AVN remains unclear. Therefore, AVN of the femoral neck fracture remains unsolved.
This current study had several limitations. First, although it included patients from two hospitals, the number of patients was not very high so there may be bias. Secondly, the follow-up time was limited. Confirmation of these initial results therefore requires a multicentre investigation with long-term follow-up. Moreover, the PCCP device was constructed from stainless steel, which produces electrolytic reactions after long-term implantation and often needs to be removed. This construction also interferes with MRI examinations. PCCP devices are also comparatively expensive imports relative to either CS or DHS fixations.
In conclusion, stable internal fixation with dynamic compression was the key advantage of PCCP for promoting femoral neck fracture healing, especially in cases of shortening. However, PCCP does not significantly improved the prevalence of AVN.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211033501 - Supplemental material for Imaging observation of percutaneous compression plate use in promoting femoral neck fracture healing
Supplemental material, sj-pdf-1-imr-10.1177_03000605211033501 for Imaging observation of percutaneous compression plate use in promoting femoral neck fracture healing by Yong Chen, Haifeng Li, Liansheng Dai, Qudong Yin, Dong Li and Xinming Wang in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605211033501 - Supplemental material for Imaging observation of percutaneous compression plate use in promoting femoral neck fracture healing
Supplemental material, sj-pdf-2-imr-10.1177_03000605211033501 for Imaging observation of percutaneous compression plate use in promoting femoral neck fracture healing by Yong Chen, Haifeng Li, Liansheng Dai, Qudong Yin, Dong Li and Xinming Wang in Journal of International Medical Research
Footnotes
Author contributions
Yong Chen: validation, formal analysis, data curation, writing-review and editing; Haifeng Li: conceptualization, methodology, validation, formal analysis, investigation, data curation, writing-original draft, writing-review & editing, supervision, project administration; Liansheng Dai: conceptualization, resources, investigation, supervision; Qudong Yin: investigation, writing-review and editing, supervision; Dong Li: investigation, resources, data curation, writing-review & editing, supervision, project administration; Xinming Wang: conceptualization, investigation, writing-review and editing, formal analysis, supervision, project administration.
Acknowledgement
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.