
Abstract
Purpose
To analyze the clinical effect and imaging data of cementless bipolar hemiarthroplasty employing a long femoral stem (peerless-160) and 2 reconstructed femoral titanium wires to repair intertrochanteric fractures among the octogenarians.
Methods
Between June 2014 and August 2016, 58 octogenarians with femoral intertrochanteric fractures underwent the long femoral stem (peerless-160) cementless bipolar hemiarthroplasty by the same surgeon. We assessed clinical and radiological outcomes such as operative time, bleeding volume, blood transfusion volume, length of hospital stay, full weight-bearing walking time, walking ability calculated by Koval classification and Harris Hip Score (HHS), including fracture healing and greater trochanter fragments subsidence.
Result
The surgery was successfully performed in all patients. The average operation time was 72.8 ± 13.2 min, the average blood loss during surgery was 225.0 ± 91.4 mL, 200 mL of blood was transfused, the mean duration of hospitalization was 11.9 ± 4.0 days, the mean time of full weight bearing was 12.5 ± 3.8 days. Patients were followed up for 24-68 months, averagely 49.4 ± 10.3 months. During follow-up, 4 (6.9%) patients died, and 1 (1.7%) was completely lost to ask about the recent situation. The average Harris Hip Score at the last follow-up was 87.8 ± 6.1, most of the patients recovered walking ability, under radiological examination, the prosthesis showed no signs of loosening. All trochanteric fractures gradually healed, the clinical and radiographic signs of healing occurred at average of 4.0 ± 1.1 months postoperatively.
Conclusion
For osteoporotic unstable intertrochanteric fractures in octogenarians, this study confirmed that the Cementless Bipolar Hemiarthroplasty Using a Long Femoral stem (peerless-160) with double cross binding technique is a satisfactory and safe choice for the octogenarians.
Keywords
Introduction
Intertrochanteric fractures often occur in older adults; the number of hip fractures worldwide is projected to increase from 1.26 million in 1990 to 4.5 million in 2050. 1 The elderly population has osteoporosis and poor bone quality, muscle atrophy and weakness, even many elderly patients have unstable fractures and are bedridden. 2 Conservative treatment is less effective and has higher mortality. Intertrochanteric fractures surgical treatment in elderly patients is currently advocated. Intramedullary nail fixation such as proximal femoral nail antirotation (PFNA) or gamma nail (GN) is considered the “gold standard technique” for treating such fractures. 3 However, the management of unstable intertrochanteric fractures is a challenge because internal fixation is technically difficult, the sophisticated tools and superb surgical skills are necessary in PFNA operation. Moreover, When closed reduction is difficult to implement, it needs to be changed to open reduction, 4 nevertheless, elderly patients with severe osteoporosis are prone to complications such as non-union, implant failure, and loss of lag screw.5-8 Several recently syfemoralatic review and meta-analysis9-12 have shown the safety and effectiveness of hemiarthroplasty in the remedy of unstable intertrochanteric fractures in the elderly. But it is still not clear which conditions are most suitable for hemiarthroplasty. At the same time, how to choose a reasonable femoral stem prosthesis and reconstruction of femoral titanium are very important. The purpose of this research is to analyze the effect of cementless bipolar hemiarthroplasty using a long femoral stem (peerless-160) and 2 reconstructions femoral titanium wires for osteoporotic unstable intertrochanteric fractures among octogenarians.
Materials and Methods
Ethical Considerations
The author is responsible for all aspects of the work to ensure that issues relating to the accuracy and completeness of any part of the work are properly investigated and resolved, all the patients who participated in this procedure and their children were provided written informed consents for surgery in advance and agreed to publish their information in public. The Ethical Committee approved this presented study (Ethical approval ID: (2013-KL-012)). All methods were executed in according to the relevant guidelines and regulations.
Inclusion and Exclusion Criteria
Inclusion criteria: ① the patient was over 80 years old; ② with severe osteoporosis (Singh index ≤ grade 3 and T < −2.5 SD); ③ unstable intertrochanteric fracture (Evans-Jensen classification type III, IV, and V those were unstable types); 13 ④ coronal fracture fragment; ⑤ Patients and their families volunteered participation in this study.
Exclusion Criteria
① Pathological fracture such as metastatic tumor; ② Bilateral intertrochanteric fractures; ③ Age less than 80 years; ④ Stable fractures; ⑤ Unfit for anesthesia; ⑥ Dexa Scan Values T-score>2.5SD; ⑦ Patients unable to walk before the fracture; ⑧ Refuse the consent.
General Information
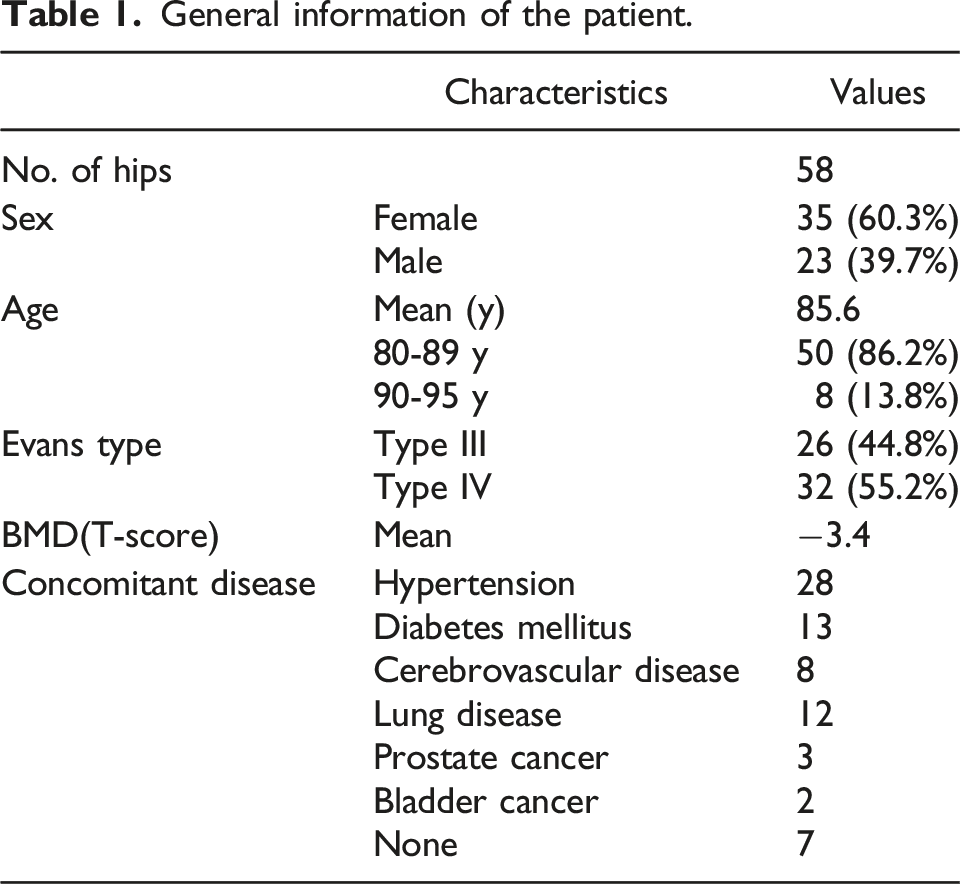
General information of the patient.
Implants
A cementless long-femoral design (peerless-160 femoral; CHUNLI, China) was used. The characteristics of the peerless-160 femoral (CHUNLI) (Figure 1) are: i The femoral is composed of plasma titanium microporous coating; ii Design of long longitudinal rib at the middle and far end to enhance the anti-rotation stability of the prosthesis; iii 130° neck femoral angle, narrow neck design, better mobility, less impact; iv It’s a 15 curve, not only reconstructs the original physiological curve of the femur, but also ensures the strength of the femoral stem prosthesis; v The overall length of the femoral ranges from 200 to 250 mm, and the diameter of the femoral ranges from 9 to 20 mm in 1-mm increments. Vi Proximal femoral stem perforated design, which convenient for the fixation of the great trochanteric fracture; vii The distal locking hole design of the prosthesis provides a more reliable fixation method and prevents the prosthesis from sinking. Viii This is a fully coated uncemented cylindrical stem that has bilateral cristae. And the bilateral cristae increase the rotational stability of the femoral stem. (Figure 2). A cementless long-handle design peerless-160 handle (CHUNLI). The distal locking hole design of the prosthesis.

The intertrochanteric fractures cause damage to the large and small femoral trochanter structure, thereby weakening the fixation of the proximal femur to the femoral stem. Using a long stem cylindrical prosthesis offers several advantages: it serves as intramedullary fixation for different degrees of bone defects, avoids stress concentration in the proximal femur, increases contact area with the bone marrow cavity, reduces the unit load on the femoral stem and bone, thereby compensating for the weakened fixation of the femoral stem to the proximal femur.
In cases of severe osteoporosis or when the femoral stem was deemed unstable during the operation, 2 locking screws could be implanted in the distal locking holes to prevent the femoral stem from sinking. Therefore, not all patients received 2 locking screws.
Operation Method
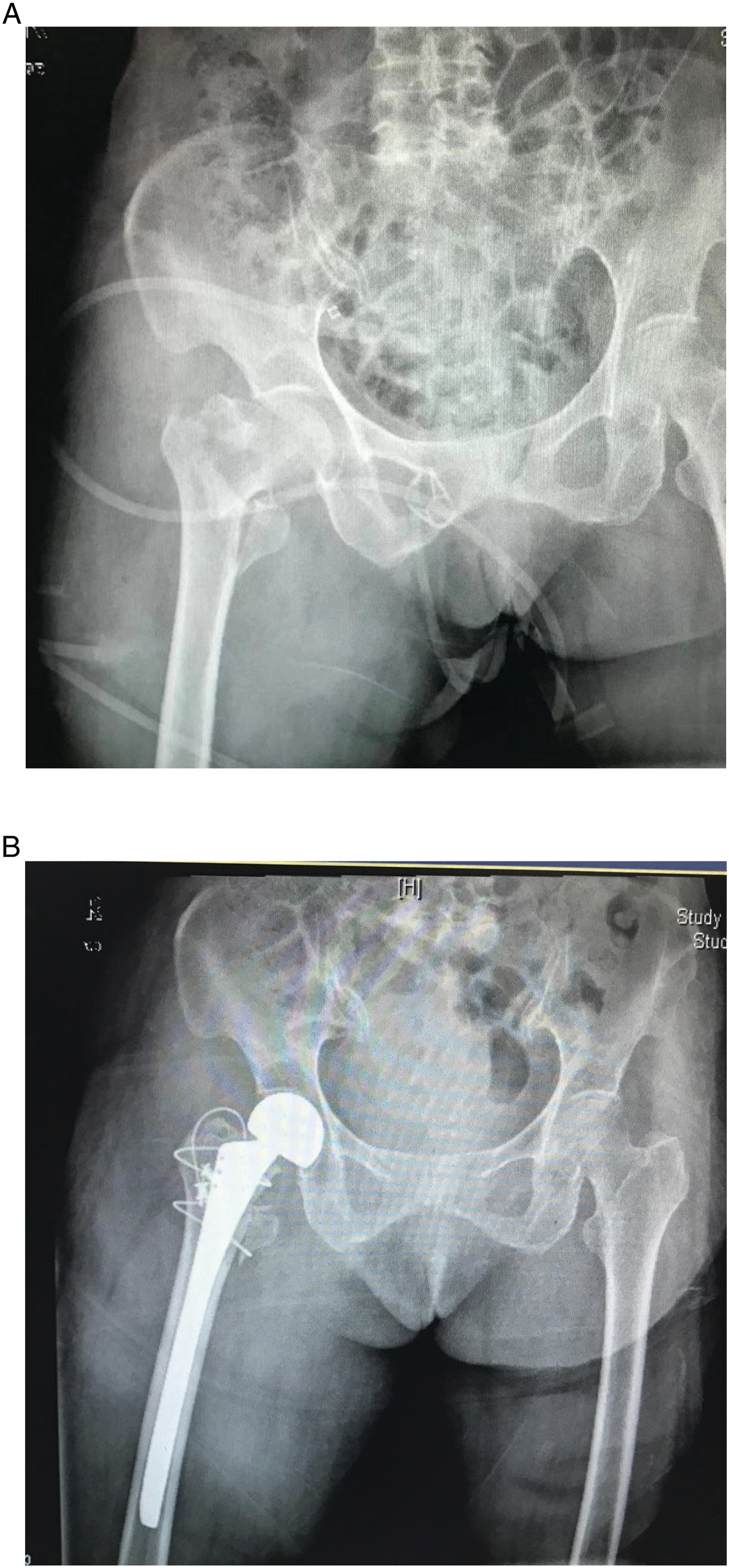
Under the spinal cord or general anesthesia, hip replacement is performed through a posterior approach, make a 10 cm posterolateral incision and cut the external rotator muscles to expose the femoral neck and fracture fragments. We use double cross binding technique to reposition the trochanteric fracture, the double cross binding fixation technique as follow: the semi-circular guide wire hook is used to guide the titanium cable. One piece is secured by a deep surface of the hip abductor around the lower margin of the lesser trochanter, which is shaped like the number 8 (Figure 3 The red dotted line), another piece is fixed by the transverse ring on the upper edge of the lesser trochanter (Figure 3 The red solid line) (Figure 4). First cut the femoral neck, the medullary cavity is then enlarged with tailor-made flexible reamers. Different flexible reamers have different diameters in .5 mm increments, until the medullary cavity reaches the desired size (flexible reamers is .5 mm larger than the prosthesis); then choose the diameter that corresponds to the prosthesis. After enlarging the medullary cavity, the femoral prosthesis model was selected. Trial reductions are then performed to check joint stability and motion, such as flexion, adduction and extension test. Then a suitable peerless-160 femoral is inserted, final tightening of the cable is performed and recheck the range of motion and stability after restoring. Repair the capsule and reconnect the short external rotator, then close the wound with a closed suction tub. The double cross binding fixation technique. (A) A preoperative X-ray of an 86-year-old woman with an Evans TYPE III intertrochanteric fracture (B) A preoperative X-ray of the hip after hemiarthroplasty use the double cross binding fixation technique with a peerless-160 handle.
In cases of severe osteoporosis or when the femoral stem was deemed unstable during the operation, 2 locking screws could be implanted in the distal locking holes to prevent the femoral stem from sinking. Therefore, not all patients received 2 locking screws.
Postoperative Treatment
Do quadriceps strengthening exercises from the day after surgery. The vacuum drain is removed after 48 h. We developed rehabilitation programs to teach patients on how to stand and walk correctly. They can walk with crutches or a weight-bearing walker the day after surgery.
Evaluation Methods
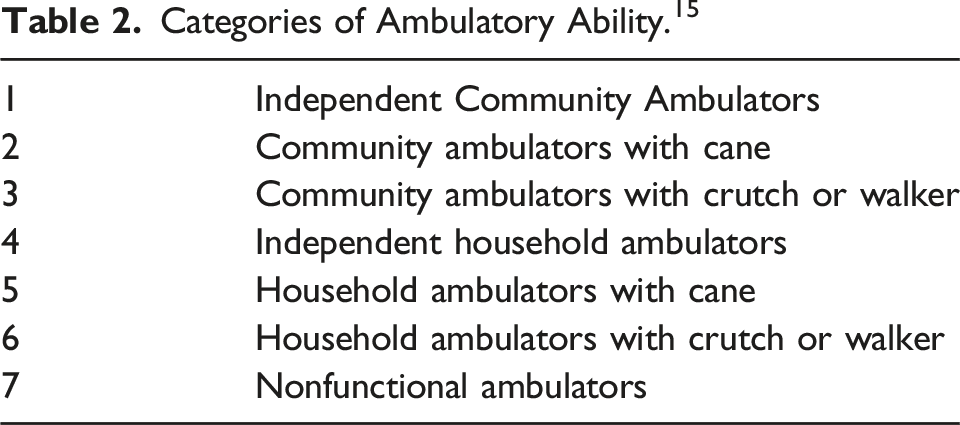
Categories of Ambulatory Ability. 15
Results
All patients underwent successful surgery, the average operative time was 72.8
Clinical Results
Patients were followed up for 24-68 months, averagely 49.4
Walking ability according to Koval’s categories 15 at the last follow-up,9 patients (17.0%) in 1 level, 12 patients (22.6%) in 2 level, 14 patients (26.4%)in 3 level, 12 patients (22.6%) in 4 level, 6 patients (11.3%) in 5 level.
Radiological Results
Radiological examination showed no loosening of the prosthesis. All trochanteric fractures had united, the signs of clinical and radiological healing were found at an average of 4.0
Case Presentation
An elderly woman developed an unstable intertrochanteric fracture with type III of left hip due to a fall (Figure 5) when she was 84 years old. The Dexa Scan Values T-score was −3.6. She was able to walk independently before the injury without any support and she had 2 concomitant diseases (hypertension and Diabetes mellitus). We performed bipolar hemiarthroplasty using the double cross binding fixation technique with a peerless-160 femoral 3 days after the injury. Two days after surgery, the walking exercise with a walker was started. One week after the operation, the X-ray showed that the fracture was reduced and the prosthesis was fixed well (Figure 6). One year after surgery, she was able to walk independently without any assistance. The X-rays taken 1 year (Figure 7(A)) and 3 years (Figure 7(B)) revealed that the bone union of the greater trochanter and the prosthesis were well fixed. An 84-year-old female preoperative anteroposterior radiograph with type III unstable. Immediate post operative X-ray. (A) X-ray one year after surgery shown bone union (B) X-ray of the third year after surgery shown bone union and the prosthesis was well fixed.


Discussion
The elderly people are prone to intertrochanteric fractures, most of which consist of unstable fracture, often comminuted and accompanied by severe osteoporosis, most cases of those patients with concomitant disease, such as Hypertension, Diabetes mellitus, Cerebrovascular disease, lung diseases and so on, so the intertrochanteric fractures have high morbidity and mortality rate.18,19 Intertrochanteric fractures surgical treatment in elderly patients is currently advocated, intramedullary nail fixation such as gamma nail (GN) or proximal femoral anti-rotation nail (PFNA) is considered the “gold standard technique” for treating such fractures. 3 However, the management of unstable intertrochanteric fractures remains challenging because of technically difficult internal fixation and, in cases where closed reduction is difficult to achieve, open reduction has to be performed. Besides, internal fixation which was not suitable for all types of fractures and still with high internal fixation failure rates.20,21 Some studies shown that octogenarians, 22 severe osteoporosis, 23 coronal fracture fragment, 24 the lateral femoral wall fracture, 25 quality of reduction 26 were main failure factors of internal fixation after PFNA treatment. Several recently review paper and meta-analysis9-12 have shown the safety and efficacy of hemi-replacement arthroplasty to treat the senile unstable intertrochanteric fractures, could reduce the implant complications and the chance of reoperation. However, it is still not clear which conditions are most suitable for semi-replacement joint replacement. So in current research the patients who were ① over 80 years old; ② with severe osteoporosis (Singh index ≤ grade 3 and T < −2.5 SD); ③ unstable intertrochanteric fracture (Evans-Jensen classification type III, IV, and V which were unstable types); ④ coronal fracture fragment. We performed bipolar hemiarthroplasty using the double cross binding fixation technique with a peerless-160 femoral. The aim of this study was to analyze the clinical effect and radiographic outcomes of consecutive series of peerless-160 femoral arthroplasties in patients with unstable intertrochanteric osteoporotic fractures with a mean follow-up of 49.4 months.
In this study, we use long femoral (peerless-160) and 2 wires reconstruction of femoral titanium to treat the intertrochanteric fractures in older adults with osteoporosis and achieved good short-term clinical effect and imaging results. The peerless-160 implantation is a kind of long-femoral femoral prosthesis composed of plasma titanium microporous coating that is designed for revision, the long longitudinal rib at the middle and far end to enhance the anti-rotation stability of the prosthesis, which has a good stable effect in both short and long term. According to HHS, 92.5% of patients in our group were very satisfied with the outcome of the surgery at the last follow-up. We recommend the biological long-femoral prosthesis to the elderly patients with intertrochanteric fractures. The reasons are as follows: Firstly, avoid excessive stress concentration at the proximal femur; Secondly, the proximal stable biological prosthesis loses its fixation function for osteoporotic unstable intertrochanteric fractures, which can only be achieved by distal fixation; thirdly, the long-femoral prosthesis can increase the contact area with the femoral bone marrow cavity and reduce the unit load of the prosthesis and bone; fourthly, peerless-160 femoral has proximal perforated design, which convenient for the fixation of the great trochanteric fracture (Figure 1) also the distal locking hole design of the prosthesis provides a more reliable fixation method and prevents the prosthesis from sinking (Figure 2); Finally, although some studies27-29 suggest that primary cemented hemiarthroplasty can also achieve good results in the treatment of unstable intertrochanteric fractures, while the use of cementless prostheses can avoid intraoperative cement reaction. Another concern is how to reduce and fix fractures of the greater or lesser trochanter. The gluteus minimums and gluteus medias, which are responsible for lower extremity abduction, attach to the greater trochanter of the femur. When these muscles are not adequately immobilized at the time of surgery, pain may persist, and the Trendelenburg gait may develop. Therefore, how to effectively and reliably reduce and fix fractures of the trochanteric has become 1 of the criteria to measure the success of surgery. Previously, screws, K-wires, steel wires, titanium wires, GTR devices, or trochanter hooks were commonly used to construct the greater trochanter. In this study, we use double cross binding technique to reposition the trochanteric fracture. The double cross binding technique has the following advantages. On the 1 hand, all the trochanteric fractures were bound in series. On the other hand, combined with the transverse ring of the upper edge of the lesser trochanter, the lateral tension band is produced, which plays an effective role in fixing all fracture pieces. After inserted the long-femoral prosthesis can further increase the fastness of strapping. And which can also reduce the incidence of trochanteric fracture displacement and bursitis. The goals to treat the unstable intertrochanteric fractures are pain relief, early ambulation, and recovery of the patient to pre-fracture levels of function. After arthroplasty, the greater and lesser trochanteric fractures healed well, the radiological examination showed no significant movement of the prosthesis, and the patient has no obvious pain. After undergoing arthroplasty. On the second postoperative day, we allowed the patient to walk with a crutch or a walker with an acceptable weight bearing. None of our patients with unstable fractures experienced nonunion or significant prosthesis subsidence due to early ambulation. At the last follow-up, the walking ability score of the patients was obtained according to Koval’s categories, 9 patients (17.0%) were in 1 level, 12 patients (22.6%) were in 2 level, 14 patients (26.4%) were in 3 level, 12 patients (22.6%) were in 4 level, 6 patients (11.3%) were in 5 level, which obviously enhance the patient’s quality of life.
Comparison of bipolar hemiarthroplasty for intertrochanteric fractures.

NR, not recorded.
Conclusion
For osteoporotic unstable intertrochanteric fractures in octogenarians, this study shows that Cementless Bipolar Hemiarthroplasty Using a Long femoral (peerless-160) and double cross binding technique is a satisfactory and safe choice.
Footnotes
Correction (June 2023):
Table 3 has been updated for minor changes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by 2023 Medical Rookie——He Bangjian (1S22317). Natural Science Foundation of Zhejiang Province (LY21H270008). National Natural Science Foundation of China (82074469). Study on the clinical experience of Hua Jiang Famous Traditional Chinese Medicine treating back and leg pain based on complex network (2023ZF019).
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study. The experiments comply with the current laws of the Country in which they were performed.
Data Availability
Data of this paper were retrieved in accordance with the Statement of human and animal rights.