
Abstract
Introduction:
Intertrochanteric (IT) femur fractures are common in elderly patients who are often in poor general health. Intertrochanteric fractures are classified as stable or unstable, taking into account fracture morphology and involvement of the posteromedial calcar. The purpose of this study is to determine whether IT fracture stability can be used as a marker for general health or as a predictor of postoperative medical complications in elderly patients.
Materials and Methods:
We reviewed the records of all patients treated for IT fractures at our institution over the past 7 years. We excluded patients who were younger than 60 years, polytraumatized, involved in high-energy mechanisms of injury, managed nonoperatively, with hardware from previous surgery, or missing preoperative radiographs. Ninety-three patients were included in the present series. Three orthopedic surgeons independently reviewed all preoperative radiographs and classified each fracture as either stable or unstable. Interrater reliability was .77 (substantial) and consensus designation was assigned by majority. We reviewed charts for age, gender, time to surgery, length of hospital stay, type of surgery, estimated blood loss, American Society of Anesthesiologists (ASA) classification, and postoperative medical complications. Univariate and multivariate statistical analyses were conducted to determine the relationship of fracture stability on ASA class and medical complications.
Results:
Intertrochanteric fracture stability had no detectable relationship with ASA class (P = .497). On univariate analysis, stability was not significantly related to medical complications (P = .421). Our multivariate analysis found that only ASA was related to medical complications (P = .004), and fracture stability was not related to complications (P = .538).
Conclusion:
Intertrochanteric fracture stability does not appear to be a marker for poor general health or to predict postoperative medical complications in elderly patients in this limited study. ASA class was predictive of medical complications. Interestingly, medical complications were 8% greater in patients with unstable fractures than in patients with stable fractures.
Introduction
Fractures of the hip are the second leading cause of hospitalization in the geriatric population. 1,2 In many cases, these fractures represent a sentinel event signaling a progressive decline in the patient’s general health. Potential medical complications following hip fractures and subsequent operative fixation include but are not limited to myocardial infarction, congestive heart failure, arrhythmias, pneumonia, pulmonary edema, bowel obstruction, gastrointestinal bleeding, stroke, delirium, acute renal failure, deep venous thrombosis, and pulmonary embolism. Previous evidence has shown that return to optimal functional levels after hip fracture surgery is not determined by the type of surgery performed but by preoperative comorbidities and frailty and postoperative complications. 3 Furthermore, we previously demonstrated that the American Society of Anesthesiologists (ASA) classification system, which represents an anesthesiologist’s assessment of the general health and well-being of a patient, 4 is strongly associated with medical complications in the postoperative period following hip fracture surgery in elderly patients. To our knowledge, no studies have investigated the relationship between hip fracture stability and ASA class or postoperative medical complications.
Intertrochanteric (IT) femur fractures (Orthopaedic Trauma Association [OTA] 31A) are extracapsular hip fractures involving the region between the greater and the lesser trochanters. These fractures are common injuries in the elderly population, often resulting from low-energy falls. Furthermore, patients who sustain IT fractures are often of poor general health. Intertrochanteric fractures can be classified as stable or unstable, taking into account fracture morphology and involvement of the posteromedial calcar. To our knowledge, IT fracture stability has never been used as a marker for general health or as a predictor of postoperative medical complications. The purpose of this study was to determine whether there is indeed a correlation between IT fracture stability and the general health of the patient and/or the likelihood of postoperative medical complications following hip fracture surgery. We hypothesized that those patients who sustain unstable IT fractures are of poorer general health and have more postoperative medical complications than those with stable IT fractures.
Patients and Methods
Prior to beginning our study, we performed a power analysis to test the hypotheses that medical complications and health status were independent of IT fracture stability versus the alternative hypotheses that they were related. We needed a total of 87 patients to observe a Cohen medium-sized difference 5 at a type 1 error rate of 0.05 and a power of 0.80. Our study population exceeded this minimum number.
The present study is a retrospective chart review of a cohort of patients within a single health care system. All elderly patients who had undergone operative fixation for an IT fracture (OTA 31A) within our health system from 2005 to 2011 were identified. Patients were included if they were more than 60 years of age, had sustained low-energy trauma (fall from standing height or less) resulting in an intertrochanteric fracture, and had undergone operative fixation within our health system. Patients were excluded if they had metabolic bone disease other than osteoporosis, if they had multiple orthopedic injuries, if they had nonorthopedic trauma-related injuries, if the mechanism of injury was high energy (greater than fall from standing height), if they were treated nonoperatively, if they had hip hardware from previous surgery, or if they did not have preoperative radiographs available for review. Ninety-three patients were included in the present series. All patients were allowed to weight bear as tolerated after surgery.
Three raters experienced in reviewing radiographs and familiar with the classification of IT fractures reviewed the preoperative anteroposterior hip radiographs of all 93 patients. Each fracture was independently classified as either stable or unstable by each reviewer, and a consensus classification was assigned by majority.
Postoperative Medical Complications Observed After Intertrochanteric Fracture Surgery, Classified by Organ System.

aA medical complication was defined as a medical problem that occurred during the hospital course and required management by a member of a medical service.
We used a free marginal κ 6 to test interrater agreement for fracture stability. Interrater reliability was found to be 0.77 (substantial). Univariate and multivariate statistical analysis was conducted to determine the relationship of fracture stability on ASA class and postoperative medical complications. Chi-square tests with Yates correction for continuity or Fisher exact tests (in cases in which the assumptions for the chi-square tests were violated) were used to determine differences in the rates of each type of complication among the various groups. These tests and a t test for independent samples were used to determine differences in demographic characteristics between the 2 groups. Finally, multivariate binary logistic regression analysis with use of the backward likelihood ratio technique was carried out, with a criterion of 0.10 for the elimination of a variable, to adjust the relationship between IT fracture stability and postoperative medical complications for all significant confounders. All statistics were calculated with SPSS Version 16.0 (SPSS Inc, Chicago, Illlinois).
Results
Patient Demographics by Intertrochanteric Fracture Stability.
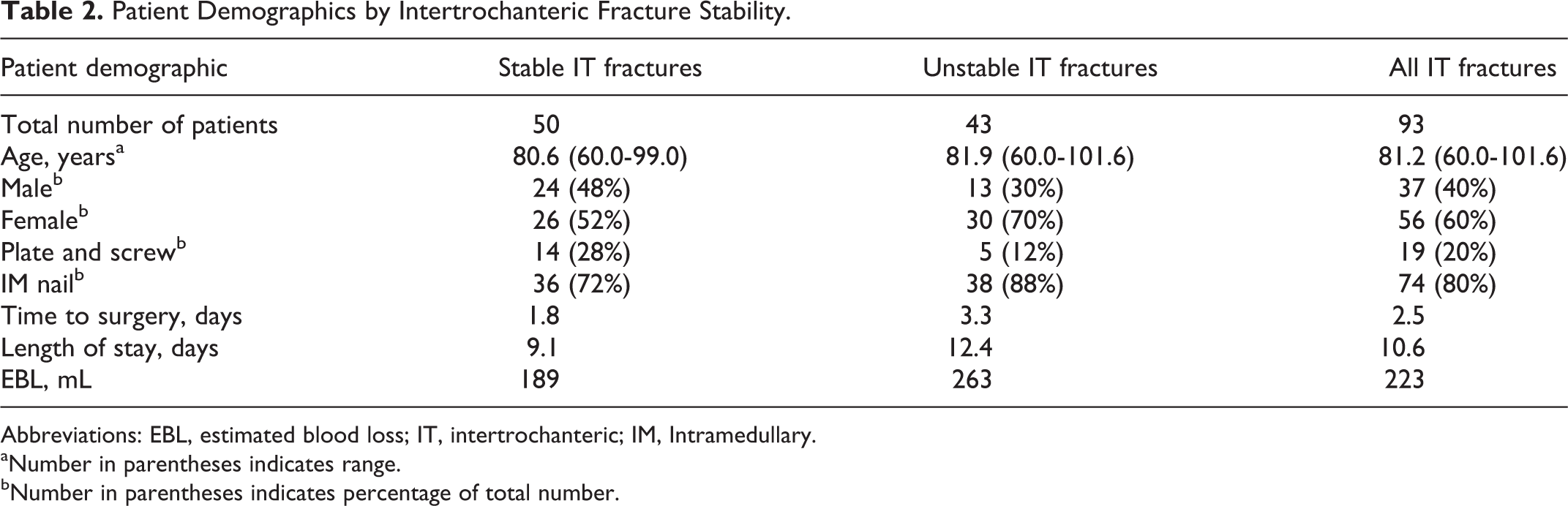
Abbreviations: EBL, estimated blood loss; IT, intertrochanteric; IM, Intramedullary.
aNumber in parentheses indicates range.
bNumber in parentheses indicates percentage of total number.
The Distribution of American Society of Anesthesiologists Class by Intertrochanteric Fracture Stability.a
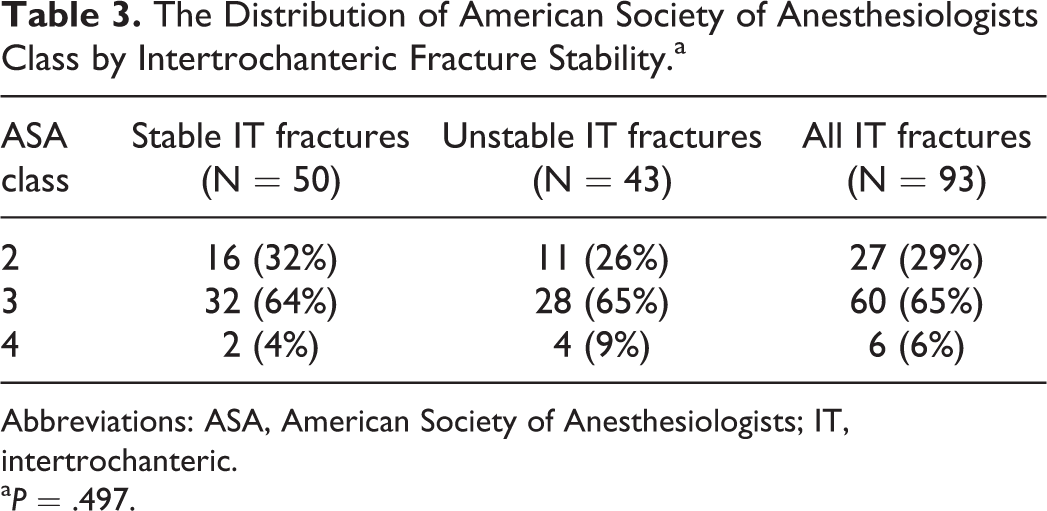
Abbreviations: ASA, American Society of Anesthesiologists; IT, intertrochanteric.
a P = .497.
Medical Complications by Intertrochanteric Fracture Stability.

Abbreviations: ICU, intensive care unit; IT, intertrochanteric.
Our multivariate analysis showed that ASA class was the only variable significantly related to postoperative medical complications (P = .004). Patients with greater ASA classes were more likely to experience medical complications during their inpatient stay. Importantly, IT fracture stability was not related to postoperative medical complications on multivariate analysis (P = .538).
Discussion
Fragility fractures of the hip often coincide with an overall decline in the health status and increase in frailty of elderly patients. A multidisciplinary approach to the management of these hip fractures has been shown to decrease the number of postoperative complications, transfers to the ICU, discharges to nursing homes, and days spent in the hospital. 7 Despite these improvements in patient management, hip fractures in elderly patients continue to represent a major public health concern. 8 It is of utmost importance to define those factors that are associated with poor outcomes so that we can identify those patients who are at the greatest risk of complications. Intertrochanteric fractures can be classified as stable or unstable, taking into account fracture morphology and involvement of the posteromedial calcar. To our knowledge, IT fracture stability has never been used as a marker for general health or as a predictor of postoperative medical complications. The purpose of this study was to determine whether IT fracture stability is a predictor of general health as measured by ASA class and/or of the likelihood of postoperative medical complications.
We found that IT fracture stability had no detectable relationship with ASA class (P = .497). Therefore, in this study, the general health of patients sustaining stable IT fractures appears to be similar to that of patients sustaining unstable IT fractures. Additionally, we did not find a significant association between IT fracture stability and immediate postoperative morbidity or mortality. The rates of medical complications by organ system, complications requiring surgery, transfer to the ICU, readmission to the hospital within 30 days, and death were not statistically different between the stable and the unstable groups. It is interesting to note that medical complications were 8% greater in patients with unstable fractures than in patients with stable fractures, even though this difference did not reach significance. This finding suggests the possibility that a larger cohort may be necessary to detect a statistically significant level of difference. Importantly, our study population was followed throughout the immediate postoperative period. During this time, patients were under the care of a multidisciplinary team, and any deviation from their baseline health status was detected quickly and managed without delay.
Interestingly, on multiple logistic regression analysis, ASA score was the only factor that predicted postoperative medical complications. This is consistent with our previous study that demonstrated the association between ASA score and postoperative medical complications following hip fracture surgery. 9 Other potential confounders, such as age, time to surgery, length of hospital stay, EBL, and type of fixation were not related to medical complications in our multiple logistic regression analysis.
This study was performed at a single institution using consecutive patients, which minimizes the variability in patient care practices that is inherent in a retrospective study design. Furthermore, we used a fracture database and electronic medical records, which ensured the completeness of our patient search and data collection. Because our study was retrospective in design and only included 93 patients, it is possible that we missed true differences on a multiple regression analysis due to variance inflation. However, our study was methodologically sound in that multiple raters rated both the exposure variable (fracture stability) and the outcome variable (medical complications). As such, our analysis had characteristics that would minimize systematic error. Assessment of bone mineral density was not routinely available in this study population, so we could not determine the effect of osteoporosis severity on fracture stability. Finally, our study was limited to complications in the immediate postoperative period; therefore, our results cannot be generalized to the long term and cannot be compared to previously published morbidity and mortality rates. Nevertheless, an examination of immediate postoperative complications is helpful in identifying patients who are at high risk of morbidity and mortality while they are in the hospital.
Interestingly, our interrater reliability with regard to IT fracture stability was substantial (κ = .77). Our results are consistent with those from a previous study by Pervez et al that determined that observers were able to reliably determine whether fractures were stable trochanteric, unstable trochanteric, or transtrochanteric. 10 In contrast, Fung et al found that surgeons were unable to reliably determine IT fracture stability. 11 That study did note that increasing experience led to improved agreement, but even staff trauma surgeons only had moderate agreement (κ = .53). 11
In conclusion, elderly patients sustaining IT hip fractures are at high risk of medical complications after surgery. Fracture stability is not an important predictor of general health or of postoperative medical complications. Therefore, surgeons should rely on more traditional risk factors, such as ASA class, to identify patients who are at high risk of morbidity and mortality. Although our study was powered on the a priori assumption that the difference between stable and unstable fractures would be “medium” (the size which corresponds to a clinically meaningful difference), 12 our actual difference in complication rate was 8%. In order to detect a change in that magnitude, we would have needed over 600 patients per group. However, because the difference is small, we feel that the stability of an intertrochanteric fracture is probably not a useful predictor of postoperative medical complications.
Footnotes
Authors’ Note
IRB Approval: This study was approved by the University of Pennsylvania Institutional Review Board (IRB).
Declaration of Conflicting Interests
The author(s) declared potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Keith Baldwin serves as a consultant for Synthes, is currently receiving a grant from the Board of Women Visitors, is receiving payment for manuscript preparation from The Journal of Bone and Joint Surgery, and holds stock in Pfizer. Samir Mehta is a board member for Pennsylvania Orthopaedic Society and AO Trauma, serves as a consultant for Smith & Nephew and Synthes, is currently receiving grants from the Department of Defense, OTA, and FOT, receives payment for lectures from Zimmer, Smith & Nephew, and Synthes, and receives royalties from Wolters-Kluwer and Elsevier. Derek Donegan serves as a consultant for Synthes.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.