
Abstract
Introduction
Intertrochanteric (IT) fractures that fail fixation are traditionally treated with arthroplasty, introducing significant risk of morbidity and mortality in frail older adult patients. Revision fixation with cement augmentation is a relatively novel technique that has been reported in several small scale international studies. Here we report a clinical series of 22 patients that underwent revision fixation with cement augmentation for IT fracture fixation failure.
Methods
This retrospective case series identified all patients that underwent revision intramedullary nailing from 2018 to 2021 at two institutions within a large metropolitan healthcare system. Demographics, injury characteristics, Charlson Comorbidity Index score, and surgical characteristics were extracted from the electronic medical record. Outcomes were extracted from the electronic medical record and included radiographic findings, pain, functional outcomes, complications, and mortality.
Results
Average follow-up after revision surgery was 15.2 ± 10.6 months. Twenty patients (90.9%) reported improved pain and achieved union or progressive healing after surgery. Most of these patients regained some degree of independent ambulation (19 patients, 86.4%), with only 5 patients (22.7%) requiring increased assistance for their activities of daily living (ADLs). One-year mortality was 13.6% (3 patients). Of the 5 patients (22.7%) that experienced complications, 2 patients (9.1%) required revision hemiarthroplasty for subsequent fixation failure. The other 3 patients did well when complications resolved.
Conclusions
Revision fixation with cement augmentation can be an effective, safe, cost-effective alternative to arthroplasty for the management of cases involving non-infected failed IT fracture fixation with implant cut-out or cut-through limited to the femoral head in older adult patients that have appropriate acetabular bone stock.
Keywords
Introduction
Hip fractures are estimated to affect 500 000 adults annually in the United States by 2040. 1 They have a dramatic impact on quality of life2,3 and currently account for in-hospital mortality of 3-7%4,5 and 1-year mortality of 19.4-58%.1,5-9 Approximately half of all hip fractures are intertrochanteric (IT) fractures. 10 The two most common treatment implants for IT fractures are the cephalomedullary nail (CMN) and sliding hip screw (SHS).7,11,12
Despite improving technology, nonunion and fixation failures such as cut-out13-16 and cut-through16-19 still occur and can be potentially devastating.20,21 Recent studies report cut-out rates as high as 6% with modern implants.16,17,20-28 Risk factors for fixation failure include tip-to-apex distance (TAD) >25 mm, inadequate fracture reduction, unstable fracture pattern, positioning outside of center-center or inferior-center positioning, and varus femoral neck-shaft angle.13,22,25,29-36 Older age and osteoporosis have also been associated with fixation failure.13,24-26,29
Revision arthroplasty procedures are the recommended treatment for failed IT fracture fixation.37-39 However, these are associated with several downsides. Compared to revision fixation, revision arthroplasty procedures are invasive surgeries that can be technically challenging, leading to increased blood loss, prolonged operative times, risk of intraoperative fracture, and risk of early dislocation.38,40-44 Given use of more expensive implants and longer surgical time, revision arthroplasty is also associated with higher costs compared to fixation. These limitations must especially be considered in frail older adult patients with multiple comorbidities.
There is a need for alternative and effective revision treatment for IT fracture fixation failure. In our institution, we started treating older adult patients with IT fracture fixation failure with revision implant exchange and cement augmentation of the cephalomedullary component, a technique reported in limited small scale studies in Europe and Asia. To our knowledge, this procedure is rarely, if ever, done in North America. Here we present the clinical outcomes of 22 patients that underwent revision fixation with cement augmentation of a failed IT fracture.
Methods
Patients and Setting
This was a retrospective review of patients that were treated in two institutions within a healthcare system located in a large metropolitan area. After approval by the Institutional Review Board, the case logs of two surgeons (JS and BC) were queried for all patients that underwent revision fixation with cement augmentation following primary fixation failure of an IT fracture from January 2018 to September 2021. Use of cement augmentation during revision surgery was confirmed through electronic medical record (EMR) review of operative notes and post-operative radiographs. We included all patients with evidence of cement augmentation in the setting of revision fixation for failed primary CMN or SHS fixation of an IT fracture (Figure 1). We excluded patients with femoral neck or subtrochanteric fractures, patients that underwent revision fixation without cement augmentation, and patients that underwent arthroplasty as their first revision procedure. A 76 year-old woman underwent cephalomedullary nail fixation for intertrochanteric fracture (A) and presented 2 months later for ongoing hip pain due to implant cut-out (B).
Surgical Technique
For patients that underwent primary fixation with a CMN, we performed a modified version of a cephalomedullary component exchange with cement augmentation.45-48 Initially a 5 cm incision proximal to the greater trochanter was made, a guidewire was placed into the proximal aspect of the nail, and all bone was cleared from the proximal aspect of the nail using the opening reamer. Next the hex screwdriver was used to engage and loosen the set screw on top of the CMN (Figure 2). Intraoperative fluoroscopy demonstrates a hex screwdriver engaging and loosening the set screw of the prior nail.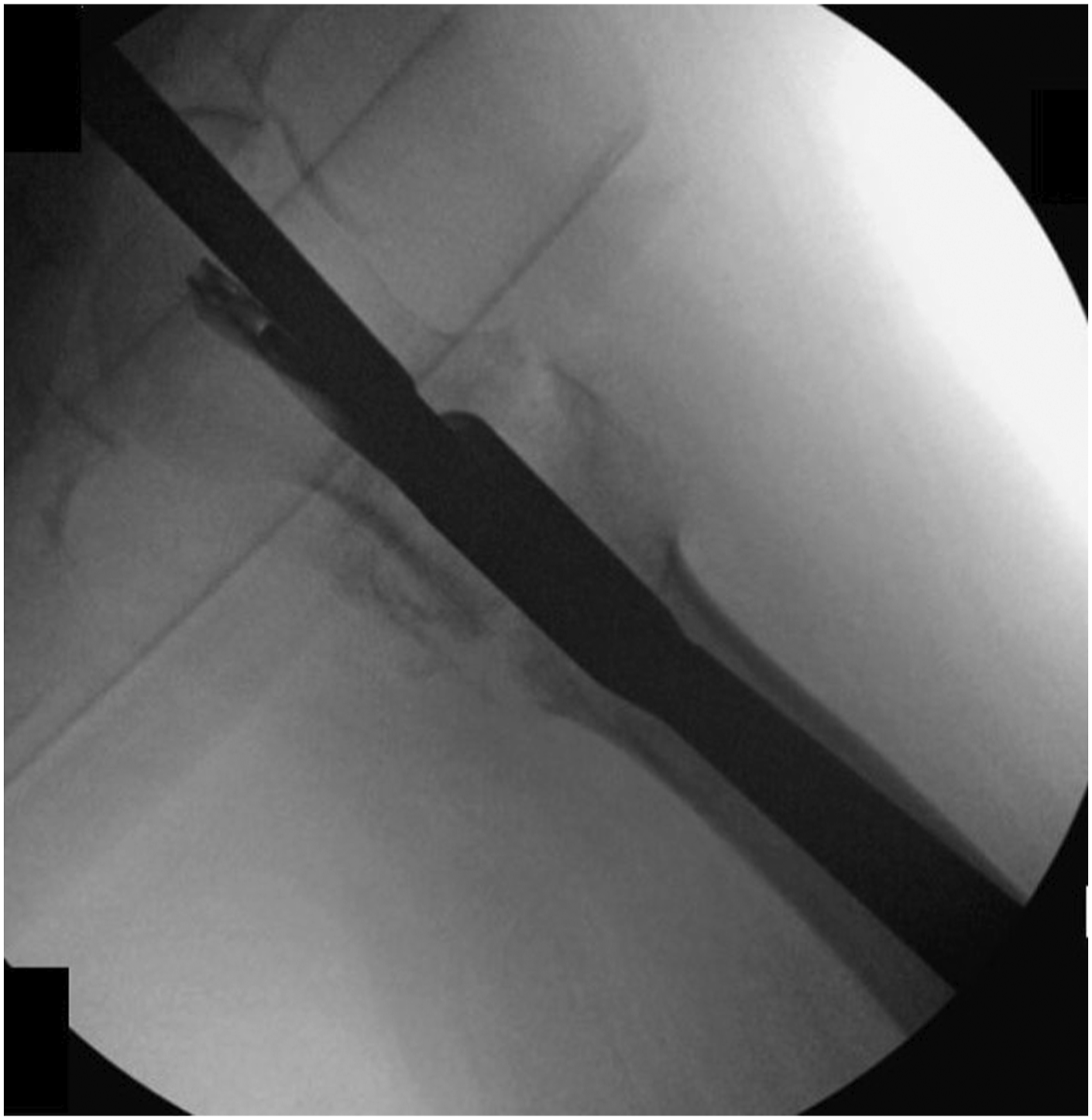
A lateral 1-2 cm incision was then made down through the iliotibial band (ITB) fascia. A reverse threaded guide engaged the original cephalomedullary component, which was then removed (Figure 3). To prevent cement leakage to the joint in cases with femoral head perforation, demineralized bone matrix was delivered to seal the defect through the prior cephalomedullary component track using the cannulated guide for the distal interlocking screw (Figure 3A). Specifically, the matrix was first injected after the outer two layers of the triple-sleeve cannula were removed and was then plunged into the area of perforation via reinsertion of the outer two layers. Intraoperative anteroposterior (A) and lateral (B) imaging of another patient demonstrate removed cephalomedullary blade with interval bone grafting of defect.
Next traction was added to the extremity and the fracture was then reduced into more valgus to proceed to revision fixation. In cases with malunion or fibrous union, a percutaneous osteotomy was made from an anterolateral approach using a quarter inch osteotome. This was rarely necessary yet highly effective when needed to produce an improved neck-shaft angle (goal of >130°).
Using the cepahomedullary guide-free hand, a guide wire for the new screw or blade was then placed along the axis of the femoral neck up to subchondral bone in the femoral head, ensuring care to not perforate the head (Figure 4). The new guide wire was intentionally placed to avoid the prior track but still end up center-center in the femoral head. A new fenestrated helical blade or set screw was then placed (Figure 5). Anteroposterior (A) and lateral (B) imaging of another patient shows Kirschner wire insertion along the new cephalomedullary component path. Intraoperative fluoroscopy demonstrates insertion of a new cephalomedullary blade along wire path, later secured via set screw tightening.

Finally, TRAUMACEM V+ injectable bone cement system (Synthes, Raynham, MA) was used to fill the femoral head with cement (Figure 6). Care was taken to avoid extrusion into the joint by using live fluoroscopy and adjusting the depth and direction of the cement cannula. The set screw was then secured and tightened using the torque-limiting screwdriver. Imaging demonstrates cement augmentation (A) of the original patient with progressive filling (B) until femoral head defect was filled (C).
For patients that underwent primary fixation with a SHS, we removed the SHS and placed a long CMN. After making a 5 cm incision centered below the greater trochanter and identifying the ITB, the incision from index procedure was used and dissection was carried down to the side plate. All plate screws were removed using the appropriate hand screwdriver, followed by extraction of the side plate. The lag screw was then removed with a reverse threaded guide as described previously, and the fracture was reduced into more valgus. Then, a 5 cm incision over the tip of the greater trochanter was made as previously described. A guide wire was inserted at the most proximal tip of the greater trochanter and advanced into the shaft of the femur. An opening reamer was introduced along the path of the guidewire, and if needed a bone hook over the calcar was used to hold the reduction. A long ball tip guide wire was then passed into the center-center position of the distal femur below the level of the patella. Next, progressive reaming was done until diaphyseal chatter was encountered. All our patients received a TFN-ADVANCED (TFNa) Proximal Femoral Nailing System (DePuy-Synthes, Raynham, MA) long CMN nail, the available implant at our institutions. The TFNa long nail was assembled with the nail guide, introduced along the reamed canal, and tapped in with a mallet. After using the guide sleeve to drill the guide wire into the femoral head as previously described, an opening reamer was inserted along the guide wire and advanced up until the femoral head again taking care to avoid the prior screw track. Cephalomedullary component insertion, cement augmentation, and set screw tightening was then performed as previously described.
It should be noted that conducting this technique for fixation failure patients that were initially treated with CMN implants that do not use a fenestrated blade or lag screw would require full exchange of the nail system and insertion of a cephalomedullary component that allows for cement injection into the femoral head. All patients in this case series that underwent primary fixation with a CMN component did so with a CMN system that includes fenestrated cephalomedullary component options that permit cement filling of the femoral head.
Variables of Interest and Outcomes
All variables and outcomes were extracted manually from the EMR. Regarding primary fixation, injury and surgical characteristics were determined radiographically and included OTA fracture classification and stability as well as post-operative reduction quality per Baumgaertner et al, 13 cephalomedullary component positioning within the femoral head, TAD, neck-shaft angle, and implant of choice. Cases with post-operative TAD >25 mm 13 or neck-shaft angle <125° 49 were noted.
For revision surgery, we collected demographics of age, sex, and body mass index (BMI). Charlson Comorbidity Index (CCI) score 50 was calculated based on EMR medical comorbidities. Other revision surgery characteristics included time from primary to revision fixation, indication (eg cutout, cut-through), and post-revision implant. Outcomes included follow-up time, radiographic union or healing, pain, ambulatory status, living arrangements, need for assistance with activities of daily living (ADL), complications, and mortality.
Regarding ambulatory status, patients were classified before and after surgery depending on whether they (1) ambulated without the use of assistive devices, (2) ambulated with the use of assistive devices, or (3) were mostly non-ambulatory. Regarding living arrangements, patients were classified before and after surgery depending on whether they resided in (1) an independent home, (2) an assisted living community residence, or (3) a long-term care facility. Regarding assistance with ADLs, patients were classified before and after surgery as (1) independent with ADLs or (2) needs assistance with ADLs.
Results
Injury and Surgical Characteristics for Primary Intertrochanteric Fracture Fixation (N = 22).

aOTA = Orthopaedic Trauma Association.
bCMN = Cephalomedulllary Nail.
cSHS = Sliding Hip Screw.
dAccording to Baumgaertner et al 1995, 1998.
eAccording to Walton et al 2005.
Demographics and Surgical Characteristics for Patients Undergoing Revision Fixation with Cement Augmentation (N = 22).

aCCI = Charlson Comorbidity Index.
bSHS = Sliding Hip Screw.
cCMN = Cephalomedulllary Nail.
Outcomes after Revision Fixation with Cement Augmentation (N = 22).

aOne of these patients passed away relatively early and was unable to be assessed properly. We included in “Non-Ambulatory” classification given functional decline.
bOnly patients that were above the lowest functional level for each category (ie “Non-Ambulatory”, “Long-Term Care”) were eligible for return to baseline assessment.
cADLs = Activities of Daily Living.

These are the final intraoperative anteroposterior (A) and lateral (B) imaging of the initial case. This patient demonstrated union at 3 months follow-up (C).
All patients with available follow-up were able to ambulate before injury, most using assistive devices (14 patients, 63.6%) (Table 3). Following revision surgery, 19 patients (86.4%) regained ambulatory capacity, with 16 patients (72.7%) returning to baseline. A total of 12 patients (63.2%) returned to their residential baseline, and only 5 patients (22.7%) required increased assistance for ADLs. All patients, other than 2 who underwent subsequent hemiarthroplasty, reported improved pain after surgery (Table 3).
Complications occurred in 5 patients and included 2 cases of fixation failure requiring revision hemiarthroplasty, 2 cases of surgical site infections, 1 case of avascular necrosis, and 1 case of bilateral post-operative pleural effusions. One hemiarthroplasty patient did well functionally for over a year with a cement-augmented CMN but then experienced increasing pain. Radiographs demonstrated cut-through as well as signs of AVN, prompting the surgeon to perform a revision hemiarthroplasty. This patient unfortunately passed away 2 months later due to stroke. The other hemiarthroplasty conversion patient experienced cut-out and increasing pain 4 months after revision cephalomedullary component exchange with cement augmentation. She declined functionally, was placed in hospice shortly after hemiarthroplasty, and passed away 2 months later from failure to thrive. Two patients developed superficial surgical site infections. They each presented with drainage and incisional pain and required one irrigation and debridement (I&D) procedure 2 weeks following revision implant exchange. They were both pain free and ambulating independently 2 months after I&D. Finally, one patient experienced increasing oxygen demands and was found to have bilateral pleural effusions. The effusions were transudative with no known cause and resolved after thoracentesis and supportive care. Of note, he had experienced similar episodes following multiple surgeries in the past. This patient is now pain free, ambulates independently, and has not had any further complications 18 months after surgery.
Discussion
IT fractures that fail internal fixation remain a challenging clinical scenario. We hypothesized that revision fixation with cement augmentation could provide an effective and safe alternative to the traditional treatment of arthroplasty, which can be an unacceptable procedure for frailer older adult patients. Revision fixation with cement augmentation provided favorable clinical results. Most patients demonstrated improved pain, regained function, and reassuring radiographic findings. The overall 1-year mortality was 13.6%. Only 2 patients required revision hemiarthroplasty a minimum of 4 months after revision fixation.
Our technique uses cement augmentation in the setting of revision fixation. Cement augmentation for primary fixation of osteoporotic proximal femoral fractures has been studied and shows favorable biomechanical and clinical results.20,51-57 A recent review reported that cement augmentation lead to higher loads to failure, decreased implant migration, and decreased complications and reoperations compared to non-augmented fixation. 20 A randomized multicenter prospective study also reported no reoperations or symptomatic episodes of CMN migration in a cement-augmented group vs 6 cases in the non-augmented group. 53 Regarding SHS, another recent review reported a 10.8-fold higher likelihood of construct failure in non-augmented SHS compared to that of cement-augmented SHS. 52
The literature is limited regarding cement augmentation in revision fixation of proximal femur fractures.45-48 Erhart et al 48 did a cadaveric biomechanical study that reported more rotational stability and increased pull-out strength for cement-augmented CMN compared to non-augmented CMN. Three articles report on clinical outcomes of revision implant exchange with cement augmentation. A recent report by Hanke et al 45 presented a successful case of revision CMN blade exchange with cement augmentation and cement plug placement at the femoral head defect that, at 1 year, led to no pain, return to pre-trauma functioning, and fracture union with no subsequent implant migration. Despite losing two patients to unrelated fatal events, Scola et al 46 reported fracture union at an average of 5.4 months for 10 patients following either full CMN or CMN blade exchange with cement augmentation. More recently, Lionel et al described 11 cases of CMN blade exchange with cement augmentation as well as 4 cases that underwent just blade exchange. They reported 2 THA conversions for cut-through in non-augmented patients vs none in the cement group. 47 Our case series validates the limited available data in the field and provides novel information on functional and quality-of-life outcomes.
Hip fractures in older adults can have drastic impacts in functioning and quality of life.2,3 Gjertsen et al 2 conducted a review of 10 324 patients that found that more than half of hip fracture patients report walking and pain problems after a year. The effect of cement augmentation on post-operative mobility is not well understood. Kammerlander et al 53 conducted a multicenter randomized controlled trial comparing primary CMN fixation with and without cement augmentation in 223 IT fracture patients and reported no Timed Up and Go test differences between the groups. In a recent systematic review of 5 studies and 301 patients, Stramazzo et al 51 found that 57.5% of patients that underwent primary fixation with cement augmentation achieved baseline pre-operative mobility. To our knowledge, no studies have reviewed these outcomes for revision fixation with cement augmentation. Our clinical series shows that 72.7% of patients reached their pre-operative ambulatory baseline, with 86.4% of total patients regaining some capacity of independent ambulation. We additionally observed that most of our patients either returned to living at their prior residential baseline or conserved their prior levels of independence for ADLs.
Hip fracture mortality is high. Recent research describes in-hospital mortality from 3-7%4,5 and 1-year mortality from 19.4-58%.1,5-9 IT fractures specifically have been shown to account for around 27% mortality after 1 year.8,9 Our clinical series demonstrated no in-hospital mortality as well as a 1-year mortality of 13.6%, which is relatively low compared to the literature. Because early ambulation after surgery is associated with lower mortality,58,59 the favorable ambulation and functional outcomes in our series may explain the relatively low mortality observed in our patients.
Two patients experienced fixation failure, one cut-out and one cut-through with AVN of the femoral head, and subsequently received a revision hemiarthroplasty. A recent study of 126 patients by Chapman et al reported an incidence of 5.6% cut-out in primary fixation of IT using CMN with helical blade, 22 and a recent review of 195 cases in 80 articles by Barquet et al 60 reported an AVN incidence of .95% 1 year after IT fracture. We observed higher incidences for these (9.1% and 4.5% for implant migration and AVN respectively) in a group of just 22 patients. Since our series was comprised of patients that underwent revision surgery and had bony deficits in the femoral head, it is difficult to compare these cohorts. Prior studies of revision with cement augmentation saw no events of failure, AVN, or revision arthroplasty,45-47 but these are also limited small-scale studies. A higher-power study may be warranted to properly evaluate the effect of revision with cement augmentation on subsequent failure and AVN.
Revision fixation with cement augmentation appears to be an effective and safe technique to address failed primary fixation of IT fractures. That being said, it is important to clarify that this procedure may not be indicated for any patient that fails primary fixation. At our institution, patients are directed to arthroplasty if they (1) suffered catastrophic fixation failure or failure involving the entire proximal femur (ie the implant cuts through the femoral neck) or (2) had significant acetabular erosion (approximately 50% or more). Revision fixation was additionally not conducted if (3) there was concern for concomitant infection of the hip or proximal femur. These patients, if deemed surgical candidates, were directed towards revision arthroplasty. Selection of patients that are appropriate for revision fixation with cement augmentation is critical to producing a successful outcome.
There are notable limitations in our work. This was a retrospective case series with a limited sample size. Our lack of standardized prospective data collection using validated patient-reported outcome measures limited our interpretation of outcomes such as pain and mobility. There is also currently no gold standard approach regarding the classification and assessment of objective functional outcomes, which has led to high variability in the way this information is reported in the literature.61,62 Thus, we recognize that our classification system for ambulation status, living arrangements, and assistance requirements was rather arbitrary. Moreover, we were unable to granularly identify independence and required assistance levels for patient ADLs. Instances of bone matrix leakage into the joint were not recorded, and thus we could not comment on the feasibility of using this component as a seal for femoral head defects. Our findings demonstrate that only three patients experienced an intra-articular cement leak and all experienced good outcomes. Finally, the CMN implant used in our revision procedures is the only available implant at our institution, which may impact the generalizability of our results to other implants. Furthermore, all patients were treated within a healthcare system in a single metropolitan area, further impacting the generalizability of our results.
Conclusion
Patients that sustained primary intertrochanteric fracture fixation failure and were subsequently treated with revision fixation and cement augmentation demonstrated favorable long-term clinical and quality-of-life outcomes. This procedure was solely attempted for cases where the majority of the articular surface of the acetabulum was preserved and where the cephalomedullary component was still contained within the femoral neck. Considering the limitations of revision arthroplasty in frailer older adult patients, this procedure shows promise by safely and effectively addressing a devastating complication while decreasing operative time and costs in this subset of patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Julie A. Switzer MD is a committee member for the American Academy of Orthopaedic Surgeons (AAOS), the American Orthopaedic Associations (AOA), and the International Geriatric Fracture Society (IGFS). She is also on the editorial board of Geriatric Orthopaedic Surgery & Rehabilitation. Brian P. Cunningham MD receives research support from Integra, and his spouse is the CEO and founder of CODE Technology. All other authors reported no disclosures or conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.