
Abstract
Background
Neck of femur fractures result in impaired function for older people. Despite surgery, many patients experience a decrease in functional level and poorer health status after the injury. The objectives of this study were (1) to determine the short-term mobility and hip function of geriatric patients who underwent hip replacement surgery for a displaced neck of femur fracture in our local population and (2) to identify factors which affect the functional outcome of these patients.
Methods
Patients aged 60 years and above, who were admitted for neck of femur fracture from January 2017 to December 2020, and treated surgically with arthroplasty, were included. Information on patient demography, comorbidities, perioperative data, mobility, hip function and complications were retrospectively collected. Outcome measures used were independent ambulation and recovery of pre-fracture mobility at 1 year after surgery while hip function was assessed using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) total, pain, stiffness, and physical function scores. Factors associated with these outcomes were analyzed.
Results
168 patients with a mean age of 75.2 (SD 8.4) years met the inclusion criteria. 32.1% of patients regained their pre-fracture mobility and 59.6% remained independent 1 year after surgery. Logistic regression analysis identified age, gender, surgical procedure, and time to surgery as significant contributors to recovery of pre-fracture mobility. Older age and increasing requirement for postoperative ambulatory aid resulted in worse WOMAC total and physical function scores. No significant differences were observed in patient-reported hip function between those who had a total hip arthroplasty and those who had a hemiarthroplasty.
Conclusion
Most geriatric patients with displaced neck of femur fractures did not regain pre-fracture mobility despite surgical treatment with arthroplasty.
Introduction
Neck of femur fractures remain a global public health concern. With an increasingly aged population worldwide, the incidence is expected to rise in tandem alongside healthcare costs and expenditure. 1 Most neck of femur fractures are a result of low-energy trauma in osteoporotic bone and is therefore unsurprisingly more common in the geriatric age group. 2
Sustaining a neck of femur fracture is a debilitating and potentially fatal injury for older people, resulting in impaired function, and a high morbidity and mortality. The goal of treatment is to get the patient up on their feet as soon as possible. Surgery allows for early mobilization and ambulation, accelerated rehabilitation and maintenance of independent living, and remains the mainstay of treatment as a conservative approach is associated with an increased mortality rate.3,4 Despite this, many patients experience a decrease in functional level and poorer health status after the injury.5,6 Published research has shown that up to 50% of older people with hip fractures do not reach their pre-fracture levels of functioning 1 year after injury. 7
This study presents new data on the short-term mobility and hip function of geriatric patients who underwent hip replacement surgery for a displaced neck of femur fracture in our local population and factors which affect the functional outcome of these patients.
Methods
This study was approved by the Medical Research and Ethics Committee (MREC) of the Malaysian Ministry of Health (NMRR ID-22-01674-PNB). The medical records of all patients who were admitted to the authors’ institution for neck of femur fracture from January 2017 to December 2020 were retrospectively analyzed. Patients aged 60 years and above, who sustained a displaced fracture of the femoral neck, and treated surgically with arthroplasty, were included in this study. Patients who were younger than 60 years old, treated with internal fixation, refused surgical treatment, or had a pathological fracture other than osteoporosis were excluded.
Information was retrieved from inpatient notes, operation theatre records and clinic notes on patient demography, American Society of Anesthesiologists (ASA) status, peri-operative data, preoperative mobility, postoperative mobility, and functional status, as well as complications. Acute fractures were defined as fractures that presented within 3 weeks from the date of injury while neglected fractures were defined as those that presented after 3 weeks. Time to surgery was the duration taken from occurrence of fracture to surgical intervention.
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) total score (range, 0 to 96), pain score (range, 0 to 20), stiffness score (range, 0 to 8), and physical function score (range, 0 to 68) was used to assess hip function in the outpatient clinic at 1 year follow-up, with higher scores indicating worse pain, stiffness, and functional limitations. The postoperative ambulatory status at 1 year was also recorded routinely. Multiple studies have demonstrated no difference in patient-reported outcome measures (PROMs) between 1 and 2 years.8,9 Therefore, 1 year follow-up data is reasonable for PROMs, rather than the required minimum 2-year data used for survivorship studies.
Sample size was calculated a priori using G*Power software, Germany (version 3.1.9.6). Considering 5% marginal error, 80% power of study and medium effect size, 128 subjects were needed to detect the mean of outcome variables. All data analysis was performed using SPSS version 26.0 (IBM Corp, Armonk, NY, USA) and statistical significance was defined as P < .05. Multiple imputation was used to treat missing data, which were missing at random. Normality was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests. To compare between groups, the independent samples t-test, Pearson’s chi-square test, Fisher’s exact test and one-way ANOVA were used, while the Pearson correlation coefficient was used to determine correlation between continuous variables and outcome scores.
Univariate and multivariate logistic regression models were fitted to examine relationships between variables. The multivariate regression model was constructed with purposeful selection of variables, after initially performing univariate analysis on each variable and selecting candidates based on a P-value cut-off point of .25. The performance of the models was assessed using goodness-of-fit tests.
Results
Patient Characteristics and Clinical Details (n = 168).

Values for age, time to surgery, length of stay, duration of surgery and EBL are presented as mean (SD). All other values are presented as frequency (percentage). Chronic fractures are defined as those that presented after 3 weeks. ASA: American Society of Anesthesiologists. THA: total hip arthroplasty. HA: hemiarthroplasty. EBL: Estimated blood loss.
44.0% of patients underwent total hip arthroplasty and 56.0% underwent hemiarthroplasty, with the majority subjected to general anesthesia (66.7%). The lateral approach and cemented femoral stems were used in all cases. Cemented acetabular cups were used in all total hip arthroplasties. The mean time to surgery, length of stay, duration of surgery and estimated blood loss (EBL) were 19.8 (SD 1.4) days, 16.9 (SD 8.8) days, 115.6 (SD 30.6) minutes and 491.9 (SD 233.6) ml, respectively. 34.5% of patients experienced 1 or more non-hip related adverse events during their hospital stay, while 6.5% of patients had at least 1 hip complication after surgery.
Comparison Between Preoperative and Postoperative Mobility.
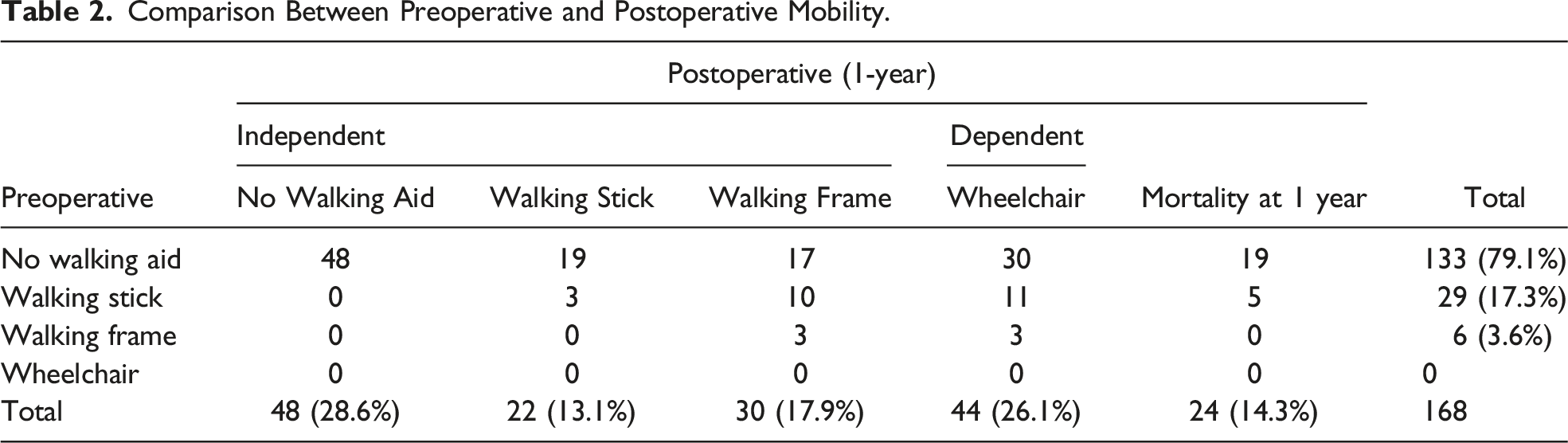

Preoperative and postoperative ambulation, including mortality at 1-year.
Association Between Variables and Postoperative Ambulation at 1-year.
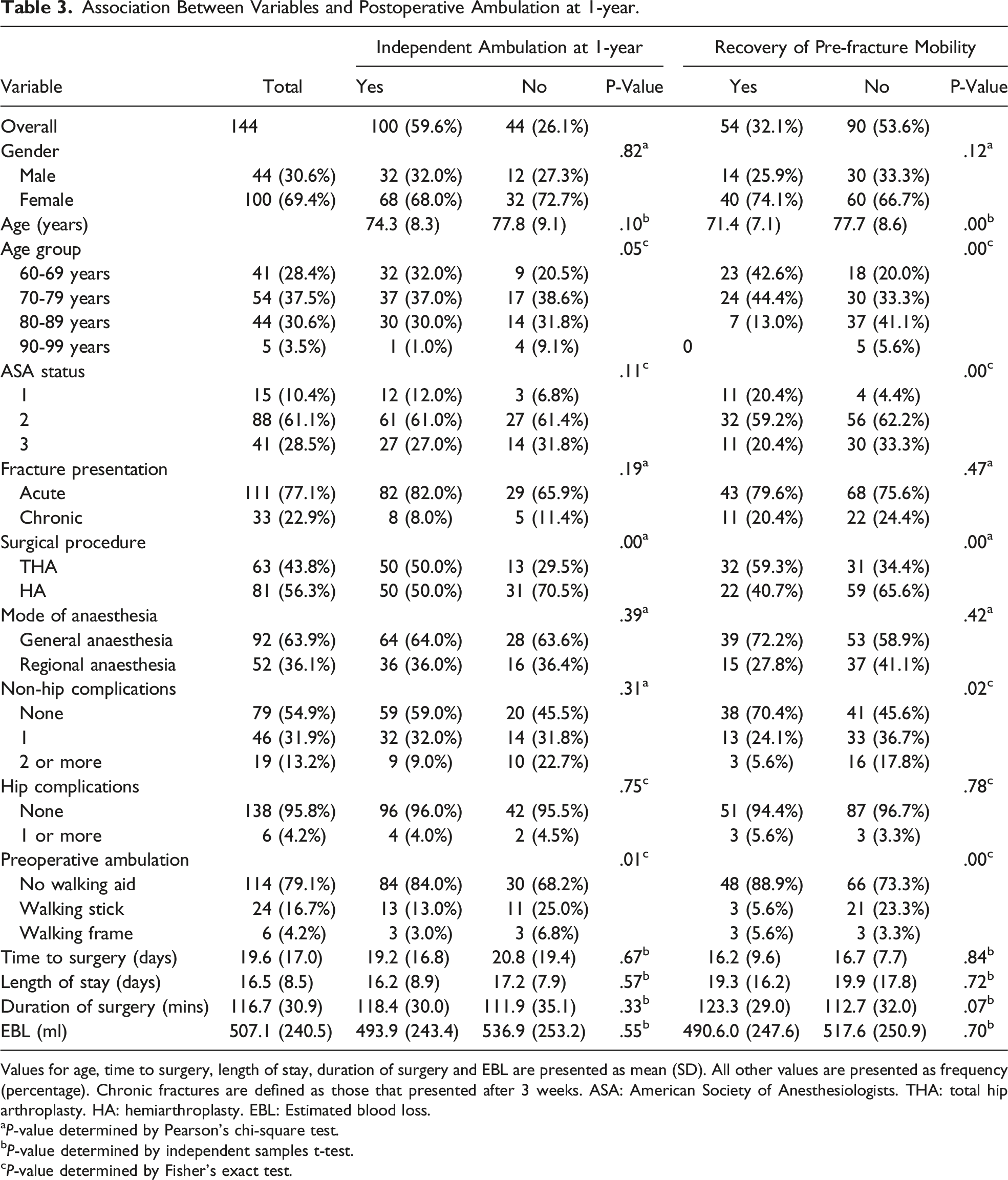
Values for age, time to surgery, length of stay, duration of surgery and EBL are presented as mean (SD). All other values are presented as frequency (percentage). Chronic fractures are defined as those that presented after 3 weeks. ASA: American Society of Anesthesiologists. THA: total hip arthroplasty. HA: hemiarthroplasty. EBL: Estimated blood loss.
aP-value determined by Pearson’s chi-square test.
bP-value determined by independent samples t-test.
cP-value determined by Fisher’s exact test.
Multivariate Logistic Regression Models for Independent Ambulation and Recovery of Pre-Fracture Mobility at 1-Year.

OR: odds ratio. CI: confidence interval. THA: total hip arthroplasty. HA: hemiarthroplasty.
No multicollinearity present in this model.
Difference Between Groups and 1-Year Postoperative WOMAC Scores.

WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index. ASA: American Society of Anesthesiologists.
aP-value determined by independent samples t-test.
bP-value determined by one-way ANOVA.
Subgroup Analysis of Surgical Procedure.
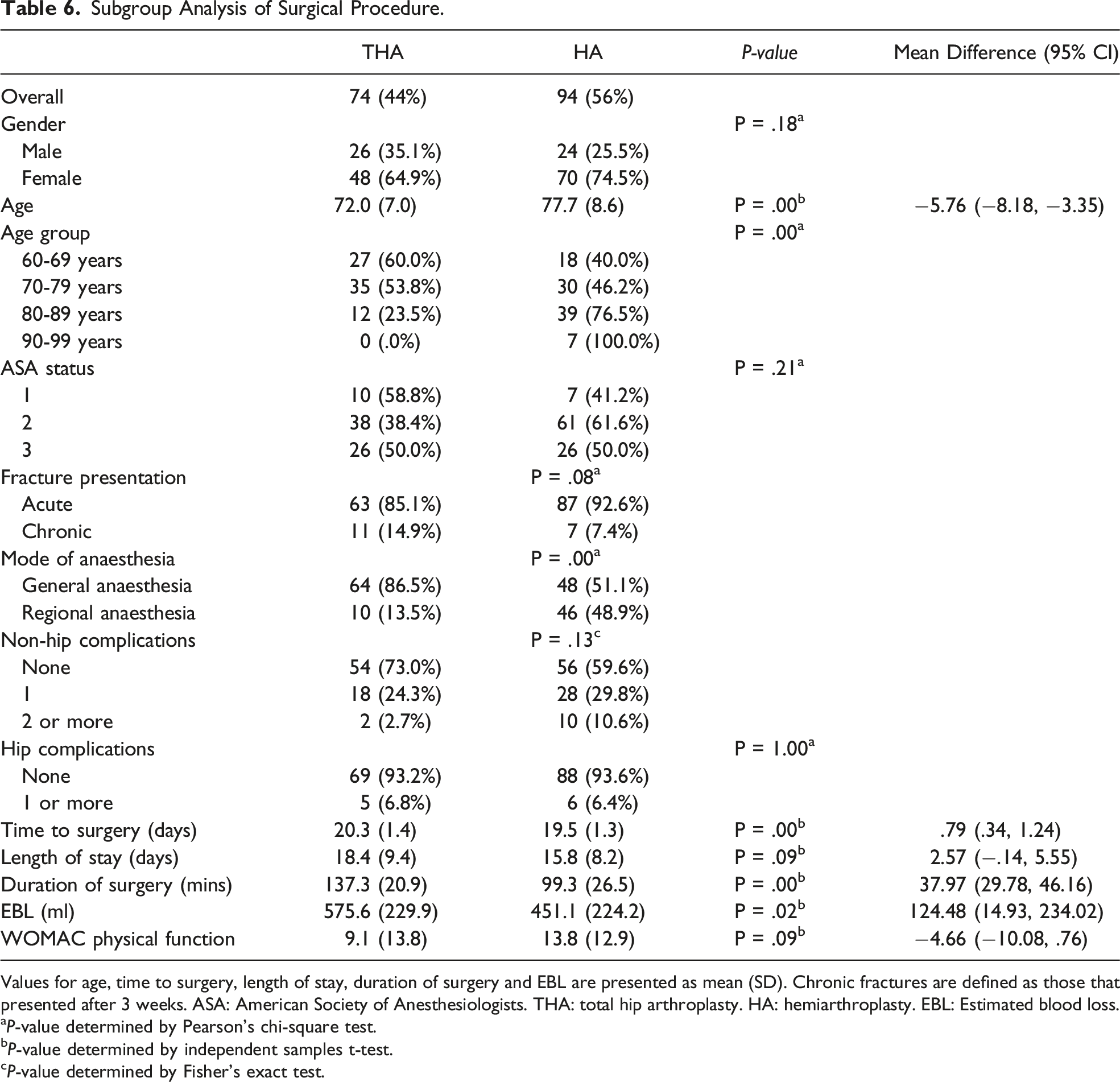
Values for age, time to surgery, length of stay, duration of surgery and EBL are presented as mean (SD). Chronic fractures are defined as those that presented after 3 weeks. ASA: American Society of Anesthesiologists. THA: total hip arthroplasty. HA: hemiarthroplasty. EBL: Estimated blood loss.
aP-value determined by Pearson’s chi-square test.
bP-value determined by independent samples t-test.
cP-value determined by Fisher’s exact test.
The 1-year mortality rate was 14.3% where the majority were from the 70 to 79 years old age group and ASA 3 category. Within the 1-year postoperative period, 1 patient from the total hip arthroplasty group underwent revision for recurrent dislocation and 1 patient from the hemiarthroplasty group underwent revision for stem fracture. There were no other secondary hip procedures within the study interval. Other hip related problems included foot drop (2), heterotrophic ossification (2), aseptic loosening of stem (1), wound complications (3) and prosthetic joint infection (1).
Discussion
Demography of the study population was predominantly female, at a 2.36:1 ratio and is reflective of local5,10 and regional 11 trends. However, these patients are relatively younger than those reported in other regions. 12 The authors’ institution provides orthopedic services to an area with a radius of approximately 200 km and is the only arthroplasty centre within the state. There are many remote communities within this area and there exists specific challenges with regards to healthcare access, due to distance and nature. Coupled with operating time constraints, these factors inadvertently result in a delay in presentation, longer time to surgery and length of stay.
The most important finding from this study was that a substantial proportion of patients did not regain pre-fracture ambulatory ability. All patients were able to ambulate independently, with or without aid, prior to fracture. Considering the mortality rate of 14.3%, at 1 year after surgery, only 32.1% managed to regain pre-fracture mobility status while 26.1% of patients became dependent. Prior to fracture, 79.2% of the patients were able to ambulate without a walking aid but only 28.6% retained this ability 1 year after surgery. Possible reasons include increasing frailty, or the lack of effective rehabilitative measures and monitoring of care delivery after discharge. 5 In 2019, Khor et al, 13 had conducted a study at a tertiary centre in the capital city and found that 41.6% of patients with hip fractures managed to regain pre-fracture mobility and that age, length of hospitalization and pre-fracture mobility status were predictors of mobility recovery. In this study, regression analysis showed that age, gender, surgical procedure, and time to surgery were predictors of mobility recovery.
The mortality rate in this review was lower than reported in past studies.14,15 This could be attributed to confounding factors such as a small sample size, or improved quality of care within our healthcare system. Involvement of geriatricians in the orthogeriatric care model has been shown to reduce complications, mortality rate, time to surgery and functional deterioration16,17 while early geriatric intervention benefits older patients with poor functional status prior to fracture. 18 Although surgeons are mostly concerned with surgery and implant related outcomes, it is important to note that better functional recovery leads to a better quality of life and thus, better overall results. Therefore, measures such as setting up a fracture liaison service, admission to a comprehensive geriatric care ward,16,19 improving time to surgery, 20 improving access to the healthcare facility and rehabilitation services, as well as continuity of care after discharge, could be implemented to improve patient outcomes in this locality.
There is strong consensus in the literature that arthroplasty is associated with a lower re-operation rate and better function than internal fixation for patients with displaced intracapsular hip fractures.21,22 However, there is still no agreement with regards to whether a total hip arthroplasty or hemiarthroplasty is superior. 22 Although multiple studies have favored total hip arthroplasty due to a lower revision risk, better function, and better quality of life,21,23,24 a recent randomized controlled trial has refuted this. 25
Results from this study showed that patients who had a total hip arthroplasty were more likely to remain independent 1 year after surgery, more likely to regain pre-fracture mobility and continue ambulating without a walking aid. Although regression analysis favored those who had a total hip arthroplasty, this advantage could be a result of selection bias as patients at the authors’ institution were planned for total hip arthroplasty if there was preexisting hip pain or if the Sernbo score was more than 16 i.e., younger, and healthier subset of older people who can ambulate independently. In addition, better WOMAC scores were observed in the total hip arthroplasty group at 1 year follow-up. Interestingly, this difference in patient-reported outcome measures was not significant and did not meet the threshold for minimal clinically important difference, 26 despite the selection bias and retrospective nature of this study.
The most common complications that these patients developed during their hospital stay were pressure sores followed by urinary tract infection. Analysis showed that this was not related to preoperative ambulatory ability, ASA status and time to surgery, nor did it have any significant association with postoperative independent ambulation and WOMAC scores. However, patients who regained pre-fracture mobility were less likely to have experienced these adverse events. Although not predictors for both regression models, this variable was included as it was found to be a significant confounding factor. In contrast, Hansson et al. 27 reported that the presence of general complications was a major risk factor affecting functional outcome and together with local complications, affecting pain and satisfaction. In this review, the total hip arthroplasty and hemiarthroplasty groups displayed no difference with regards to hip-related complications. The effect of all these variables on mortality rate was not analyzed.
The mean age of patients in this study was 75.2 years old. With an average life span of 75.6 years in this population, 28 and no significant differences in patient-reported hip function or complications after surgery in the short-term, it may be reasonable to choose hemiarthroplasty in this age group even when patients meet the criteria for total hip arthroplasty, especially if cost is a factor. Other advantages include shorter duration of surgery and less blood loss. However, the difference in transfusion requirement and long-term problems associated with hemiarthroplasty such as acetabular erosion and revision to total hip arthroplasty were not explored in this study. To the best of the authors’ knowledge, this is the first study to date on short-term mobility and hip function after geriatric neck of femur fractures treated with arthroplasty in this population.
Limitations
The main limitation of this study is that it is a retrospective review with a relatively small sample size. Therefore, patient groups or treatment modalities could not be compared objectively as the study subjects were not matched nor randomized. Furthermore, there is a lack of information regarding the rehabilitation process, which ostensibly could affect both mobility and hip function postoperatively.
Conclusion
A significant proportion of patients did not regain their pre-fracture mobility after sustaining a neck of femur fracture, despite surgical treatment with arthroplasty. In this retrospective review, there was no significant difference in patient-reported hip function between those who had a total hip arthroplasty and those who had a hemiarthroplasty.
Footnotes
Acknowledgments
We would like to thank the Director General of Health Malaysia for his permission to publish this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.