
Abstract
Aim
Internal fixation of femoral neck fractures is a widely used procedure that is comparatively less invasive and faster than hip replacement. While head preserving internal fixation of these fractures are still preferred where feasible, a faster recovery and lower reoperation rates make arthroplasty increasingly more appealing, in spite of being a more invasive option. Our aim was to determine the reoperation rate after internal fixation at our institution and to explore relevant risk factors in a geriatric population.
Methods
This monocentric follow-up study was conducted analyzing 116 patients aged 65 and older with femoral neck fractures who were surgically treated with either cancellous screws or dynamic hip screws between 2010 and 2017. We retrospectively collected longitudinal data from our patient database, supplemented by a telephone survey, with a follow-up period of at least 18 months.
Results
Twenty reoperations, due to either a failure of fixation, avascular necrosis, or posttraumatic osteoarthritis, were identified in our cohort, which constituted a reoperation rate of 17.2% (20/116). Fracture displacement was significantly associated with the reoperation risk (HR 8, CI 3-20; P < .001). The reoperation rate was 52.2% in displaced fractures vs 8.9% in undisplaced fractures. No link was found between the reoperation rate and gender, age, BMI, ASA score, type of implant, quality of internal fixation, type of living accommodation, and pre-fracture mobility.
Conclusion
Internal fixation has been found to be an effective option in elderly patients with undisplaced fractures regardless of their specific age, cognitive ability or physical condition. In displaced fractures the reoperation rate was found to be high, therefore a primary hip replacement should be recommended.
Keywords
Introduction
Femoral neck fractures are described as intra- and extracapsular fracture and require distinct treatment strategies. Intracapsular fractures far outweigh extracapsular fractures and can be classified into Garden’s Types I-IV, as a function of displacement on antero-posterior hip radiographs. 1 The optimal treatment for undisplaced fractures (Garden I and II) is still controversal, whereas several guidelines (NICE, ESTES) recommend arthroplasty for displaced fractures.2,3
About one quarter to one third of all femoral neck fractures show an undisplaced fracture pattern.4,5 This subset has a significantly lower reoperation rate after internal fixation when compared to displaced fractures.6,7 The ESTES guidelines include cannulated screws and dynamic hip screws as head-preserving techniques for undisplaced femoral neck fractures. 3 Reoperation rates after internal fixation in undisplaced fractures were reported between 4.5% and 27.7%, mainly due to a failure of fixation, avascular necrosis, or posttraumatic osteoarthritis.7-10 Risk factors for reoperation are fracture displacement and poor quality of reduction. 11 However, rather intuitive factors such as age, gender, body mass index (BMI), or bone mineral density appear to have no clear link or show contradictory results in different studies.12,13 Especially the specific age among the elderly is under debate concerning the best treatment approach.10,14
The aim of this study was to assess the reoperation rate after internal fixation of femoral neck fractures in patients aged 65 and older. Furthermore, we explored risk factors for a reoperation such as gender, age, BMI, ASA score, fracture classification (Garden, AO), type of implant, quality of internal fixation, type of living accommodation, and pre-fracture mobility.
Methods
Study Design and Population
The study design is monocentric, retrospective and longitudinal. The follow-up was carried out 18 months or more after the last surgery by searching the hospital’s database for current radiographs and clinical entries containing statements on postoperative course and surgical outcome. In cases of doubt, a telephone survey was conducted in June 2019 to identify potential reoperations that where performed elsewhere (“Have you had another hip surgery after surgery for femoral neck fracture? If yes, please specify.”).
We screened patients aged 65 years and older with femoral neck fractures that underwent a head-preserving surgery (cannulated screws or dynamic hip screw) between January 1, 2010 and December 31, 2017. Inclusion criteria were traumatic injury, intra- and extracapsular fractures, and a follow-up of 18 months and more. Exclusion criteria were stress fractures or pathological fractures (tumors), incomplete documentation or a follow-up of less than 18 months. Reoperation cases not related to surgical technique or implants were also excluded. A total of 132 patients were eligible. After applying the inclusion and exclusion criteria, 116 patients remained for final analysis and calculation of the reoperation rate. The excluded and included cases are displayed in Figure 1. Screened, excluded and included cases.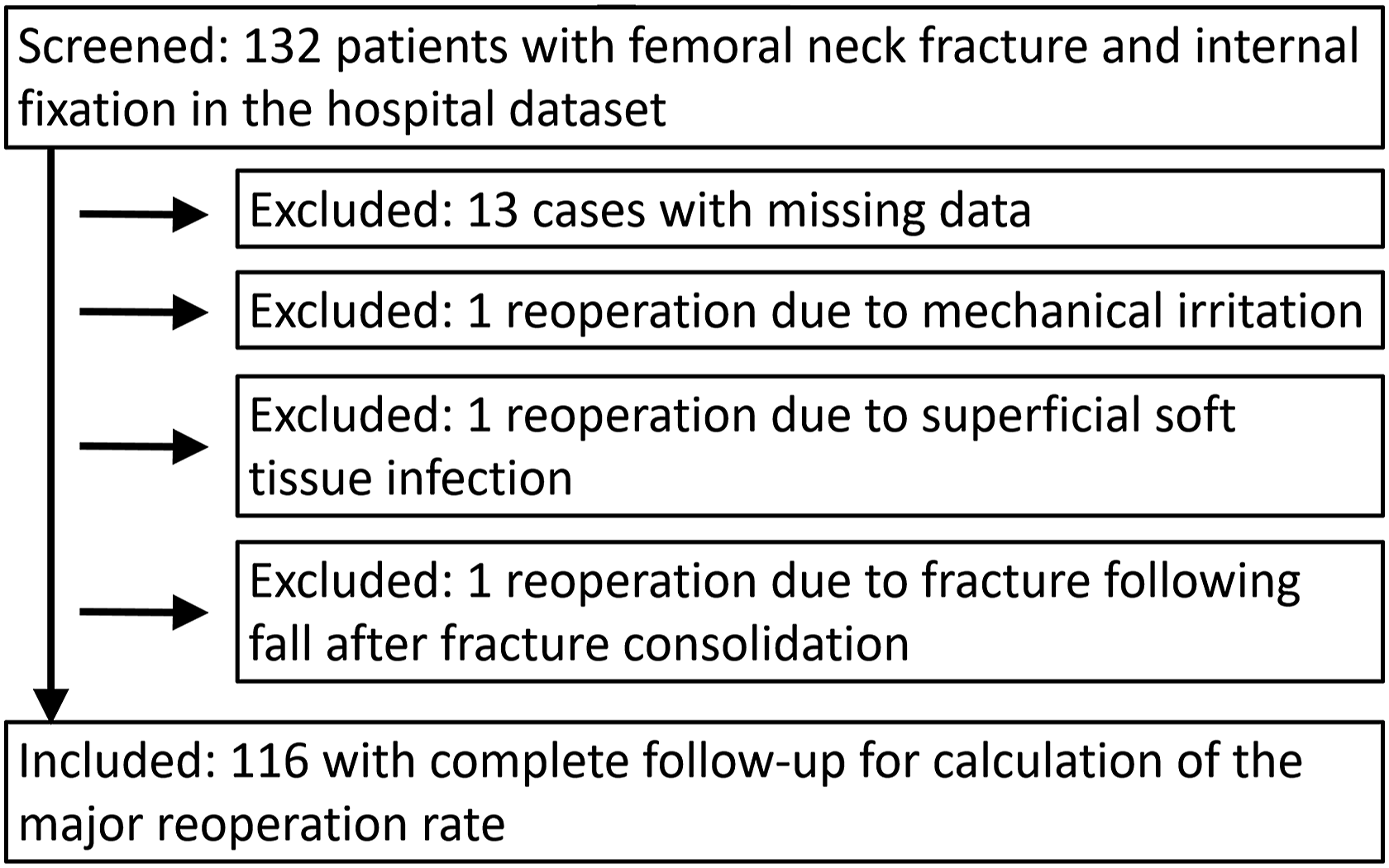
All patients were treated with the same postoperative protocol, which included non-weight bearing for 6 weeks after internal fixation of the femoral neck fracture.
Outcome Measurements
The primary study measure was reoperation after I: failure of the internal fixation, II: an avascular necrosis of the head, or III: posttraumatic osteoarthritis. The failure of the internal fixation was defined as an effect of delayed union or non-union.
The removal of screws due to mechanical irritation after fracture healing was considered a minor reoperation and was therefore excluded from the analysis of the reoperation rate and the reoperation risk.
Study Variables
Variables of interest were gender, age, BMI, ASA score, fracture type according to the Garden classification (Types I-IV) and the AO classification (B1-3), type of implant (two or three cannulated screws/dynamic hip screw), quality of internal fixation, type of living accommodation (own home/nursing home), and pre-fracture mobility (independent/with walking aid/wheelchair-bound/bedridden).
The quality of the internal fixation was defined as either good, fair, or poor. Fixation was considered good with parallel screw placement, subcortical screw position, and anatomical fracture reduction. Fair fixation was defined as an imperfection in one of these categories, and poor reduction as an imperfection in two or more of these categories. Variables derived from radiographs were assessed by the authors VL and TP, ambiguous cases were then reevaluated by PP.
Statistical Analysis
Patient characteristics were reported as frequencies and percentages for all data, as initially numeric parameters (age and BMI) were categorized. In the first place, univariable Cox regression analyses were performed to explore risk factors for reoperation. We assessed gender, age, BMI, ASA, fracture classifications (Garden, AO), type of implant, quality of internal fixation, type of living accommodation, and pre-fracture mobility. Hazard ratios (HR) were presented along with their 95% confidence interval (CI). Furthermore, Kaplan-Meier analysis and log-rank tests were performed.
For sensitivity analysis, a competing risk analysis was carried out considering death a competing risk. A P-value of .05 or less was considered statistically significant. All statistical analyses were conducted using R version 3.6.1 (https://www.r-project.org).
Results
After applying in- and exclusion criteria 116 patients were included in the study with a mean age of 79.5 years (SD 7.9), 70% being female. Nearly a third of the study population (34/116) was aged ≥85 years. The median follow-up time was 30 months (18-106).
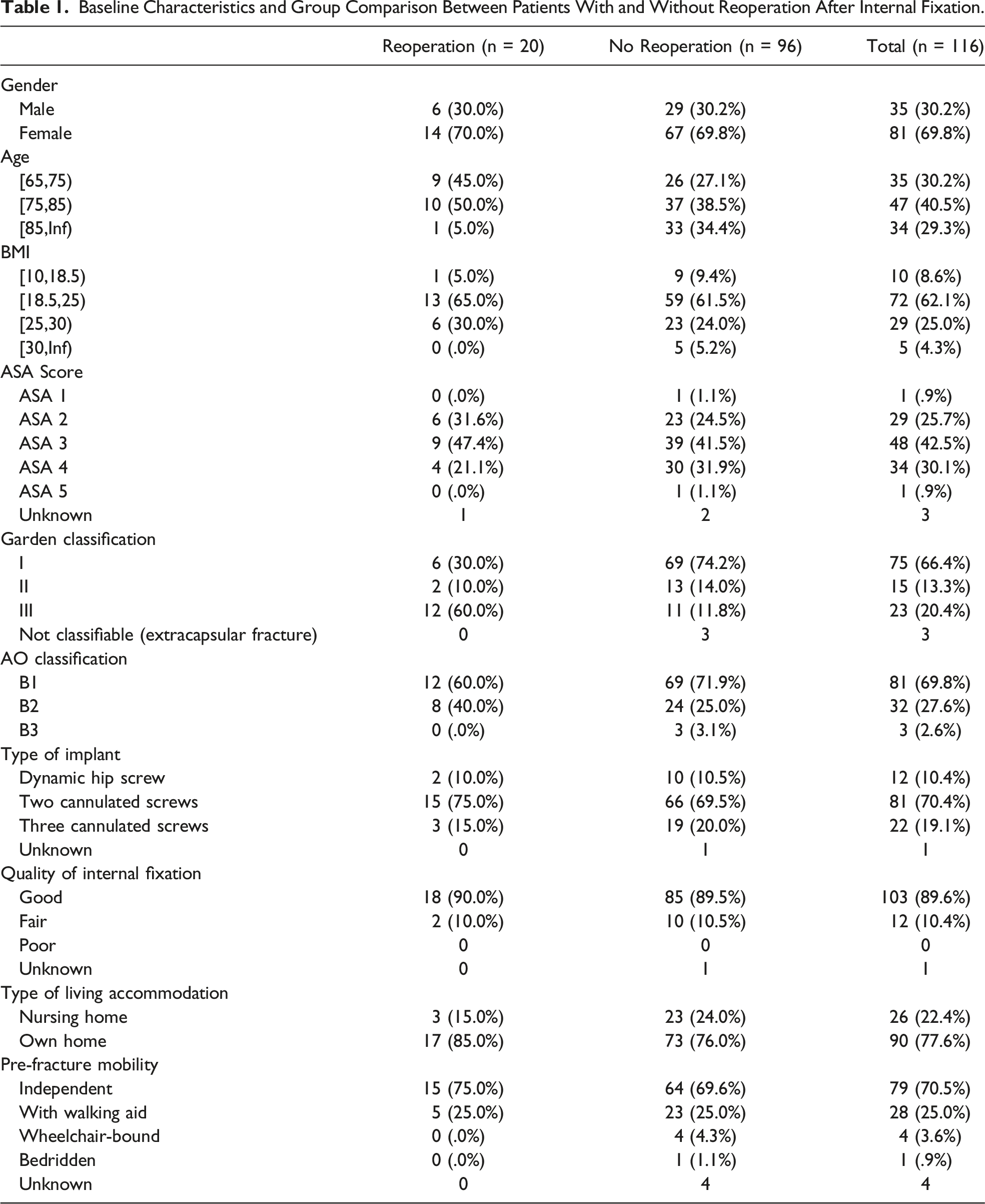
Baseline Characteristics and Group Comparison Between Patients With and Without Reoperation After Internal Fixation.
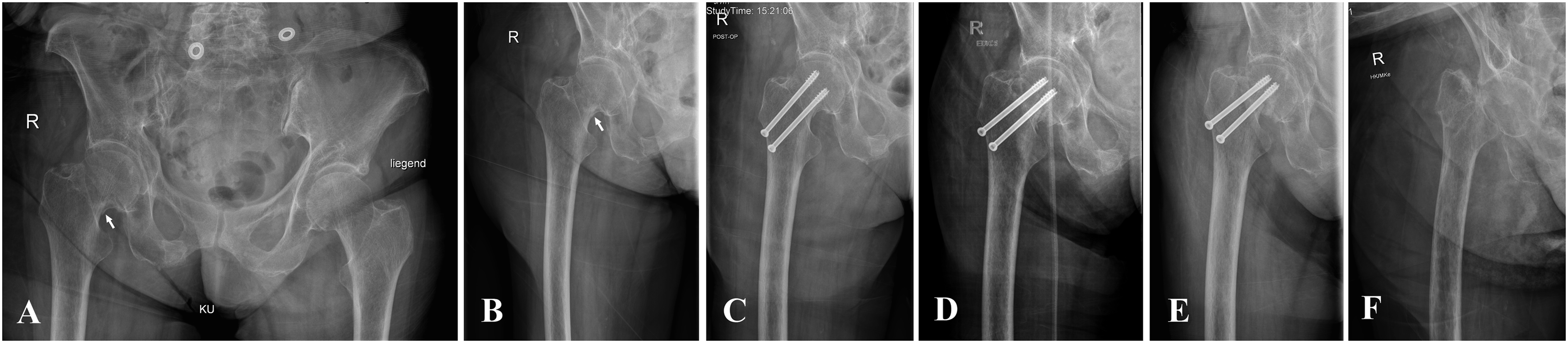
Radiographic evaluation of a multi-morbid patient with femoral neck fracture Garden III and internal fixation with two cannulated screws. A. Initial radiographs of the pelvis and B. the right hip demonstrating the Garden III classified fracture at the femoral neck due to a complete fracture indicated by a double contour (white arrow), C. Three days post-op radiograph showing internal fixation with two screws, D. Eight weeks post-op showing shortening of the femoral neck and varus tendency of the femoral head, E. Twelve weeks post-op showing failure of internal fixation with non-union and collapse of the construct, and F. A radiograph following metalwork removal and establishment of a Girdlestone excision arthroplasty.

Radiographic evaluation of a patient with Garden III femoral neck fracture and internal fixation with two cannulated screws. A. Initial radiographs of the pelvis and B. Right hip demonstrating the fracture, C. Two weeks post-surgery radiograph, D. Six weeks post-op radiograph showing failure of internal fixation with telescoping of the two screws, shortening of the neck, and varus collapse of the femoral head, and E. A radiograph following total hip replacement surgery.

Radiographic evaluation of a patient with Garden I femoral neck fracture and internal fixation with two cannulated screws. A. Initial radiograph of the pelvis and B. the left hip demonstrating the undisplaced fracture. C. Two weeks post-op radiograph, D. Four weeks post-op radiograph without any evidence of failure. The patient did not attend a follow-up appointment, likely due to successful initial healing. However, E. 1 year and 4 months later, the patient presented with radiographic evidence consistent with avascular necrosis of the head. F. The case was ultimately treated with total hip replacement surgery.
Detailed Information on Reason for Reoperation, Year of Reoperation, Procedure at Reoperation, and Time Until Reoperation.

Time to Reoperation
Overall, the median time between the first surgical repair and the reoperation was 8 (2-52) months (Table 2).
Fifteen patients suffered failure of fixation and underwent reoperation on after a median time of 5 months. Five patients had radiographic fracture healing after primary surgical repair, of which four presented with avascular necrosis of the head and one with posttraumatic osteoarthritis after a median time of twenty-one months. Only one case of reoperation was identified in the group aged ≥85 years (Table 1).
The Reoperation Rate in Displaced and Undisplaced Fractures
Analysis of Risk Factors
Fracture displacement was identified as a significant risk for reoperation in the Cox regression analysis. Patients with displaced fractures (defined as Garden III) had an 8-fold risk for reoperation compared to undisplaced fractures (defined as Garden I + II), (HR 8, CI 3-20; P < .001). There was no statistically significant link to an increased risk for reoperation in the Cox regression analysis for gender, age, BMI, ASA score, type of implant, quality of internal fixation, type of living accommodation, and pre-fracture mobility. Very similar results were obtained using the competing risk analysis (data is available upon request from the author).
Mortality Rate
Within the study population of 116 patients, 15 patients died within the first year. The 1-year mortality rate was 12.9% (15/116).
Discussion
The aim of this study was to assess the major reoperation rate after internal screw fixation of femoral neck fractures in patients aged 65 and older. Furthermore, we explored risk factors for reoperation such as gender, age, BMI, ASA score, fracture classification, type of implant, quality of internal fixation, type of living accommodation, and pre-fracture mobility.
The reoperation rate was strikingly high in patients with Garden III, (=displaced) fractures (Figure 5), a finding that is in line with previous reports.6,15 We found an 8-fold increased risk for reoperation in displaced fractures (Garden III) when compared with undisplaced fractures (Garden I and II). The current guidelines incorporate fracture displacement as the major determinant, where displaced fracture types should be treated with arthroplasty and undisplaced fractures with osteosynthesis.2,3 However, during the studied period (2010-2017), our institution favored osteosynthesis in several unclear cases, a circumstance that explains why we have a total of 23 displaced fractures for internal fixation in this work. In contrast to this view, there is evidence from an RCT in patients aged ≥70 suggesting the use of hemiarthroplasty even in undisplaced fractures. Hip function was similar after surgical repair, but an increased rate of reoperation occurred after screw fixation in comparison to hemiarthroplasty (20% vs 5%).
10
Kaplan-Meier plot for facture type (Garden classification) regarding reoperation.
Undisplaced fractures within our study population had a relatively low reoperation rate (8.9%). Compared to the literature, our rate ranks amongst the lowest reported values.7,9 The quality of reduction and internal fixation was rated as “good” in almost 90% of our cases and as “fair” in only 10%. This may partly explain the low reoperation rate in these patients with undisplaced fractures, where osteosynthesis is an established option.
Cox Regression Analysis Exploring Gender, Age, ASA Score, BMI, Fracture Displacement, Garden and AO Classification, Type of Implant, Quality of Internal Fixation, Type of Living Accommodation and Pre-Fracture Mobility as Possible Risk Factors for Reoperation.

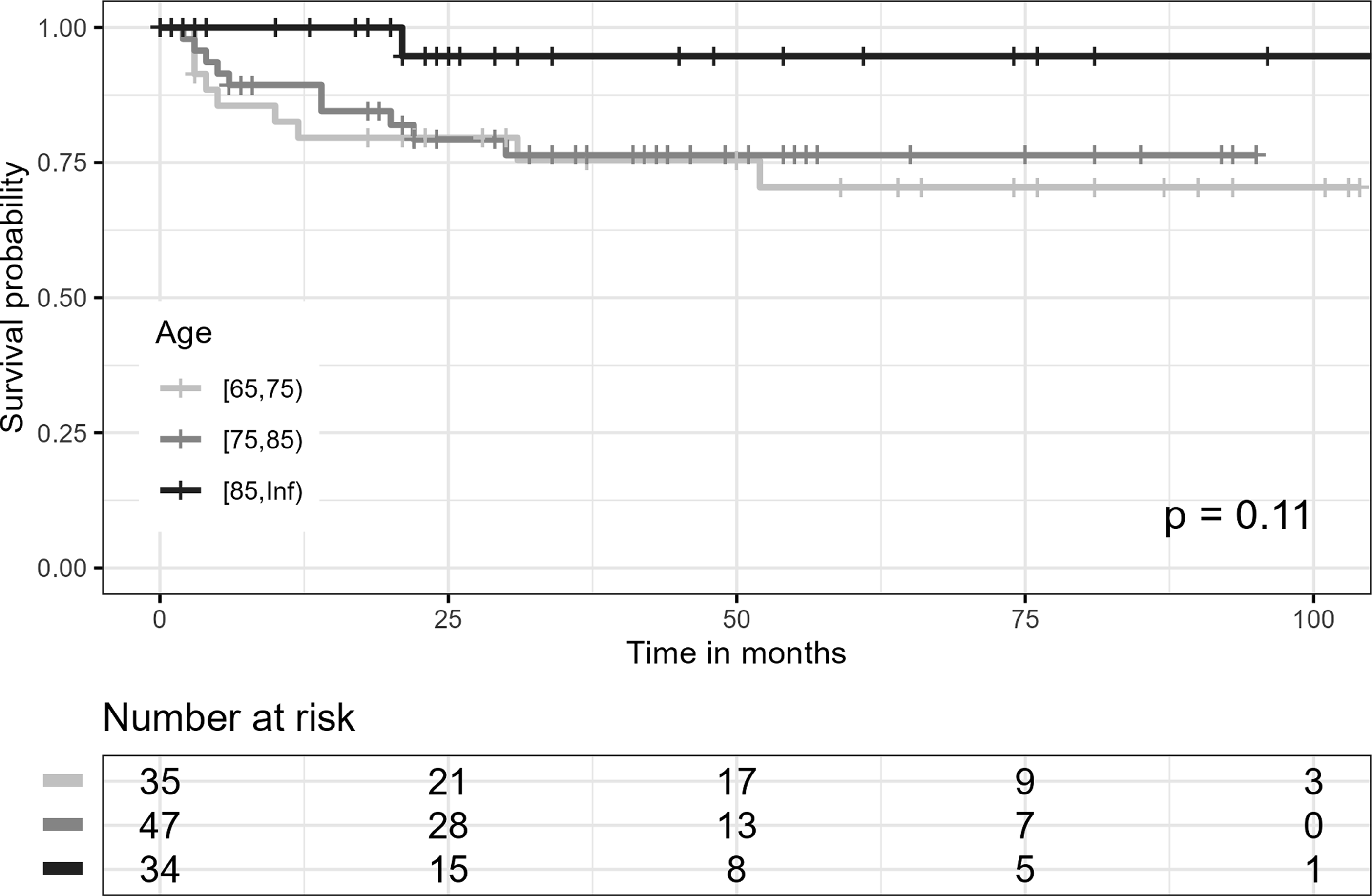
Kaplan-Meier plot for age groups regarding reoperation.
Secondary displacement in initially conservatively treated Garden I fractures was found to be associated to dementia, institutionalization, multiple comorbidities, and a history of repeated falls. 16 We investigated the type of accommodation (own home vs nursing home), going on the assumption that it may serve as an estimate for physical and cognitive fitness. We assume that nursing home residents are generally more frail and in need of more care than their peers. One in 5 patients lived in a nursing home, however, we found no statistically different risk for reoperation in these patients. Interestingly, higher reoperation rates among the youngest elderly patients who were physically fit and lived in their own homes were reported in literature. 11 They argue that this specific age group has higher demands regarding satisfactory functional results than nursing home residents. This fact in turn would increase the likelihood of reoperation. Accordingly, we tested further surrogate parameters for physical fitness (BMI, ASA score, and pre-fracture mobility) without identifying a link to reoperation.
The choice of implant as a risk factor for reoperation has long been a matter of discussion.17,18 The FAITH trial was an international, multicenter RCT that assessed the effects of a DHS (n = 557) vs cancellous screws (n = 551) on reoperation rates after two years in patients with a low-energy femoral neck fracture. 19 The overall results did not show a difference in the reoperation rate between the two implant types, only subgroup analysis suggested fewer reoperations following DHS in displaced fractures and smokers. Our data set comprises of twelve DHS of which two underwent reoperations. However, the statistical analysis did not reveal an advantage of one implant over the other.
There are several good arguments for internal fixation in undisplaced fractures in the elderly population. The procedure provides sufficient stabilization in frail patients with a low demand for physical function. 20 It does not expose the patient to the risk of potentially fatal bone cement implantation syndrome as in arthroplasty, 21 and it can be performed with regional anesthesia even in cases of severe cardiac compromise. 22
Limitations
A total of 16 cases have been excluded, 13 of those due to missing follow-up data (see Methods).
Due to the retrospective study design, there is a risk of selection bias. A total of 23 patients with initially displaced fractures were identified in our study. Why these patients were selected a priori for treatment with internal fixation is not known, however the treating surgeon chose to do so. At that time (2010-2017), evidence and guidelines on hip replacement for displaced fractures existed, but some surgeons were (erroneously) eager to preserve rather than replace the hip in a displaced fracture situation.
We were unable to explore established indices for hip function or quality of life, as they were neither collected nor documented.
Furthermore, we did not take other potential risk factors such as posterior fracture tilt (only seen on lateral radiographs or CT), 23 time-to-surgery, and comorbidity into consideration.
Conclusion
Head preserving techniques showed low reoperation rates in patients over 65 years with undisplaced fractures. In displaced fractures, however, the reoperation rate may be as high as 50%, hence primary prosthetic replacement should be recommended instead. Gender, age, BMI, ASA score, type of implant, quality of internal fixation, type of living accommodation, and pre-fracture mobility were not significantly associated with reoperation in our study population. However, the influence of the outlined risk factors on reoperation needs to be further investigated in prospective studies.
Footnotes
Acknowledgments
Thanks to Jan Lewis for proofreading the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Data is available upon written request to the corresponding author.
Ethics Approval
This study followed accepted ethical, scientific and medical standards and was conducted in compliance with the principles of the Declaration of Helsinki. The study was approved by the Ethics Committee of the Medical University Graz under the reference number 31-137 ex 18/19.
Consent to Participate
All study members gave consent to participate in the telephone survey.
Consent for Publication
All authors gave consent for publication.