
Abstract
Introduction
The effects of postoperative early weight-bearing (WB) on walking ability, muscle mass, and sarcopenia have been investigated. Postoperative WB restriction is also reportedly associated with pneumonia and prolonged hospitalization; however, its effect on surgical failures has not been studied. This study aimed to assess whether WB restriction after surgery for trochanteric fracture of the femur (TFF) is useful in preventing surgical failure, considering the unstable fracture type, quality of intraoperative reduction, and tip-apex distance.
Patients and Methods
This retrospective analysis included 301 patients admitted to a single institution between January 2010 and December 2021, diagnosed with TFF, and who underwent femoral nail surgery. Eight patients were excluded, and finally 293 patients were included in the study. Propensity score (PS) matching yielded 123 cases; 41 patients in the non-WB (NWB) group and 82 patients in the WB group were included in the final analysis. The primary outcome was surgical failure (cutout, nonunion, osteonecrosis, and implant failure). The secondary outcomes were medical complications (pneumonia, urinary tract infection, stroke, and heart failure), change in walking ability, period of hospitalization, and sliding distance of the lag screw.
Results
Five surgical complications occurred in the NWB group and two in the WB group, with significantly more surgical complications in the NWB group (P = .041). Cutout occurred in two cases, each in the NWB and WB groups. Two cases of nonunion and one case of implant failure occurred in the NWB group, but not in the WB group. Osteonecrosis did not occur in both groups. The secondary outcomes were not significantly different between the two groups.
Conclusions
The results of this retrospective cohort study using a PS matching approach showed that WB restriction after TFF surgery could not decrease the incidence of surgical failures.
Keywords
Introduction
Globally, the incidence of hip fractures is estimated to be approximately 1.7 million per year due to the growing elderly population. 1 Trochanteric fracture of the femur (TFF) accounts for approximately half of all the hip fractures, and its incidence is increasing. 2 Femoral nail surgery is widely performed for TFF, and good outcomes have been reported. 3 However, postoperative complications such as cutout and nonunion have been reported to occur in 3-13% of cases.4,5 The main risk factors for surgical failure are unstable fracture type, quality of intraoperative reduction, implant position, and tip-apex distance (TAD).6–9
Postoperative weight-bearing (WB) is restricted in the treatment of lower-extremity fractures to prevent fixation failure. 10 This is due to the long-standing concern that premature WB on the bony junction results in poor fracture fixation. 11 Postoperative early WB in patients with TFF has been recommended to help restore walking ability and prevent loss of muscle mass and sarcopenia. 12 It has also been reported that postoperative WB restriction is associated with pneumonia and prolonged hospital stay. 13 However, few studies have reported the impact of postoperative WB restriction on surgical failures, such as cutout. 14 In addition, no study has assessed the impact of postoperative WB restriction on the prevention of surgical failures, such as cutout, considering the following risk factors for surgical failure: unstable fracture type, quality of intraoperative reduction, and TAD.
We hypothesized that postoperative WB restriction after TFF surgery would decrease the incidence of surgical failures, such as cutout. This study aimed to assess whether WB restriction after TFF surgery is useful in preventing the occurrence of surgical failure, considering unstable fracture type, quality of intraoperative reduction, and TAD. We also investigated the impact of postoperative WB restriction on medical complications, length of hospital stay, and walking ability.
Patients and Methods
This was a retrospective analysis of 301 patients who were admitted to a single institution between January 2010 and December 2021, diagnosed with TFF, underwent femoral nail surgery, and followed up for at least 6 months. The exclusion criteria were high-energy injury (fall from a height of more than 1 m and traffic accident), multiple traumas, and external lateral wall fracture during surgery. Ultimately, 293 patients were included in this study (Figure 1). Patient’s selection study flow chart.
Patient information was obtained from the hospital electronic medical records. Preoperative factors included patient age, sex, presence of dementia, and surgical risks determined by the anesthesiologist according to the American Society of Anesthesiologists (ASA) classification, fracture type, and the number of preoperative waiting days. Surgical factors, such as the position of intraoperative reduction, TAD,
15
and implant length (>220 mm or ≤220 mm) were investigated. For fracture type, we used a new Arbeitsgemeinschaft Osteosynthese (AO) classification;
6
31A1 was defined as stable, and 31A2.2, 31A2.3, and 31A3 as unstable.6,16 The position of the intraoperative reduction was evaluated and defined using previously reported methods.
8
The patients were evaluated using simple radiographs in the immediate postoperative period. In the frontal view of the reduction, anatomical type was defined when the medial cortical bones of the proximal femoral fragments (PFFs) and diaphyseal fragments (DFs) were in contact with each other, intramedullary type when the PFF was more medial than the DF, and extramedullary type when the PFF was more lateral than the DF. Similarly, in the lateral view of the reduction, the anatomical type was defined when the PFF and anterior cortical bone of the DF were in contact with each other, intramedullary type when the PFF was depressed posteriorly and within the medullary cavity of the DF, and extramedullary type when the PFF was displaced anteriorly and outside the medullary cavity of the DF.
8
A fracture with an intramedullary type in either the frontal or lateral images was defined as “poor reduction” (Figure 2). For TAD, the distance from the apex of the bone head to the tip of the lag screw was measured on the frontal and lateral view of simple radiographs. Using the lag screw diameter as a reference, the true distance was calculated after correcting for the magnification of the simple radiographs. The TAD was divided into TAD ≥25 mm and <25 mm.9,15 “Poor reduction” is defined as intramedullary type of reduction in either the frontal or lateral radiographic images.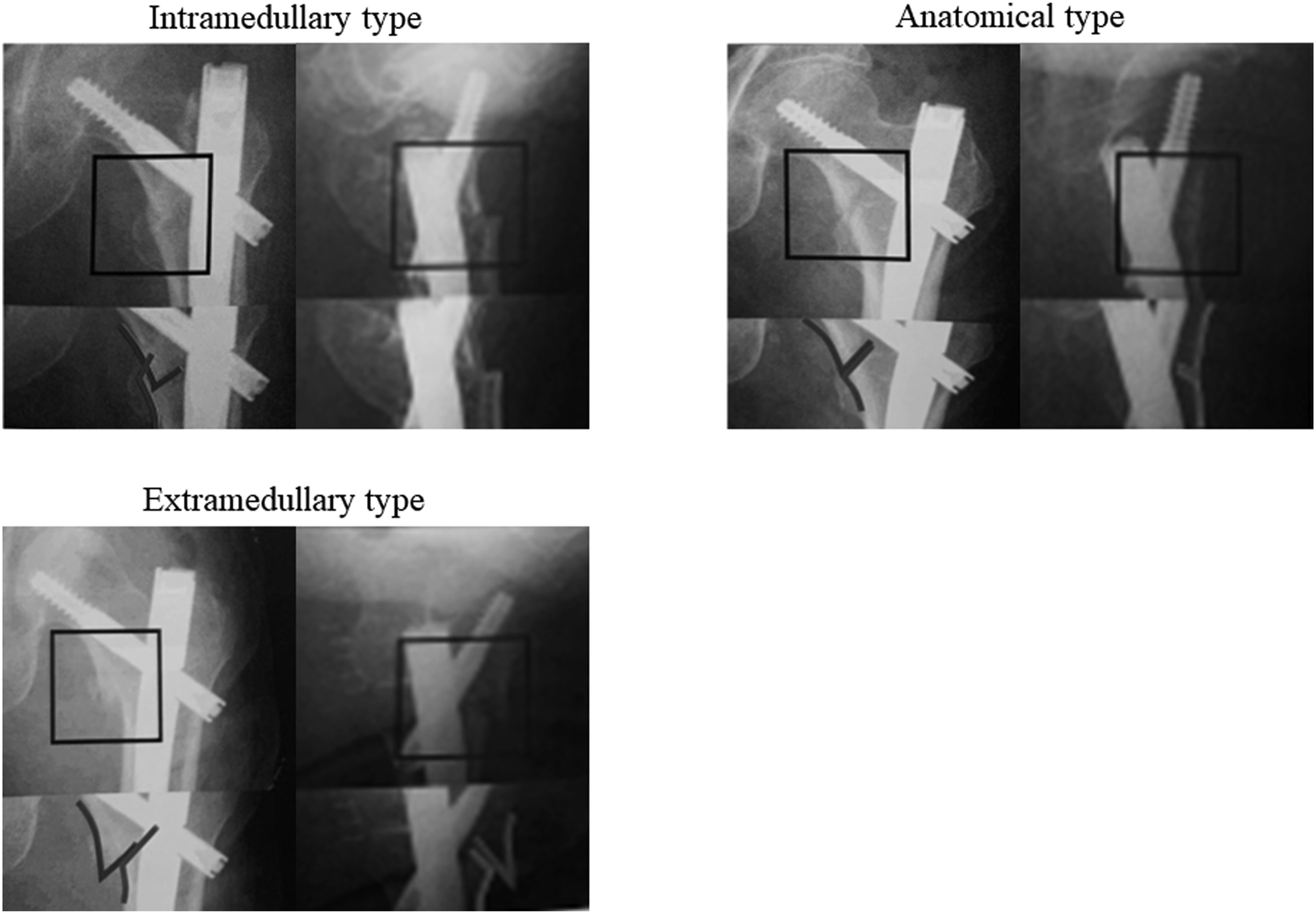
In terms of postoperative rehabilitation, the hospital usually begins rehabilitation on the day after surgery by applying as much weight as the patient can bear. Under the guidance of a physical therapist, standing and walking were performed with the assistive device, and the assistive device was changed as walking ability improved, with the goal of achieving walking independence. There are three basic determinants that make it non-WB (NWB). The first is if the fracture type is unstable, as in an AO classification A2.2, A2.3 or A3 fracture. The second is poor reduction, for example, when there is very little contact between the proximal and diaphyseal fragments, or when the proximal fragments are more intramedullary than the diaphyseal fragments. The third is when there is a defect in the implant, such as failure to place a distal screw. Using these three basic criteria, the surgeon ultimately made the decision and indicated whether to WB or NWB based on his own experience as well.
The group that was allowed to rehabilitate with WB as much as possible from the day after surgery to within 1 week after surgery was defined as the WB group. Conversely, the group that was instructed to perform rehabilitation with no WB for more than 1 week after surgery was defined as the NWB group.
The primary outcome was surgical failure (cutout, nonunion, osteonecrosis, and implant failure). The secondary outcomes were medical complications (pneumonia, urinary tract infection, stroke, and heart failure), change in walking ability, period of hospitalization, and sliding distance of the lag screw. The patient’s walking ability was established based on a previous report.
17
Walking ability was stratified into the following five categories: (1) use of a wheelchair (no walking), (2) use of a walker, (3) use of crutches, (4) use of a single stick, and (5) independent gait. The change in walking ability was modified based on a previous report.
18
Changes in walking ability were defined as walking ability at the last follow-up minus walking ability before injury. The sliding distance of the lag screw was measured using a simple radiograph in frontal view. The sliding distance was measured 1 month postoperatively, with the immediate postoperative period as the reference. The true distance was calculated using the lag screw diameter as the reference and by correcting for the magnification of the simple radiograph (Figure 3). (a); Radiograph immediately after surgery, (b); Radiograph one month after surgery Sliding distance of lag screw = (Xb × Db/Dtrue)−(Xa × Da/Dtrue) (Dtrue: known true diameter of the lag screw).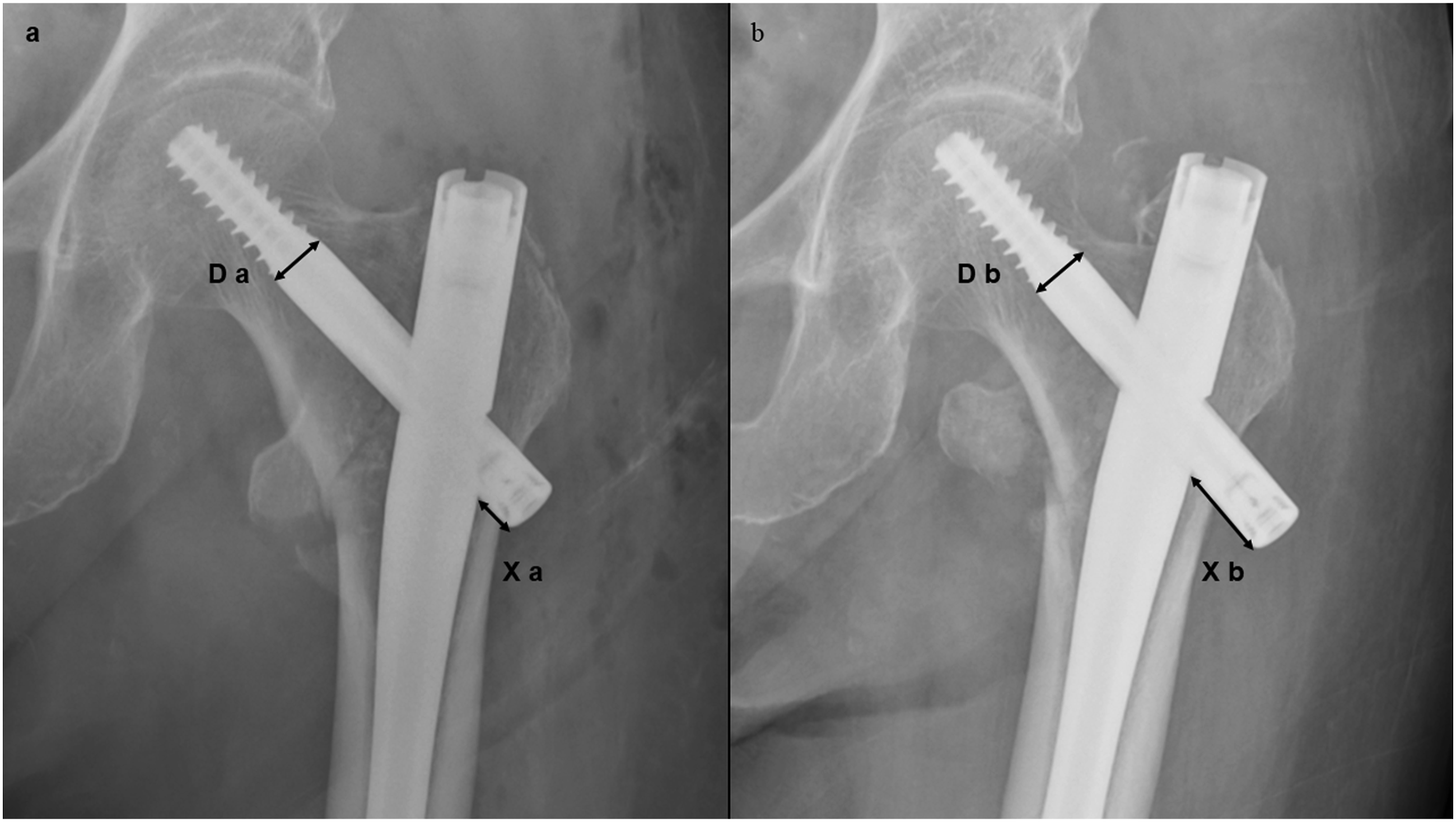
Statistical Analysis
To align the background factors of the two groups, multiple logistic regression analysis was performed with load restriction as the dependent variable, and fracture type, poor reduction, and TAD ≥25 mm as covariates, and a propensity score (PS) was calculated. To confirm that the estimated PS discriminated well between the NWB and WB groups, a receiver operating characteristic (ROC) curve was drawn and the C statistic was obtained; the C statistic was .826. Nearest-neighbor matching using PSs was performed with logistic regression analysis; one-to-two pair matching was performed with a caliper width of .2 of the standard deviation of the PS. Standardized differences were calculated to estimate the balance of covariates in the matched cohort. In this study, the standardized differences were the absolute values of the calculated standardized differences. The standardized difference was less than .1, suggesting that the variable balance after PS matching was adequate.
Continuous variables were analyzed using the t-test or Mann–Whitney U test, and categorical variables were analyzed using the χ2 test or Fisher’s exact probability test, as appropriate. All statistical analyses were performed using the R software (version 4.1.2; R Foundation for Statistical Computing, Vienna, Austria). The statistical significance level was set at P < .05.
Results
Patient Characteristics and Preoperative and Surgical Factors
Patient Characteristics.

ASA; American Society of Anesthesiologists; IQR; Interquartile Range.
Patient Characteristics After Propensity Score Matching.
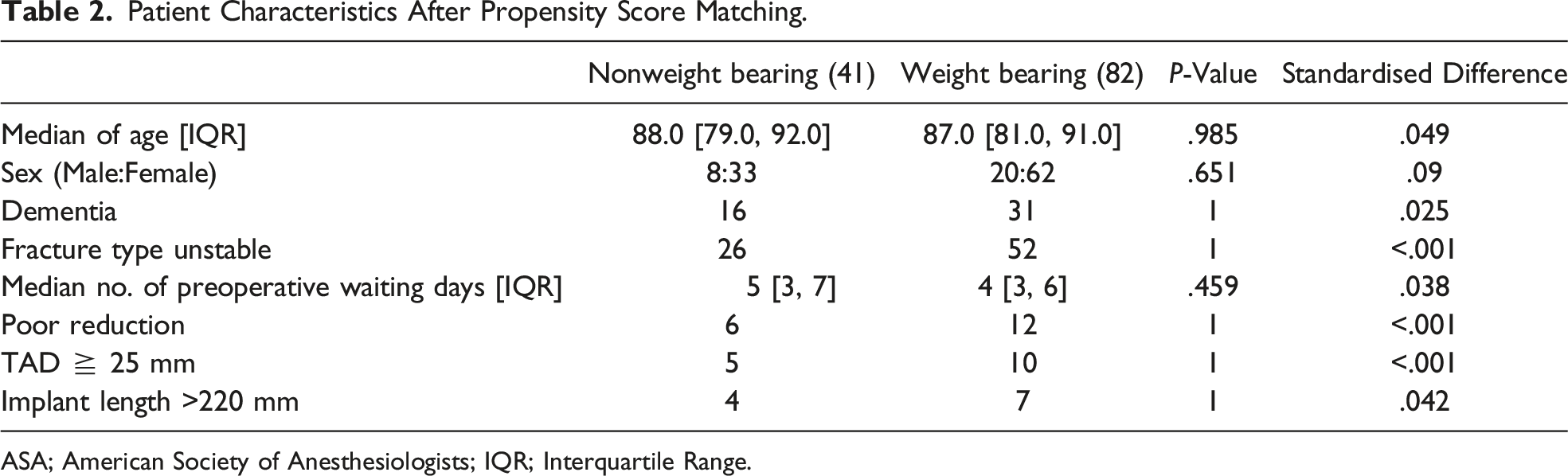
ASA; American Society of Anesthesiologists; IQR; Interquartile Range.
The changes in fracture type and intraoperative reduction before and after PS matching in the patient groups are shown in Figures 4 and 5. Fracture types before and after propensity score matching. A certain number of cases with unstable fracture type were included after the match. A; Anatomical type, I; intramedullary type, E; extramedullary type Intraoperative reduction before and after propensity score matching. It means a combination of frontal and lateral views of the reduction in simple radiographs. Shown in frontal image * lateral image. For example, I*E means intramedullary type in the frontal image and extramedullary type in the lateral image. A certain number of cases with poor reduction were included after matching.

Primary Outcome (Surgical Failure)
Primary Outcome and Secondary Outcome.

IQR; Interquartile Range.
Secondary Outcomes (Medical Complications, Change in Walking Ability, Length of Hospital Stay, and Sliding Distance of Lag Screw)
The secondary outcomes are shown in Table 3. The secondary outcomes were not significantly different between the two groups.
Discussion
In this study, we compared the occurrence of surgical failure between the NWB and WB groups using PS matching, adjusting for fracture type, quality of intraoperative reduction, and TAD, which are reported to be the major risk factors for surgical failure. The results showed that the NWB group had a significantly higher incidence of surgical failure than the WB group. These results were contrary to our hypothesis that postoperative WB restriction could reduce surgical failures, such as cutout. The results are novel and provide new insights into TFF treatment. There were no significant differences in medical complications, changes in walking ability, length of hospitalization, or sliding distance of the lag screw between the two groups. To the best of our knowledge, this is the first study to evaluate the utility of postoperative WB restriction after adjusting for fracture type, quality of intraoperative reduction, and TAD, which are considered to have a significant impact on surgical failure.
Some reports have shown that early loading is beneficial after TFF surgery in terms of restoring walking ability and decreasing mortality.19,20 However, in the aftercare of hip fracture patients, nearly 25% of surgeons recommend partial WB to “protect the bony junction” from overload. 21 Ottesen et al 21 reported that in a cohort of approximately 5000 patients, only 64% were able to bear weight postoperatively within acceptable limits, and approximately 25% of the patients were restricted from bearing weight postoperatively. In the present study, 82 of 293 patients (27.9%) were instructed to undergo postoperative WB restriction, which is consistent with previous reports.
In this study, late complications, such as nonunion and implant failure, were common. In a study comparing the time of bone healing in femoral diaphyseal fractures in the NWB and WB groups, the time of bone healing was significantly delayed in the NWB group. 22 This is because weight restriction prevents micromotion at the fracture site, resulting in unstimulated nonunion. 22 In addition, it has already been reported that WB and exercise are important mechanical stimuli for bone growth and metabolism, 23 suggesting that postoperative WB restriction may prolong bone healing. Nonunion and prolonged healing have also been reported as risk factors for implant failure. 24 While it goes without saying that achieving a good reduction position of the bones after fracture surgery is important, postoperative WB may also be an important factor in bone healing.
In this study, two cutouts occurred in each of the NWB and WB groups; three of the four cases occurred in the early postoperative period, within the first 3 months after surgery. The four cutout cases met at least one of the following criteria: unstable fracture type, poor reduction, and TAD ≥25 mm, consistent with previous reports.6–9
In previous reports, the disadvantages of WB restriction included delayed recovery of walking ability and rehabilitation after surgery.14,20 Jia X, et al reported a significantly longer time to full WB application in the group with WB restriction. 14 Postoperative WB restriction is also associated with increased medical complications and mortality.13,19 In our study, there were no significant differences in medical complications, changes in walking ability, or length of hospital stay. In our hospital, even during WB limitations, rehabilitation actively provided standing training and gait practice using parallel bars. Outside of rehabilitation, the patients were allowed to sit in a wheelchair instead of lying in bed. This is thought to be a factor associated with prevention of occurrence of medical complications. Regarding changes in walking ability, there were no significant differences in this study. Many factors influence the postoperative functional prognosis, including cognitive function, preoperative walking ability, and physical function, 25 and further studies are required.
This study has several limitations. First, it was a retrospective cohort study, and some information may have been collected incompletely. However, patient data were recorded and available in the electronic medical records used at the hospital and, thus, did not differ significantly and did not affect the overall outcome. Second, there might have been unmeasured confounding factors. Although we adjusted for fracture type, intraoperative reduction, and TAD in this study, other factors that were not investigated might have contributed to the occurrence of surgical failures. For example, osteoporosis and osteoporosis drugs. However, BMD was not evaluated in all patients and basically no postoperative osteoporosis treatment was provided. Therefore, we do not believe that this will have a significant impact on the results in this study. The strength of this study is that it measured TAD, which is difficult to measure in large surveys, and analyzed the impact of postoperative load restriction after adjusting for all major risk factors for surgical failure. Third, cases that did not match the criteria were not included in the analysis. In particular, the majority of A2.3 and A3 patients were excluded before and after propensity score matching. Although further study of these fracture types is needed, a certain number of cases with unstable fracture types and poor reduction were included in the analysis, which might not have significantly affected the results. Finally, the study included patients with dementia, and it was unclear whether they were able to comply with NWB instructions. However, several physical therapists were in charge of postoperative rehabilitation, and several nurses assisted with tasks other than rehabilitation, such as transfer to the restroom, which we assumed did not significantly affect the results. To increase the reliability and generalizability of this study, it is necessary to conduct a multicenter, randomized, and large sample survey.
In conclusion, the results of a retrospective cohort study using a PS matching approach showed that WB restriction after TFF surgery could not decrease the incidence of surgical failures, such as cutout. Prospective series are necessary to confirm the results of this retrospective evaluation.
Footnotes
Acknowledgments
We thank to Department of General Affairs in Toyamakensaiseikaitakaoka Hospital for data organization.
An Authorship Declaration
All authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors. All authors are in agreement with the manuscript.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The research protocol was approved by the Institutional Ethics Committee (number 040412-01). The requirement of informed consent was waived.