
Abstract
Background
Total hip arthroplasty (THA) significantly improves the quality of life of patients with end-stage osteoarthritis. Dementia, which is prevalent in geriatric THA recipients, is correlated with several adverse outcomes. This study further investigated the impact of dementia on perioperative outcomes (complications, mortality, skilled nursing facilities [SNFs] transfer, total cost, and length of hospital stay [LOS]) in geriatric patients undergoing elective THA.
Methods
This study retrospectively analysed data from patients aged 65 years and older who underwent elective THA in the Nationwide inpatient sample (NIS) database from 2010 to 2019. Propensity score matching (PSM) was applied to reduce potential selection bias arising from differences in demographic and comorbidity factors. The Wilcoxon rank test (for continuous data) and Chi‒square test (for categorical data) were used to assess demographic characteristics, comorbidities, LOS, total hospital costs, and in-hospital mortality; logistic regression analysis was employed to determine the influence of dementia on adverse outcomes.
Results
376 323 elective geriatric THA patient samples from the NIS database were included, with an overall dementia prevalence of 2.05%. Adverse outcomes following elective THA in patients with dementia included deep vein thrombosis, acute myocardial infarction, acute anaemia, cardiac arrest, urinary retention, urinary tract infection, acute renal failure, pneumonia, respiratory failure, invasive mechanical ventilation, postoperative delirium, gastrointestinal bleeding, mechanical loosening, broken internal joint prosthesis, dislocation, other prosthesis-related complications, wound rupture/unhealed, transfusion, prolonged LOS, increased total cost, and discharge to SNFs.
Conclusion
In elective geriatric THA patients, dementia is independently associated with significantly higher risks of perioperative complications and greater healthcare resource utilization, underscoring the need for enhanced perioperative monitoring and multidisciplinary care for this vulnerable group.
Keywords
Background
Total hip arthroplasty (THA) has evolved into a transformative orthopaedic intervention that markedly improves function and quality of life in patients with end-stage osteoarthritis.1,2 This procedure predominantly serves an aging demographic, with patients over 70 years of age accounting for approximately 50% of cases. 3 In the United States, the number of annual THA procedures is approximately 400 000, with projections indicating an increase to 572 000 by 2030, driven by demographic transitions and surgical innovations. 3 Nevertheless, this major surgical intervention carries significant risks, especially in the geriatric population, where adverse prognostic outcomes such as increased perioperative complications and mortality rates may occur. 4 These challenges have prompted contemporary studies to identify risk factors for complications and develop strategies to improve clinical and prognostic outcomes. 5
Dementia, a progressive cognitive decline disorder, presents a significant challenge in geriatric patients undergoing THA. 6 Several studies have demonstrated that hip surgery patients with dementia experience higher rates of perioperative complications, like pneumonia and postoperative delirium, alongside extended hospital stays and an increased likelihood of requiring long-term care facilities.6–13 However, most existing evidence is derived from hip fracture surgery, which differs substantially from elective THA in clinical aspects. To date, large-scale studies specifically evaluating the independent effect of dementia on outcomes following elective geriatric THA remain limited. Therefore, this cross-sectional study aims to utilize the National Inpatient Sample (NIS) database to address this knowledge gap. The primary outcome of this study was perioperative complications. Secondary outcomes included in-hospital mortality, discharge to skilled nursing facilities (SNFs), hospital costs, and length of stay (LOS).
Methods
Data Source
The NIS database served as the primary data source for this study. Recognized as the largest all-payer inpatient database in the United States, the NIS captures approximately 8 million annual hospitalizations from a nationally representative sample of hospitals. 114,15 It includes detailed information on patient demographics, hospital characteristics, LOS charges, insurance type, and in-hospital mortality. This study was exempt from ethical approval and Institutional Review Board (IRB) review, as it utilizes de-identified data from the publicly available NIS database, in accordance with U.S. federal regulations (45 CFR 46.104(d)(4)).
Study Cohort
We identified 462 318 geriatric patients who underwent elective THA using the International Classification of Diseases, 9th Revision and 10th Revision (ICD-9 and ICD-10) procedure codes (ICD-9: 81.51; ICD-10: 0SR9-X, 0SRB-X) from 2010 to 2019 in the NIS database.
Inclusion criteria were: (1) age ≥65 years and (2) primary THA performed during hospitalization.
Exclusion criteria included: (1) pathological femoral neck fracture, femoral neck fracture, traumatic pelvic fracture, or osteomyelitis; (2) nonelective admission; (3) revision hip arthroplasty; or (4) missing data.
Dementia was identified using ICD-9 and ICD-10 diagnosis codes recorded during the index hospitalization, based on a previously validated code list
16
(Table S1). To minimize selection bias, 1:4 propensity score matching (PSM) was performed (caliper = 0.02; abandonment rate = 0.26%) based on baseline characteristics. After matching, 20 dementia patients were excluded for ineligibility. The final cohort comprised 376 323 patients: 7706 with dementia and 30 615 without (Figure 1). Flow diagram of enrolment and study design
Outcomes
The primary outcome was perioperative complications across multiple organ systems, identified with ICD-9 and ICD-10 codes. To quantify resource consumption, we analysed the total cost and LOS during hospitalization. A prolonged LOS and higher total costs were defined as values exceeding the 75th percentile for the LOS and total cost, respectively. The information regarding whether patients were discharged to SNFs was also retrieved from this database.
Statistical Analysis
To assess statistically significant differences between the cohorts, Wilcoxon rank-sum test was performed for continuous variables, and Chi-square test was performed for categorical variables. To evaluate the associations between dementia and perioperative adverse outcomes, we employed univariable and multivariable logistic regression models. The multivariable model was adjusted for baseline characteristics (including age, gender, race, and type of insurance), hospital characteristics (including bed size, location, region, and teaching status), and preoperative comorbidities. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated using the non-dementia group as a reference. Both unadjusted odds ratios (uORs) and adjusted odds ratios (aORs) are reported. Statistical significance was defined as a two-sided α level of 0.05, which is consistent with other NIS-based studies.17,18
This study was reported in accordance with the strengthening the reporting of observational studies in epidemiology (STROBE) guidelines.
Results
Prevalence of Dementia in Geriatric Patients Undergoing Elective THA
From 2010 to 2019, a total of 462 318 patients aged 65 years and older who underwent elective THA were identified in the NIS database. After applying the exclusion criteria, 376 323 patients were included in the final analysis. Among them, 7706 patients were diagnosed with dementia, resulting in an overall prevalence of 2.05%.
Baseline Characteristics
The median age of dementia patients (79 years) was significantly higher than that of the non-dementia group (72 years; P < 0.001). The sex distribution was significantly different, with a greater proportion of females in the dementia group (63.38% vs 60.59%, P < 0.001). Medicare was the predominant insurance type (92.77% vs 87.47%, P < 0.001), whereas private insurance coverage was significantly lower (5.77% vs 10.99%, P < 0.001).
Demographic Characteristics and Hospital Characteristics of the Study Cohorts

Note. For the continuous variable (age), group comparisons were performed using the two-sided Wilcoxon rank-sum test due to the non-normality of its distribution. For categorical variables, group comparisons were performed using the two-sided Chi-square test.
aSMD, standardized mean difference between the dementia and propensity score-matched non-dementia cohorts.
Comorbidity Burden and Preexisting Conditions
Preoperative Comorbidities of the Study Cohorts

Note. For categorical variables, group comparisons were performed using the two-sided Chi-square test.
aSMD, standardized mean difference between the dementia and propensity score-matched non-dementia cohorts.
After performing 1:4 PSM, all confounding variables listed in Table 1 and Table 2, including age, sex, race, payer type, hospital bed size, hospital location, hospital teaching status and comorbidities, were not significantly different between the dementia and matched non-dementia cohorts. Furthermore, the standardized mean differences (SMDs) for all variables were less than 0.100, indicating an adequate balance between the 2 cohorts (Table 1 and Table 2).
Perioperative Complications
Comparison of Clinical Outcomes Among the Study Cohorts
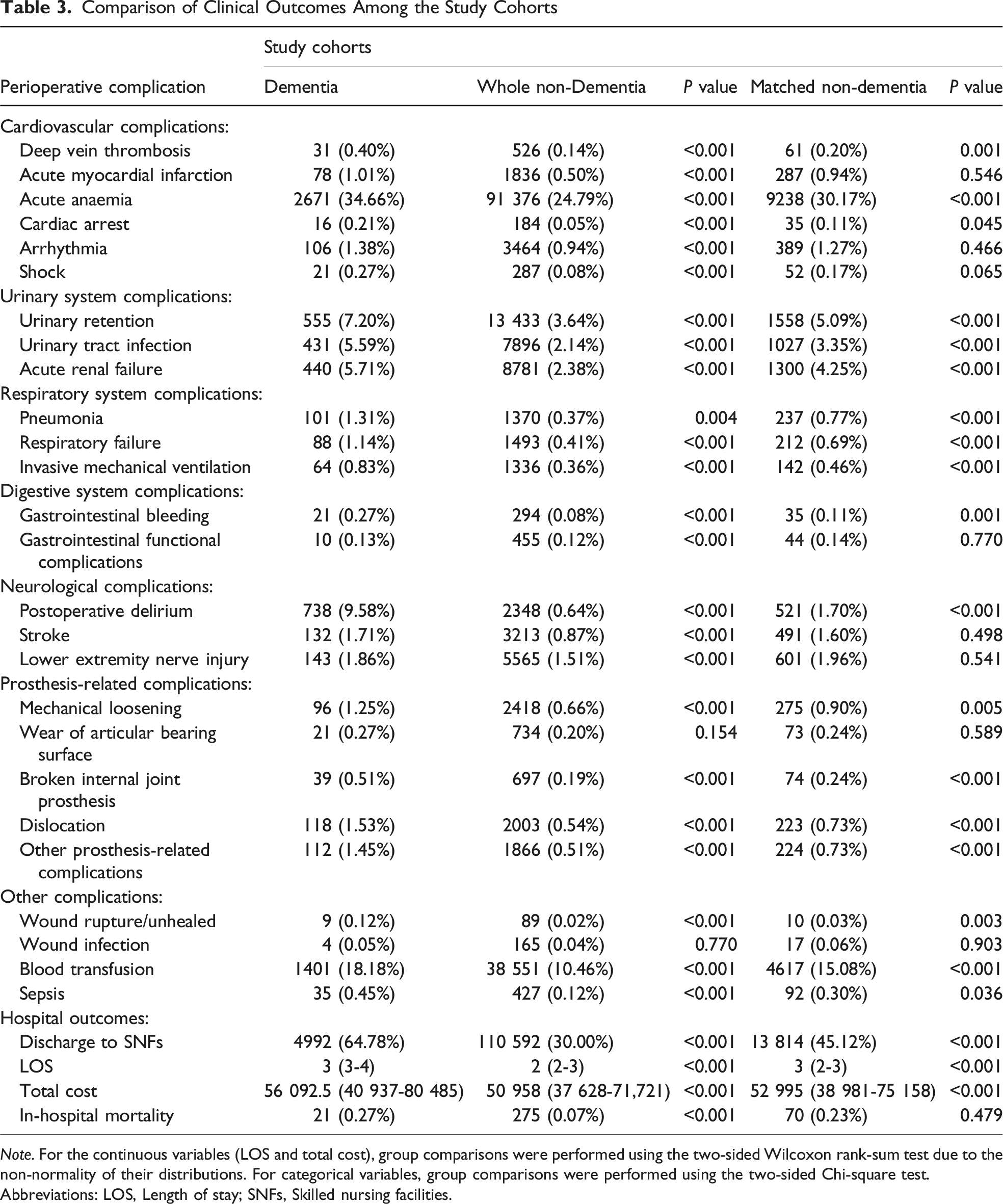
Note. For the continuous variables (LOS and total cost), group comparisons were performed using the two-sided Wilcoxon rank-sum test due to the non-normality of their distributions. For categorical variables, group comparisons were performed using the two-sided Chi-square test.
Abbreviations: LOS, Length of stay; SNFs, Skilled nursing facilities.
Multivariable regression analysis revealed that dementia diagnosis was independently associated with an increased risk of various perioperative complications (Figure 2). Cardiovascular complications included deep vein thrombosis (aOR = 1.958, P = 0.002) and acute myocardial infarction (aOR = 1.221, P < 0.001). Urinary system complications were more common, with higher risks of urinary retention (aOR = 1.434, P < 0.001), urinary tract infections (aOR = 1.683, P < 0.001), and acute renal failure (aOR = 1.339, P < 0.001). Respiratory complications, including pneumonia (aOR = 1.631, P < 0.001), respiratory failure (aOR = 1.634, P < 0.001), and acute traumatic ventilation (aOR = 1.763, P < 0.001), were also significantly elevated. Gastrointestinal bleeding was more prevalent in the dementia group (aOR = 2.348, P = 0.002). Postoperative delirium was strongly associated with dementia (aOR = 6.127, P < 0.001). Prosthesis-related complications included increased risks of mechanical loosening (aOR = 1.384, P = 0.006), broken internal joint prosthesis (aOR = 2.069, P < 0.001), dislocation (aOR = 2.093, P < 0.001), and other prosthesis-related complications (aOR = 1.975, P < 0.001). Other notable complications included blood transfusion (aOR = 1.239, P < 0.001), wound rupture/unhealed (aOR = 3.572, P = 0.006) and blood transfusion (aOR = 1.239, P < 0.001). Unadjusted/adjusted odds ratios of clinical outcomes. Odds ratios (ORs) and 95% confidence intervals (CIs) were obtained from logistic regression models. P values were calculated using two-sided Wald tests. All tests were two-sided.
Resource Consumption
While the median LOS was 2 days in both groups, patients with dementia presented a significantly greater risk of prolonged hospitalization (aOR = 1.873, P < 0.001). Additionally, dementia was associated with increased median total hospitalization costs ($56 092.5 vs $50 958, P < 0.001).
In-hospital mortality rates were initially higher in the dementia group (0.27% vs 0.07%, P < 0.001) in the unmatched analysis. However, this difference became nonsignificant after PSM and multivariate adjustment (aOR = 1.115, P = 0.663).
The presence of dementia was significantly associated with higher rates of discharge to SNFs. A total of 64.78% of patients with dementia required SNF care, whereas 30.00% of non-dementia patients did (P < 0.001). This difference persisted after PSM (64.78% vs 45.12%, P < 0.001) and multivariate adjustment (aOR = 2.341, P < 0.001).
Discussion
This cross-sectional study conducted a large-scale health economic analysis utilizing NIS database, aiming to determine the impact of dementia on hospitalization outcomes in geriatric patients undergoing elective THA. We examined 376 343 elective geriatric THA patients from the NIS database between 2010 and 2019, among whom 2.05% were registered as having dementia, a prevalence rate comparable to that reported in studies using the same database. 18 Dementia was significantly associated with adverse outcomes following elective THA in geriatric patients, especially increased risk of various complications, including cardiovascular complications (deep vein thrombosis, acute anaemia, acute myocardial infarction), urinary system complications (urinary retention, urinary tract infection, acute renal failure), respiratory system complications (pneumonia, respiratory failure, acute traumatic ventilation), gastrointestinal bleeding, postoperative delirium, prosthesis-related complications (mechanical loosening, broken internal joint prosthesis, dislocation, and other prosthesis-related complications), wound rupture/unhealed, blood transfusion, and sepsis. In addition, dementia was independently associated with higher rates of transfer to SNFs, prolonged LOS, and increased total hospital costs.
We found that dementia increased the risk of deep vein thrombosis and stroke in geriatric patients after THA. Therefore, patients with dementia face a greater risk of thromboembolism after surgery. Postoperative care for these patients should include early lower extremity mobilization, individualized anticoagulation therapy, and multidisciplinary collaborative management to reduce the occurrence of thromboembolic events. 19 Moreover, dementia was significantly associated with perioperative cardiovascular complications, including acute myocardial infarction, arrhythmia, cardiac arrest, and shock. Previous studies have also revealed a significant association between cognitive impairment in geriatric surgical patients and adverse cardiovascular outcomes. 20 Research has indicated that myocardial infarction events are related to cognitive decline, and cognitive dysfunction shares common cardiovascular risk factors with acute myocardial infarction, both becoming increasingly prevalent in the geriatric population. Therefore, preoperative dementia may lead to an increased incidence of complications such as arrhythmia and myocardial infarction. 21
In our study, we found that dementia was a significant risk factor for urinary system complications, including urinary retention, urinary tract infections, and acute renal failure. Urinary retention may cause urine reflux, affecting the renal mucosal microenvironment and further increasing the possibility of kidney injury. 22 Factors such as urinary tract infections can also lead to acute kidney injury.
Postoperative delirium is a common and serious complication following joint arthroplasty. This acute brain dysfunction typically manifests as fluctuating changes in attention, consciousness level, and cognitive function.23,24 Our study demonstrated that patients with preexisting dementia had a significantly greater incidence of postoperative delirium than non-dementia patients did (10.7% vs 0.4%). The increased incidence of postoperative delirium in patients with preexisting dementia is not surprising, as even seemingly minor trauma can be sufficient to trigger delirium in dementia patients. 23 In contrast, for patients without dementia, postoperative delirium typically occurs only after experiencing a series of significant stressors, such as general anaesthesia, major surgery, or ICU admission. 25 Accordingly, routine preoperative delirium risk stratification, together with postoperative multicomponent non-pharmacological interventions and orthogeriatric co-management, may lower postoperative delirium rates and improve outcomes in dementia patients.26,27
Hu Chaorong et al reported that surgical patients with preexisting dementia were more prone to pneumonia, a major postoperative complication, than patients without dementia. 28 This finding aligns with our study, which revealed significantly higher rates of postoperative pneumonia in dementia patients than in non-dementia patients. Similarly, we found that dementia was also a risk factor for other pulmonary complications, including acute respiratory failure and traumatic mechanical ventilation. The increased risk may be attributed to dementia patients’ inability to communicate effectively, which can limit their participation in pulmonary function exercises and early mobilization. Additionally, their difficulties in expressing pain and swallowing problems often result in poor rehabilitation compliance, potentially further increasing the risk of pneumonia and acute respiratory failure. 29 Given these elevated risks, postoperative care for patients with dementia may benefit from several strategies, including early swallow screening and oral care, pulmonary rehabilitation program, and early mobilization, to mitigate respiratory complications.30,31
Severe complications may occur with implanted prostheses postoperatively and are often associated with prosthesis-related complications such as periprosthetic joint infection, mechanical loosening of the prosthesis, dislocation, and periprosthetic fractures. 32 Previous studies reported that among patients who underwent hemiarthroplasty, those with dementia presented a greater risk of prosthetic dislocation (OR = 1.87) and periprosthetic fractures (OR = 1.29) within the first year after surgery. However, no significant increase in the risk of periprosthetic joint infection or aseptic loosening was observed. 33 In our cohort study on elective THA, dementia significantly increased the risk of prosthetic dislocation and periprosthetic fractures during hospitalization, which is consistent with previous findings. This may be attributed to abnormal behaviour and noncompliance with postoperative protocols, as well as cognitive impairment and muscle weakness, which may predispose patients to an elevated risk of dislocation. 34 However, in our study, the incidence of periprosthetic joint infection was also greater in dementia patients, which contrasts with earlier research. This discrepancy may be due to differences in surgical technique. Therefore, postoperative rehabilitation for these patients should be given high priority, as it could improve functional recovery and reduce the incidence of prosthesis-related complications.35,36
Zerky et al demonstrated that dementia is a predictive factor for discharge to nursing facilities in hospitalized geriatric patients in both acute and geriatric rehabilitation hospitals. 37 In our study, the proportion of dementia patients transferred to specialized care facilities was 64.78%, whereas it was 45.12% for non-dementia patients. Owing to cognitive impairment and multiple comorbidities, dementia patients are more likely to be transferred to specialized care facilities, highlighting the multifaceted challenges in postoperative care management and the increased need for additional support. 38
In our study, we found no significant difference in in-hospital mortality between patients with dementia and those without dementia following THA. This finding aligns with several previous studies. Yong-Chan Ha et al, in their study of geriatric hip fracture patients (150 dementia patients vs 2196 non-dementia patients), reported no significant difference in 30-day mortality rates between the 2 groups. 9 Similarly, Mayur Sharma et al reported no significant difference in in-hospital mortality rates between cohorts with and without dementia undergoing spine fusion procedures. 39 The non-significant association may be attributed to the fact that postoperative mortality rates following hip surgery tend to increase over time, making it difficult to detect the impact of dementia during relatively brief hospital stays. However, some studies have demonstrated that dementia is an independent risk factor for long-term mortality following hip surgery.10,36,40 This finding emphasizes the importance of healthcare teams thoroughly considering the potential impact of dementia on long-term outcomes during both preoperative assessment and perioperative management.
Patients with dementia encounter greater challenges in perioperative rehabilitation. The LOS is a key determinant of hospitalization costs following THA, and there is a significant association between the LOS and discharge to SNFs. Studies have reported that the longer the hospital stay is, the greater the likelihood of patients being discharged to SNFs.37,38 Given the increased rehabilitation needs of patients with dementia, their LOS is often prolonged, which further exacerbates the consumption of medical resources. Therefore, several studies recommend implementing close follow-up early in the postoperative period for patients with dementia, along with proactive communication with internal medicine or geriatric specialists within bundled payment models, as these strategies may help prevent complications, enhance care quality, and reduce overall costs.6,8
Beyond the aforementioned perioperative multidisciplinary protocols, routine preoperative cognitive screening using tools such as the Mini-Mental State Examination (MMSE) or Mini-Cog is recommended for geriatric patients undergoing THA. This approach can facilitate early risk stratification, inform shared decision-making and anesthesia planning, and may help prevent common adverse outcomes.41,42
Like other large-scale database analyses, this study is subject to certain inherent limitations29,43: (1) potential underestimation of the incidence rates of various perioperative outcomes due to coding discrepancies and data entry errors; (2) lack of follow-up records after discharge, making it challenging to assess the long-term impact of dementia on clinical outcomes; (3) absence of biochemical test results, detailed surgical information, and perioperative medication data, which limited comprehensive regression adjustments and may have introduced residual confounding in evaluating dementia’s perioperative impact; and (4) no formal power analysis was performed, as this study relied on all samples available in the NIS database who met the inclusion and exclusion criteria. As a cross-sectional analysis, the data in this study may be insufficient to comprehensively verify the impact of dementia on the outcomes of elective THA in geriatric patients. Further prospective studies are warranted for in-depth exploration.
Conclusion
In geriatric patients undergoing elective THA, dementia is linked to greater perioperative complications, longer LOS, higher costs, and an increased likelihood of discharge to SNFs. Although there was no significant correlation between in-hospital mortality and dementia after PSM, these adverse outcomes highlight the need for healthcare providers to strengthen preoperative risk assessment for patients with dementia and optimize perioperative multidisciplinary management, thereby improving clinical outcomes and healthcare resource utilization.
Supplemental Material
Supplemental Material - Effects of Dementia on Adverse Outcomes in Geriatric Patients Undergoing Elective Total Hip Arthroplasty: Analysis of the US Nationwide Inpatient Sample
Supplemental Materia for Effects of Dementia on Adverse Outcomes in Geriatric Patients Undergoing Elective Total Hip Arthroplasty: Analysis of the US Nationwide Inpatient Sample by Bofei Dong, Junhao Lin, Xinlin Huang, Qinfeng Yang, Lu Tao and Xiaolong Hu in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Ethical Considerations
This observational study involved the analysis of deidentified publicly available human data. The study was conducted in accordance with the ethical principles of Declaration of Helsinki.
Consent to Participate
The requirement for informed consent was waived due to the non-interventional nature of the research and the use of deidentified data. Given the use of deidentified public data, there was no requirement for obtaining informed consent from participants.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, analysis and interpretation were performed by BFD, JHL and XLH. The first draft of the manuscript was written by BFD and JHL with revision, guidance and feedback from QFY, LT and XLH. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. All authors agree to be accountable for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the President Foundation of Nanfang Hospital, Southern Medical University (2024A036), Medical Scientific Research Foundation of Guangdong (B2025509), and Open Funding Project of Jiangxi Provincial Key Laboratory of Precision Therapy for Cells (Jiujiang College) (JJ2025002).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors state that their research data will be made available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.