
Abstract
Objective
To identify the risk factors associated with prolonged length of stay (LOS) despite an enhanced recovery after surgery (ERAS) protocol in short-level lumbar fusion surgery.
Methods
We gathered data for all patients undergoing short-level lumbar fusion surgery from January to November 2021. Given the discharge criteria, a threshold was set according to mean LOS, and two groups were spontaneously formed: LOS shorter than the threshold for discharge (control group, n = 114) and LOS longer or equal to the threshold for discharge (delayed group, n = 72). Preoperative metrics were compared to identify risk factors associated with prolonged LOS.
Results
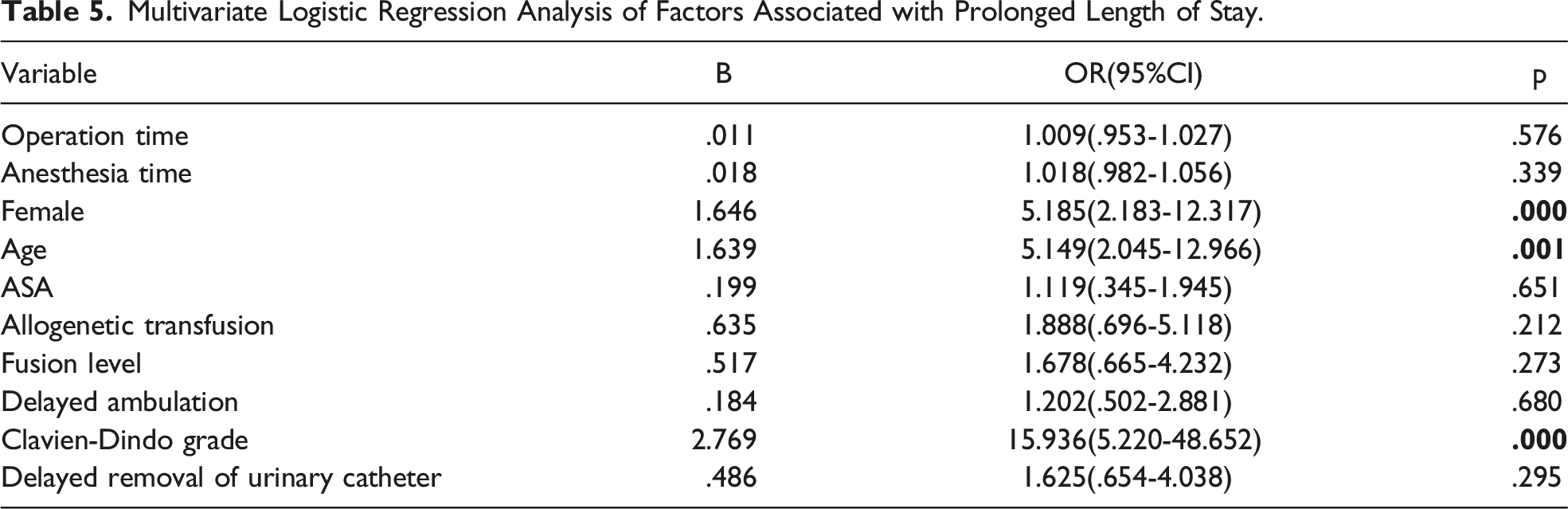
A total consecutive 186 patients with complete medical records were enrolled (77 males and 109 females; mean age 71.08 ± 5.70 years). After dichotomization according to the threshold for discharge, there were 114 patients in control group and 72 in delayed group. Statistical analysis demonstrated that age ≥75 years (P = .002), female sex (P < .001), American Society of Anesthesiologists grade ≥ 3 (P = .035), operation time (P < .001), anesthesia time (P < .001), ambulation time >1 day (P = .027), removal of urinary catheter time >1 day (P = .019), fusion levels (P < .001), Clavien-Dindo grade > 1 (P <.001) and allogeneic transfusion (P = .009) were significantly related to prolonged LOS. Binary logistic regression revealed that age (odds ratio (OR) 5.149; 95% confidence interval (CI) 2.045-12.966, P = .001), sex (OR 5.185, 95% CI 2.183-12.317, P < .001) and Clavien-Dindo grade > 1(OR 15.936, 95% CI 5.220-48.652, P < .001) were independent risk factors of prolonged LOS.
Conclusions
In this retrospective study, we analyzed the potential risk factors associated with delayed LOS despite implementing ERAS, further, binary logistic regression exhibited that age ≥75 years old, female sex and Clavien-Dindo grade >1 were independently correlated with prolonged LOS.
Introduction
Kehlet proposed enhanced recovery after surgery (ERAS) in 1997, 1 which provides a multimodal, multidisciplinary management strategy.2,3 The primary purpose of ERAS is to reduce postoperative adverse events and accelerate recovery by decreasing stress responses, shortening the length of stay (LOS) and hospitalization costs.2,4 Compared with conventional perioperative care, ERAS has demonstrated its superiority in reducing postoperative complications and LOS.5-9 While ERAS has been widely applied in many surgical fields, 10 its use in spine surgery is in an early stage. 7
Although there is a reduction in LOS and lower complication rates, specific patients cannot be discharged as quickly as expected despite ERAS, demonstrating that there were potential risk factors related to prolonged LOS. Hence, it is critical to elucidate the risk factors and implement customize perioperative management stratege. Previous studies reported satisfactory results after implementing ERAS in spine surgery2,11,12; however, few studies report the risk factors correlated with prolonged LOS despite ERAS for short-level lumbar fusion surgery. Therefore, this study aimed to identify the perioperative prognostic risk factors associated with prolonged LOS and to identify customized prophylaxis protocols to facilitate function recovery and earlier discharge.
Patients and Methods
Study Design
Enhanced Recovery After Surgery Items for Short Level Lumbar Fusion Surgery.

Baseline Characteristics of all Patients (n = 186).

BMI: body mass index; EBL: estimated blood loss; ASA: American Society of Anesthesiologists grade; LOS: length of stay; ODI: Oswestry Disability Index; VAS: visual analog scale.
Statistical Analysis
Continuous variables were expressed as mean value ± standard deviation for normally distributed data. For non-normally-distributed data, the median and interquartile range was used. Categorical variables were expressed using proportions. Continuous variables were analyzed using the two-sample T-test, while statistical analysis for categorical variables was performed using the Chi-square test or the Fisher exact test. Binary logistic regression for multivariate analysis was used to identify the independent risk factors of prolonged LOS. All statistical analyses were performed using SPSS software version 25.0 (SPSS, Inc, Armonk, NY, USA), and P-values <.05 were considered statistically significant.
Results
Demographic Data
A total consecutive 186 patients were enrolled (77 males and 109 females; mean age 71.08 ± 5.70 years; mean BMI 25.65 ± 3.63 kg/m2; operation time and anesthesia time were 187.61 ± 55.94 mins and 246.88 ± 58.35 mins, respectively). There were 84 patients with one fusion level and 102 patients with two fusion segments. The mean EBL was 247.43 ± 199.20 mL. Twenty-eight received an allogeneic transfusion. There were 22 patients with preoperative albumin levels lower than 35 g/L and 13 patients with preoperative hemoglobin levels lower than the standard value, respectively. The preoperative Oswestry disability index was 52.68 ± 3.12, and the preoperative visual analog scale for back and leg were 5.04 ± 1.48 and 5.63 ± 1.53, respectively. The detailed demographic data are displayed in Table 2.
Risk Factors for Prolonged Length of Stay.
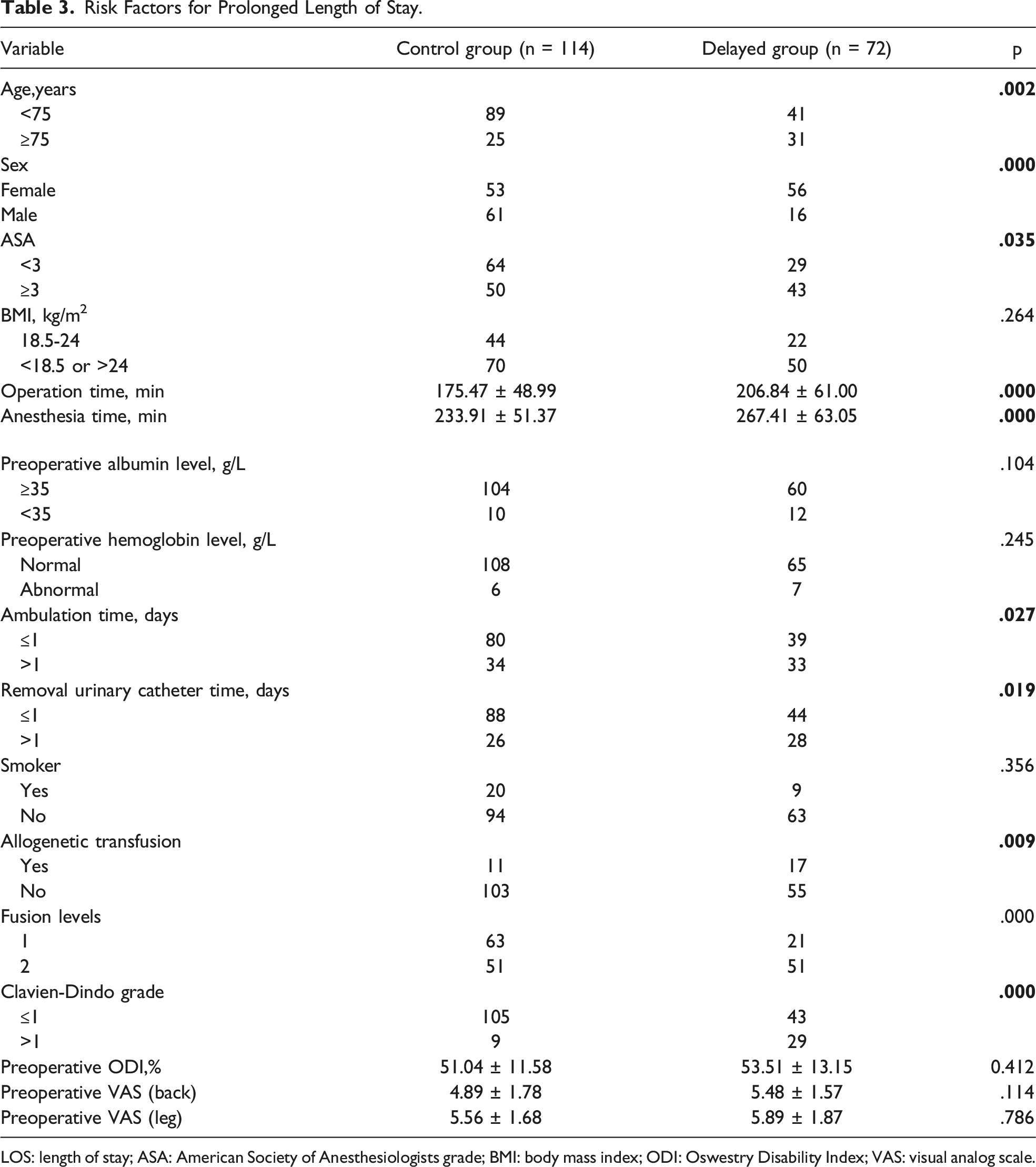
LOS: length of stay; ASA: American Society of Anesthesiologists grade; BMI: body mass index; ODI: Oswestry Disability Index; VAS: visual analog scale.
Compliance With the ERAS Protocol
Compliance to Enhanced Recovery After Surgery Pathway.

Risk Factors for Prolonged LOS
Multivariate Logistic Regression Analysis of Factors Associated with Prolonged Length of Stay.
Discussion
Substantial attention has been paid to the effects of compliance with ERAS and the reduction of LOS.17-19 To our knowledge, few studies are focusing on the risk factors associated with prolonged LOS in short-level lumbar fusion surgery despite the implementation of ERAS protocol. In our study, we found that age
In a retrospective cohort study, Li et al showed elderly patients with comorbidities are at a higher risk for complications after lumbar spine surgery. 20 Analogously, in a retrospective analysis of 585 patients who underwent lumbar spine surgery, Kanaan et al found male patients walked significantly longer distance than female patients, although clinically insignificant. 22 In our study, we found that age older than 75 years and females were independently related to prolonged LOS despite ERAS, which reminds us of the importance of age and gender on postoperative complications, and more attention should be paid to these patients in perioperative management to prevent postoperative complications.
The increasing proportion of the aging population is generally associated with comorbidities and the postoperative complication rate following lumbar fusion surgery.23,24 ERAS results in shorter LOS and fewer postoperative complications than conventional perioperative care.5,10,25,26 Although ERAS has been widely applied in other surgical fields, its implementation in spine surgery, though promising, is still in the early stages. 7 In a retrospective propensity score matching, D’Astorg et al revealed that the ERAS protocol decreased the hospital LOS (2.6 vs 4.4 days, P < .0001), while postoperative complications were similar in two groups. 11 In current study, according to Clavien-Dindo complication grade, we found patients with delayed LOS had more severe postoperative complications (P < .001, Table 3), and Clavien-Dindo grade > 1 was independently correlated with prolonged LOS (Table 5). What’ more, it is worth noting that despite meticulous preoperative nutritional care and early oral feeding, there were 123 patients with postoperative hypoproteinemia (Table 2). According to previous studies, preoperative nutritional status is critical for recovery after major surgery and correlated with postoperative complications and prolonged LOS,27,28 therefore, it is essential to take additional measures to prevent severe postoperative hypoproteinemia.
Patients must actively participate in ERAS programs even though there may be reduced compliance with specific ERAS items. 7 In our study, the items with lower compliance were ambulation on POD 1 (63.9%) and removal of bladder catheter on POD 1 (70.9%). Previously, because of the reduction of bladder function and the longer functional recovery of spine surgery, few studies explicitly illustrated the time of ambulation and removal of a bladder catheter and only stressed the concept of early ambulation and early removal of the bladder catheter.29,30 Given the adverse events associated with prolonged bed rest and the importance of early ambulation in reducing LOS,29,31 attention should also be paid to adverse events related to prolonged urinary drainage (urinary tract infections and surgical site infections).32,33 In a before and after cohort study on elderly patients who underwent elective spine and peripheral nerve surgery, Ifrach et al 34 showed improved mobilization and ambulation on POD 0 in ERAS group, and proved the safety and feasibility of early mobilization and ambulation in this population. In the present study, patients were explicitly requested to ambulate and remove the bladder catheter on POD 1 unless there were contraindications. Only one patient developed urinary retention (Table 2) in 132 patients (Table 3) who had the bladder catheter removed on POD 1, and there were no adverse events associated with early mobilization.
The present study has several limitations. First, this was a monocentric, retrospective study, and there were some offsetting and confounding factors. Second, the small sample size limits the robustness of our findings. Thirdly, due to the characteristic of spine surgery, the severe stress response and longer functional recovery, and the feature of the elderly population, patients with more than two fusion levels were excluded. This decision may have introduced selection bias. Finally, the imbalance of distribution of fusion levels between two groups may be the results of current study, hence, studies with comparable fusion levels are needed to further explore the risk factors associated with prolonged LOS.
Conclusion
In this retrospective study, we analysed the potential risk factors associated with delayed LOS despite implementing ERAS, further, binary logistic regression exhibited that age ≥75 years old, female sex and Clavien-Dindo grade >1 were independently correlated with prolonged LOS.
Footnotes
Acknowledgments
We thank the Department of Orthopedics, Xuanwu Hospital Capital Medical University staff and all the patients who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Beijing Municipal Medical Science Institute-public Welfare Development Reform Pilot Project: (Capital Medical Research No.2019-2).
Ethical Approval
The institutional review board in Xuanwu Hospital Capital Medical University approved the study (No. 2018086), which followed the Declaration of Helsinki principles.
Informed Consent
A written informed consent was obtained from all participates of this study.