
Abstract
Objective
To evaluate the application of an enhanced recovery after surgery (ERAS) protocol in patients undergoing robot-assisted laparoscopic prostatectomy (RALP).
Methods
We conducted a retrospective cohort study of 136 patients who underwent RALP between August 2017 and June 2018 as the control group and a prospective analysis of 106 patients who underwent RALP between January 2019 and January 2020 as the ERAS group. ERAS focused on preoperative education, nutritional intervention, electrolyte solution intake, restrictive fluid infusion, body warming, no indwelling central venous catheter, use of nonsteroidal anti-inflammatory drugs (NSAIDs), early mobilization, and eating recovery.
Results
The times from RALP to the first intake of clear liquid; first ambulation; first defecation; first fluid, semi-liquid, and general diet; drain removal; and length of hospital stay (LOS) were significantly shorter, and operative time, fluid infusion within 24 hours, postoperative day (POD) 1 albumin, POD 1 hemoglobin, and POD 2 drainage were significantly higher in the ERAS group. Five patients (3.8%) in the ERAS group developed postoperative complications (urine leakage, n = 4; intestinal obstruction, n = 1), while 1 patient (0.7%) in the control group developed intestinal obstruction.
Conclusions
ERAS effectively accelerated patient rehabilitation and reduced the LOS for patients undergoing RALP.
Keywords
Introduction
Prostate cancer is the most common cancer of the genitourinary tract in men. 1 In China, the incidence of prostate cancer is 60.3 per 100,000. 2 With widespread application and increasing experience, robot-assisted laparoscopic prostatectomy (RALP) has become an increasingly popular minimally invasive choice among urologists for managing localized prostate cancer. 3 , 4 However, these procedures involve major surgical resection, increased risk of bleeding and perioperative transfusion, and in cases of cystectomy, urinary diversion and a high frequency of postoperative complications. Furthermore, patients undergoing RALP are usually older, with cardiovascular and other comorbidities, anemia, possible infection, and malnutrition.
ERAS was first reported by the Danish surgeon Kehlet, 5 and involves evidence-based optimization of a series of perioperative treatment procedures that aim to reduce the physical and psychological stress of surgical trauma and thus, accelerate the patient’s rehabilitation. 6 ERAS programs can significantly reduce the length of hospital stay and the time to ambulate, defecate, and flatus in patients undergoing colorectal, 7 , 8 bariatric, 9 orthopedic, and gynecological surgery,10,11 as well as esophagectomy, 12 and even RALP, 13 , 14 increasing clinical efficacy and safety. There is currently an increased interest in ERAS protocols in urology.
Although Jiang and Li introduced and promoted ERAS in China in 2007, 3 its integration into urological surgery has been relatively slow. There remains a lack of well-recognized studies exploring the clinical efficacy and safety of an ERAS protocol in RALP, which has hindered wide application in patients with prostate cancer.
In this study, the evidence and guidelines in Chinese and English databases were systematically searched, a quality evaluation and summary were performed, and indices of the perioperative ERAS protocols in RALP were preliminarily formulated. We evaluated the clinical efficacy and safety of ERAS in patients undergoing RALP regarding operative time, blood loss, postoperative day (POD) 1 albumin, POD 1 hemoglobin, postoperative drainage, and complications, compared with conventional care.
Materials and methods
ERAS protocol development
We performed a comprehensive literature review using the following databases: BMJ Best Practice, Ovid JBI EBP, Cochrane library, EBSCO Medline, PubMed, Elsevier, NGC, RNAO, SIGN, NICE, Wanfang, and CNKI, to screen published articles reporting the outcomes of applying the ERAS protocol in RALP patients. The following Medical Subject Heading (MeSH) search terms were used: [“fast track surgery” OR “fast-track rehabilitation” OR “enhanced recovery protocol” OR “enhanced recovery after surgery”] AND [“prostate cancer” OR “prostatic cancer” OR “prostatectomy” OR “radical prostatectomy”]. To identify studies that may have been missed, we reviewed the reference lists of all related articles and published abstracts. A total of 712 English-language studies or evidence and 59 Chinese studies or evidence were identified; 669 studies with unrelated topics and 80 duplicates were excluded, leaving 21 studies for inclusion. The studies comprised 12 clinical practice guidelines,15–26 7 JBI evidence summaries,27–33 and 2 recommended practices. 34 , 35 According to the classification and recommendation of evidence-based medicine, 13 evidence-based articles were finally included in the study.
Patients
The writing of this report followed the CONSORT guidelines. The inclusion criteria were: age: 18 to 85 years, good physical condition, prostate cancer confirmed by preoperative prostate tissue biopsy, and undergoing RALP. The exclusion criteria were: emergency surgery; severe cardiovascular disease, pulmonary dysfunction, severe hemorrhagic tendency, or blood clotting disorders that significantly increased the surgical risk; body mass index (BMI) >30 kg/m2 or patients with a score of 3 points on the nutritional risk screening form 2002 (NRS 2002), and lack of written consent.
We retrospectively analyzed patients who underwent RALP between August 2017 and June 2018 and prospectively analyzed patients who underwent RALP between January 2019 and January 2020 in a prestigious urology center in Shanghai (ranked 2nd in China). The effects on perioperative outcomes of the patients’ demographic data, recovery condition, and quality of care were examined by comparing patients receiving conventional care with patients receiving the ERAS protocol. The principles of conventional care and the ERAS protocol are listed in Table 1.
Protocols in the ERAS and control groups.
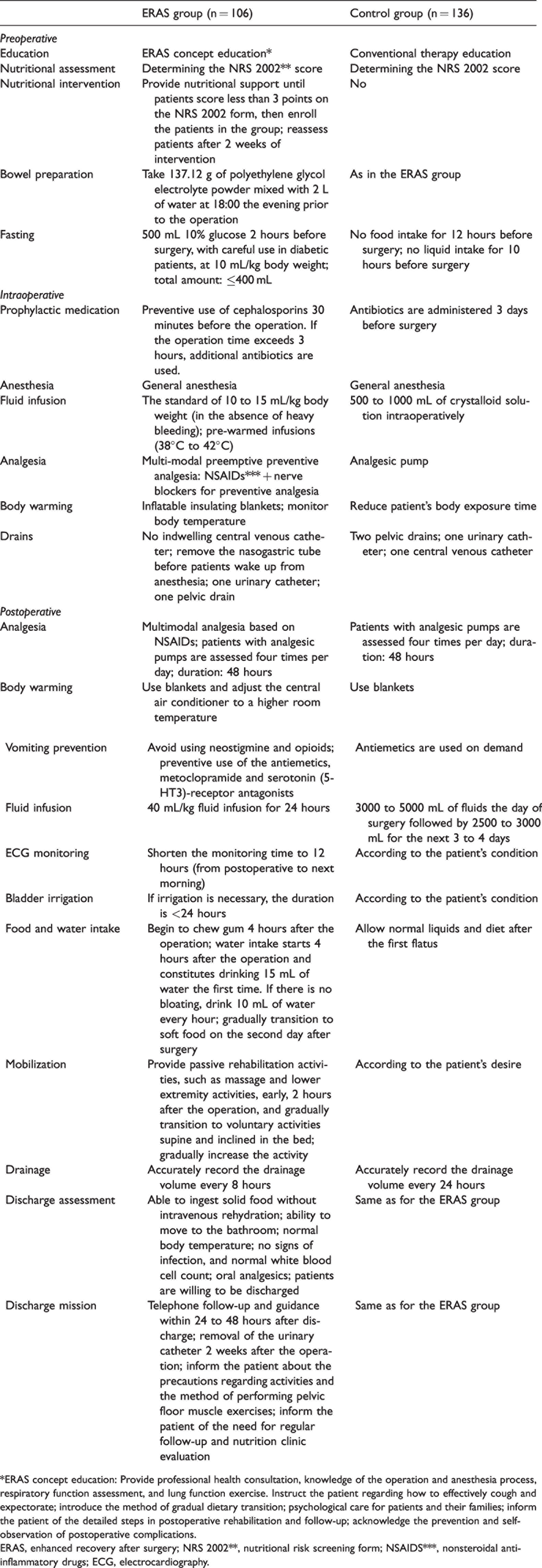
*ERAS concept education: Provide professional health consultation, knowledge of the operation and anesthesia process, respiratory function assessment, and lung function exercise. Instruct the patient regarding how to effectively cough and expectorate; introduce the method of gradual dietary transition; psychological care for patients and their families; inform the patient of the detailed steps in postoperative rehabilitation and follow-up; acknowledge the prevention and self-observation of postoperative complications.
ERAS, enhanced recovery after surgery; NRS 2002**, nutritional risk screening form; NSAIDS***, nonsteroidal anti-inflammatory drugs; ECG, electrocardiography.
This study was part of a research project titled “Building and Empirical Study of a Multidisciplinary Precise Rehabilitation Model for Surgical Patients with Prostate Cancer Based on an Intelligent Medical Platform”, which received Institutional Review Board (IRB) approval from Changhai Hospital (approval No. CHEC2020-111). In this study, we adhered to the following ethical principles: respect, competence, responsibility, and integrity. Before each interview in the prospective section of this study, interviewees were given information about the study, and voluntary participation and the confidential handling of all data were discussed. Then, patients and their family members provided written informed consent for participation and the use of their clinical data in publications. Medical and nursing faculty also provided written informed consent for participation.
We retrospectively registered this trial in the Chinese Clinical Trial Registry http://www.chictr.org.cn/ (registration number: ChiCTR2100047730).
Conventional care
All patients were instructed to fast for 12 hours before the surgery and perform bowel preparation at 18:00 the day before surgery. An analgesic pump was used intraoperatively. Postoperatively, all patients received standard fluid therapy, and their mobilization depended on their own desire.
ERAS protocol
The ERAS protocol comprised preoperative, perioperative, and postoperative considerations.
Patients in the ERAS group received comprehensive preoperative education comprising knowledge of the operation and anesthetic process, and the ERAS concept, and all underwent respiratory function assessment and lung function exercise. We gave specific guidance regarding appropriate dietary recovery, psychological care for patients and their families, and acknowledged the prevention and self-observation of postoperative complications during hospitalization. We also provided nutritional support for patients with substandard diets and reassessed patients after 2 weeks of intervention.
Patients ingested 137.12 g of polyethylene glycol electrolyte powder mixed with 2 L of water at 18:00 the evening prior to the operation. Patients also received 500 mL of 10% glucose 2 hours before surgery (careful use in diabetic patients). Prophylactic cephalosporins were administered 30 minutes before the operation; additional antibiotics were added if the operation time exceeded 3 hours.
The fluid infusion volume was limited to 10 to 15 mL/kg body weight (in the absence of heavy bleeding) intraoperatively. We combined nonsteroidal anti-inflammatory drugs (NSAIDs) and nerve blockers as preventive analgesia and kept the patients’ bodies warm via inflatable insulation blankets, temperature monitoring, and pre-warmed infusions (38°C–42°C) intraoperatively. The central venous catheter and orogastric tube were removed before patients woke up.
Next, we addressed postoperative analgesia, body warming, and vomiting prevention. Fluid infusion during the first 24 hours was reduced to 40 mL/kg, and postoperative pain was measured using a visual analogue scale (VAS).
Electrocardiographic (ECG) monitoring time and bladder irrigation were shortened to less than 24 hours. Patients drank 15 mL of water for the first time 4 hours after the operation and 10 mL of water every hour thereafter if there was no bloating. Each patient’s diet was gradually transitioned to soft food on the second day after surgery. Passive rehabilitation exercises were performed early, 2 hours after the operation; we encouraged patients to try voluntary activities as soon as possible.
Complication observation
Patients were monitored postoperatively for intestinal obstruction during hospitalization. Urine leakage was defined as urine leaking from the urethra into the pelvic cavity caused by insufficiency of the vesicourethral anastomosis, which was diagnosed by an abnormal increasing trend in the fluid drainage volume. We generally measured creatinine concentration in the drainage fluid to diagnose this issue, and cystography was not usually performed.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows, version 19.0 (IBM Corp., Armonk, NY, USA). Quantitative variables with symmetrical distribution were expressed as mean and standard deviation and were compared using Student’s t test for independent samples. Categorical variables were analyzed using the Chi-square test or Fisher’s exact test. The Mann–Whitney U test was used for variables with asymmetrical distribution. P values <0.05 were considered statistically significant. A sample size calculation was performed using PASS 11 (NCSS, Kaysville, Utah, USA). Group sample sizes of 40 and 40 achieved 91% power to detect a difference of −1.0 between the null hypothesis that both group means were 4.0 and the alternative hypothesis that the mean of group 2 was 5.0 with estimated group standard deviations of 1.5 and 1.5, respectively, and with a significance level (alpha) of 0.05000 using a one-sided two-sample t-test.
Results
We initially identified 245 patients; 1 was older than 89 years, and 2 patients had NRS 2002 scores of 3 points. These three patients were excluded from the study. Of the remaining 242 patients, 136 patients undergoing RALP were retrospectively analyzed, and 106 patients undergoing RALP were prospectively analyzed. The patients’ demographic and preoperative clinical data are shown in Table 2. No significant differences in age, BMI, prostate-specific antigen (PSA) concentration, pathological tumor stage, biopsy Gleason score, and hemoglobin (Hb) or albumin (Alb) concentrations were observed between the two groups (Table 2).
Preoperative characteristics of the patients in the control and ERAS groups.

*Values are expressed as mean ± standard deviation.
**Statistical tests: chi-square test for categorical data and the Mann–Whitney U or t test for continuous data.
ERAS, enhanced recovery after surgery; PSA, prostate specific antigen; BMI, body mass index; Alb, albumin; Hb, hemoglobin; p, pathological stage; T, tumor stage.
There were no significant differences in blood loss, or POD 1 and POD 3 drainage volumes between the two groups. The POD 1 Alb and Hb concentrations, operative time, and fluid infusion volumes within 24 hours in the ERAS group were higher than in the control group (all P < 0.05). Compared with the control group, the patients in the ERAS group had lower fluid infusion volumes within 48 hours and after 48 hours (all P < 0.05). Additionally, the POD 2 drainage volume in the ERAS group was more than that in the control group (P < 0.05) (Table 3).
Postoperative outcomes of the patients in the control and ERAS groups.

*Values are expressed as mean ± standard deviation.**Statistical test: Mann–Whitney U test for continuous data.
ERAS, enhanced recovery after surgery; POD, postoperative day; Alb, albumin; Hb, hemoglobin.
Compared with the control group, the patients in the ERAS group had a significantly shorter time to first intake of clear liquid; first ambulation; first defecation; first fluid, semi-liquid, and general diet; and drain removal, and postoperative hospital stay (all P < 0.05). Additionally, fewer drains were placed in the ERAS group. There were no significant differences in pain scores and total complications between the two groups. Five patients (3.8%) in the ERAS group developed postoperative complications, namely four with urine leakage and one with intestinal obstruction, while 1 patient (0.7%) in the control group developed postoperative complications, namely intestinal obstruction (Table 4).
Surgical recovery parameters in patients in the ERAS and control groups.

*Values are expressed as mean ± standard deviation.**Statistical tests: chi-square test for categorical data and the Mann–Whitney U test for continuous data.
ERAS, enhanced recovery after surgery; LOS, length of stay; PCA, analgesic pump; Y, yes; N, no.
Discussion
Compared with conventional care, obvious differences in the ERAS protocol comprise preoperative nutrition, avoidance of preoperative fasting and carbohydrate loading, and early mobilization. All patients received intraoperative and postoperative restricted fluid therapy, multimodal analgesia, and body warming. We chose 10% glucose as a preoperative supplement because of its high carbohydrate and electrolyte levels and because this solution is easily absorbed. Regarding drug selection, opioid drugs are now commonly used in clinical practice, but they have serious side effects, such as unfavorable effects on the recovery of gastrointestinal function. In our study, multimodal analgesia in ERAS included NSAIDs, especially selective NSAIDs. The combination of NSAIDs and nerve blockers, preemptive and preventive analgesia, and preventive use of the antiemetics, metoclopramide and serotonin (5-HT3)-receptor antagonists, improved the patients’ quality of life during recovery. Moreover, patients receiving ERAS performed more postoperative activities, which could promote earlier ambulation. Encouraging exercise and drinking water early might also prevent thrombosis.
Patients in the ERAS group had food and water earlier to absorb nutrients and restore bodily functions; therefore, the POD 1 Hb and Alb concentrations of these patients were significantly higher than those in the control group after surgery. The ERAS group had more drainage on POD 2 compared with the control group, which may be related to the early postoperative activities. Changing body positions encourages drainage; the control group patients did not move, which was not conducive to drainage.
Administering excessive fluid causes intestinal edema, coagulation dysfunction, impaired wound healing, increased interstitial lung water, hypervolemia, and cardiopulmonary complications, which can all negatively influence recovery. 36 Restricting intraoperative and postoperative fluid infusion volumes not only eases the patient’s pain but also accelerates recovery. 37 There were significant differences between the groups in fluid intake within 24 hours, within 24 to 48 hours, and after 48 hours after surgery, mainly because patients in the ERAS group received fluid-restricted therapy.
Previous studies have demonstrated that early oral intake can stimulate the gastrointestinal tract to promote bowel movement.38–41 Chewing gum postoperatively leads to a clinically significant reduction in time to passage of first flatus and time to first bowel movement. 42 In this study, early oral intake and gum chewing were encouraged in the ERAS group, and these patients had a significantly shorter time to first intake of clear liquid and food and first defecation. These findings were similar to those in previous studies indicating a statistically significant shorter time to defecation and oral intake with ERAS.43–46
Recovery of intestinal function is vital in postoperative recovery. The ERAS protocol recommends omitting preoperative bowel preparation and performing preoperative carbohydrate loading and restricted fluid therapy. In our study, considering the risk of intestinal fistula, we performed bowel preparation for all patients. However, we performed preoperative carbohydrate loading and restricted fluid therapy in the ERAS group. Our results indicated that these interventions might have reduced the incidence of intestinal edema after surgery, and the recovery of intestinal peristalsis was also faster. As a result, the mean postoperative stay was 4.5 days in the ERAS group versus 5.0 days in the conventional group. Seven previous studies involving 784 participants reported hospital length of stay, which was statistically significantly shorter in the ERAS group compared with the control group. 14 ,42–47
Patients in the ERAS group had a significantly shorter time to drain removal, and fewer drains were placed. Four studies involving 457 participants reported the time to drain removal and indicated a shorter drain removal time. 14 , 43 , 44 , 46
We identified several reasons for the higher surgical complication rate in the ERAS group in this study. More activity was invariably accompanied by urine leakage, which was related to frequent position changes in the ERAS group. The outcome may have differed with a longer observation time. However, because the average length of stay was only 4.5 to 5 days, some significant indicators may have been missed. We plan to monitor the patients’ long-term quality of life to comprehensively evaluate the effect of ERAS.
Limitations
This was a single-center study, and the patients were not ethnically diverse. Once ERAS is adopted in other countries or regions, multicenter studies will be possible. Another limitation is the lack of reports of ERAS in robotic-assisted surgery. We hope that more randomized controlled trials will be performed to provide a scientific basis for summarizing the ERAS program according to robotic surgery characteristics.
Conclusion
We confirmed that the application of the ERAS protocol effectively accelerated patient rehabilitation and decreased hospital length of stay in patients undergoing RALP for prostate cancer. Although the ERAS protocol has been widely implemented in Europe and the United States and has become an accepted guideline for colorectal surgery worldwide, surgeons’ acceptance of some critical ERAS protocol elements remains low. 6 , 48 The application of the ERAS protocol in China is still in the preliminary stages, and a large-scale, well-designed, multicenter randomized controlled trials should be conducted to confirm our results.
Footnotes
Acknowledgments
We thank all participants who shared their valuable experiences in our study. We also thank Prof. Xu Gao for help with language editing, and Prof. Xiaoying Lu for reviewing and commenting on our paper.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (NSFC‐81903182) and the Shanghai Municipal Health Committee Project (201740275).
Author contributions
Study design: Jie Cao and Yan Wang; data collection: Jie Gu and Xianjuan Guo; data analysis: Xu Gao and Xiaoying Lu; and manuscript preparation: Jie Cao and Jie Gu.