
Abstract
Background
Patients with frailty are more prone to have perioperative adverse events, and enhanced recovery after surgery (ERAS) has been widely adopted to improve perioperative outcomes. The purpose of this study was to assess the impact of improved compliance with ERAS on perioperative outcomes in frail patients.
Methods
Geriatric patients (over 65 years) who underwent multi-level lumbar fusion surgery between June 2017 and June 2022 were included. The patients were divided into two groups according to their degree of compliance with the ERAS. Stepwise nearest-neighbor propensity score matching 1:1 cohorts for age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA) classfication and Charlson Comorbidity Index (CCI) was performed between groups, namely frail-compliant (FC), frail-noncompliant (FN). Further length of stay (LOS), complications and clinical efficacy were compared between groups.
Results
There were 83 pairs of well-balanced patients with comparable clinical baseline data. It was worth noting that patients in FC group has significant lower overall complications (20.5% in the FC group vs 39.8% in the FN group, P = 0.007), major complications (7.2% in the FC group vs 19.3% in the FN group, P = 0.022) and shorter LOS (11.18 ± 5.32 in the FC group vs 14.45 ± 4.68 in the FN group, P < 0.001) than patients in FN group. In addition, the initial occurrence of ambulation (2.14 ± 1.21 in FC group vs 3.18 ± 1.73 in FN group, P = 0.012) and bowel movement (3.68 ± 1.24 in FC group vs 4.17 ± 1.32 in FN group, P = 0.031) were earlier for patients in FC group than patients in FN group. With regard to clinical efficacy, there were no significant difference between FC and FN group in terms of patients who meet minimal clinical important difference (MCID) for Oswestry Disability Index (ODI) at postoperative day (POD) 30, Visual Analog Scale (VAS) for back at POD 30-90 and VAS for legs at POD 30, 90, and 180 follow-up intervals. However, there were significant more patients meeting MCID for ODI at POD 90 and180, and VAS for back at POD 180 between FC and FN group.
Conclusions
In this retrospective cohort study, we found that frail patients with higher ERAS adherence group had a lower incidence of overall complication, mjor complications, and a shorter LOS than their lower ERAS adherence counterparts. In addition, frail patients with higher ERAS adherence had earlier ambulatioin and bowel movement. More importantly, we found there were significant more patients meeting MCID for ODI at POD 90 and180, and VAS for back at POD 180 in higher ERAS adherence than their lower counterparts.
Introduction
Frailty is a complex age-related clinical condition characterised by a decline in physiological capacity across several organ systems, with a resultant increased susceptibility to stressors.1,2 The rapid expansion of the ageing population has brought a concomitant rise in the number of older adults with frailty and degenerative spinal deseases. 3 Unfortunately, older people with frailty have an increased likelihood of unmet care needs, falls, fractures, hospitalization, lower quality of life and iatrogenic complications after spine surgey, 1 especially multi-level lumbar fusion surgery. 4 Therefore, effective strategies that target the management of frailty in this population will probably improve clinical outcomes.
Enhanced recovery after surgery (ERAS) is an evidence-based, multidisciplinary perioperative approach adopted to decrease postoperative adverse events by mitigating stress response in patients following surgical intervention.5-7 Previous study has demonstrated significant improvement in length of stay (LOS) and recovery of physiological function in frail patients undergoing multi-level lumbar fusion surgery.8,9 However, we found there were still considerable frail patients who did not recovery as expected in clinical practice and follow-up when the iatrogenic cause were excluded. ERAS program usually consist of a bundle of different interventions. However, there is ongoing controversy whether all recommended interventions equally improve patient outcomes after surgery. 10 Recent published multicenter and prospective cohort studies indicate that the resultant reduction in postoperative complications and hospital LOS after the implementation ERAS most probably relying on the aggregation of marginal outcome gains by every single intervention. 11 An increase in ERAS adherence appears to be associated with a decrease in postoperative complications. 12
Previous studies has proved the clinical efficacy of ERAS protocol in lumbar fusion surgery, however, there is no sufficient data pool have evaluated the increasing ERAS adherence on clinical outcomes in frail patients following multi-level lumbar fusion surgery.8,9 Therefore, the purpose of this study were to evaluate the impact of ERAS adherence on the return of physiological function, hospital LOS, perioperative complications and clinical efficacy within one year in frail patients undergoing multi-level lumbar fusion surgery.
Methods and materials
Subjects
A retrospective analysis of geriatric patients (over 65 years) who underwent multi-level lumbar fusion and instrumentation, defined as fusion segments great than or equal to 3 between June 2017 and June 2022 were performed. All included patients were treated with posterior lumbar interbody fusion (PLIF), transforaminal lumbar interbody fusion (TLIF) or combined. This study was conducted after approval from the institutional review board (IRB#2021023). Informed consent was waived due to the nature of study design. Inclusion criteria were as following: (1) geriatric patients aged over 65 years; (2) undergoing multi-level lumbar fusion surgery for degenerative discogenic conditions and lumbar spondylolisthesis; (3) explicit frail status, which was identified using Fried phenotype score with score >2 was defined as frailty and (4) with a minimum follow-up of 6 months. Patients who were exposed to history of spinal surgery; concomitant cervical surgery or thoracic spine surgery and lack of clinical data were excluded.
ERAS Interventions
ERAS program is an patient-specific perioperative management approach, and a tailor-made management rigimen should be adopted for patients profiles in the scenario of ERAS principle. As described previously, 13 our ERAS protocol consists of preoperative, intraoperative and postoperative interventions. Perioperative measures were (1) perioperative education and counseling: informing patients the ERAS pathway to ensure them learn and understand it; (2) nutritional assessment: involving evaluating the nutritional status of the patients and providing with necessary nutrition support under the guidance of expertised nutritionist; (3) cessation of smoking and alcohol: two weeks before surgery; (4) no prolong fasting: eating is permitted up to 6 hours prior to surgery, while consumption of carbohydrate drink allowed up to 2 hours before the procedure; (5) antibiotic prophylaxis: within half an hour of incision. Intraoperative interventions were (1) tranexamic acid: within half an hour of incision or applying to the incision surface before closing the incision; (2) maintenance of normothermia: keep temperature at 36-37°C; (3) local infiltration analgesia: 10 mL ropivacaine and 10 mL lidocaine; (4) standard anesthetic protocol: TIVA-based anesthetic technique with propofol, lidocaine, ketamine, ketorolac, antiemetics and with up to 0.5% MAC inhaled anesthetics. Postoperative interventions were (1) early oral feeding: light hospital diet and oral feeding after recovery from anesthesia; (2) early ambulation: early ambulation is encouraged within the first 48 h postoperatively; (3) early removal of bladder catheter: the removal of the bladder catheter is recommended after 24 hours, in accordance with best practice guidelines; (4) multimodal analgesia: the multimodal analgesia regimen is based on the visual analogue score (VAS), with nonsteroidal anti-inflammatory drugs prescribed for VAS scores of 1 to 3, weak opioids for scores of 4 to 6, and opioids for scores greater than 7. Additionally, patient-controlled analgesic pumps were utilized.
Adherence with ERAS
Compliance with the ERAS variables was measured for each protocol of the program, and overall compliance was calculated as the percentage of protocols in the 13-element ERAS program used in the study that were fulfilled. Good compliance (>75%) was defined as compliance with any 10 or more of the 13 ERAS protocols by each patient. 14 The patients were divided into two groups according to their degree of compliance with the ERAS interventions. The frail patients were dichotomized frail-compliant (FC) group and frail-noncompliant (FN) group according to the compliance threshold.
Variables
Patient-specific and procedure-specific variables were extracted from medical records. Patients-specific perioperative data including age, gender, body mass index (BMI), smoking, drinking and Charlson Comorbidity Index (CCI), which is a validated quantitatives assessment of patient’s comorbidity burden. Procedure-specific variables including operation time, intraoperative blood loss, postoperative length of stay (LOS), fusion segments and 30-day readmission rate. Postoperative complications were reported within 30-day and classified based on comprehensive complication index, 15 calculated and weighted based on the Clavien-Dindo classification, 16 was used to summarize all postoperative complications and their severity. Included complications were wound infection, urinary tract infection, sepsis, delirium, deep vein thrombosis, urinary retention, cerebrovascular and neurological complication. Major complications were determined if comprehensive complication index scores were >20.9, equivalent to the single score of Clavien-Dindo classification II. The initial occurrences of ambulation and bowel movement were also recorded. The Visual Analog Scale (VAS) for the back and legs, as well as the Oswestry Disability Index (ODI) score, were assessed preoperatively and at one-, three-, and six-month follow-up intervals. Clinical efficacy was evaluated between groups according to minimal clinically important difference (MCID) with cut-off for ODI were 12.8 points, 1.2 points for back pain and 1.6 points for leg pain. 17
Statistical Analysis
Shapiro-Wilk test was used to test normality. Parametric data with a normal distribution was summarized as the mean and standard deviation (mean ± SD); if not, the median and interquartile range were used. Categorical variables were expressed as frequencies and proportions. Stepwise nearest-neighbor propensity score matching 1:1 cohorts for age, gender, BMI, ASA and CCI was performed between groups to keep preoperative comparable clinical characteristic. Match tolerance was set at 0.02. After propensity score matching, continuous variables with a normal distribution were analyzed using pared-samples t test, if not, Wilcoxon rank sum test was performed. Categorical variables were analyzed using McNemar test. The linear fitting was performed to describe the relationship between ERAS adherence and LOS. Adjusted R2 was used to describe goodness of fit. In addition, to calculate sample size for emphasized the impact of this study, the test level α was set as 0.05, the allowable error δ was set as 0.1, and the sensitivity was set as 0.8. According to the formula, the sample size of each group is 62. All statistical analyses were performed using SPSS software version 25.0 (SPSS, Inc, Armonk, NY, USA), and P-values <0.05 were considered statistically significant.
Results
Demographics
Results of Propensity Score Matching Between Groups.

SD: standard deviation; BMI: body mass index; ASA: American Society of Anesthesiologists; PLIF: posterior lumbar interbody fusion; TLIF: transforaminal lumbar interbody fusion CCI: Charlson comorbidity index; IQR: interquartile range; EBL: estimated blood loss.
Compared with pared-samples t test.
Compared with the McNemar test.
Compared with Wilcoxon rank sum test.
Outcome Data
A total of 50 patients developed postoperative complications, resulting in a complication rate of 26.9%, and 22 patients developed complications graded as major complications based on comprehensive complication index. There were significantly difference in overall complicatioins (20.5% in the FC group vs 39.8% in the FN group, P = 0.007) and major complications (7.2% in the FC group vs 19.3% in the FN group, P = 0.022) among groups. The number of patients with overall complications was 33 in FN group, while the lowest was 17 in FC group. In frail patients, the overall complication was significantly lower in patients with higher adherence with ERAS than their lower adherence counterparts. Collectively, patients with higher adherence with ERAS had a significantly shorter hospital LOS than their lower adherence counterparts (11.18 ± 5.32 in the FC group vs 14.45 ± 4.68 in the FN group, P < 0.001). Furthermore, the linear fitting results in frail patients indicated that with the increase in ERAS adherence, the hospital LOS was gradually reduced (adjusted R2 = 0.292) (Figure 1). There were no significant differences were found for 30-day readmission (9.6% in the FC group vs 8.4% in the FN group, P = 0.787) and 30-day reoperation rate (1.2% in the FC group vs 1.2% in the FN group, P = 1) between groups. The detailed information was showed in Table 2. The linear fitting in frial patients indicate that with the increase in ERAS adherence, the hospital LOS was gradually reduced. The Perioperative Outcomes in Postoperative 30 days Between Groups. LOS: length of stay. acompared with the McNemar test. bcompared with pared-samples t test.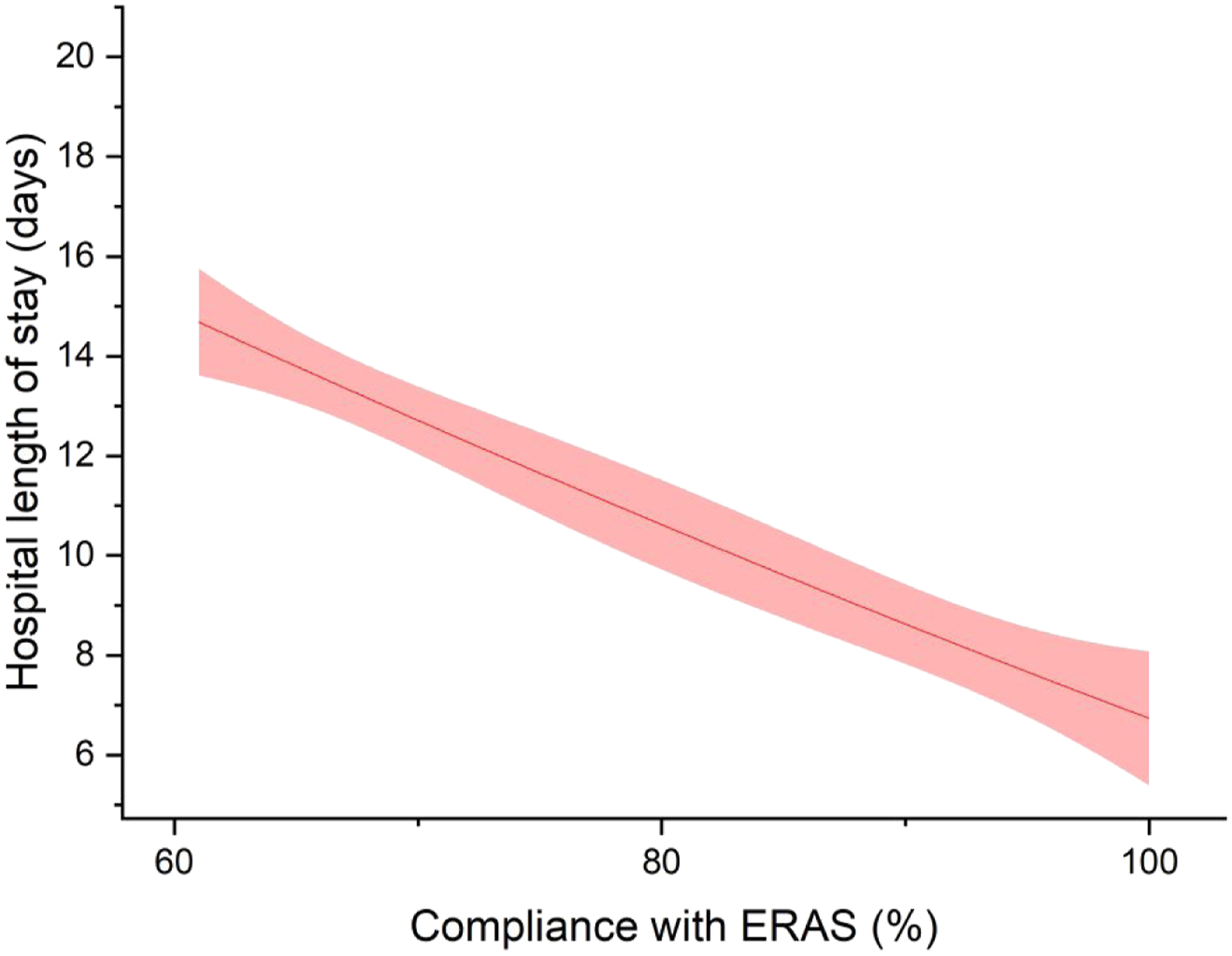

Rehabilitation
The initial occurrence of ambulation were 2.14 ± 1.21 in FC group, 3.18 ± 1.73 in FN group (P = 0.012), respectively (Figure 2). Patients with higher adherence had significantly earlier ambulation time than their lower adherence counterparts. Analogously, the bowel movement time were 3.68 ± 1.24 in FC group and 4.17 ± 1.32 in FN group (P = 0.031), respectively (Figure 3). Patients with higher adherence had significantly earlier bowel movement time than their lower adherence counterparts. The difference of initial occurrence of ambulation between groups. The difference of initial occurrence of bowel movement between groups.

Clinical Efficacy
The Outcomes of ODI and VAS at Preoperative and Postoperative 30, 90 as Well as 180-Day Follow-Up Between Groups.

ODI: Oswestry disability index; VAS: visual analogue scale; POD: postoperative day.
aCompared with pared-samples t test.
Clinical Efficacy Described as Recovery Rate for ODI and VAS According to Respective MCID During Follow-Up.
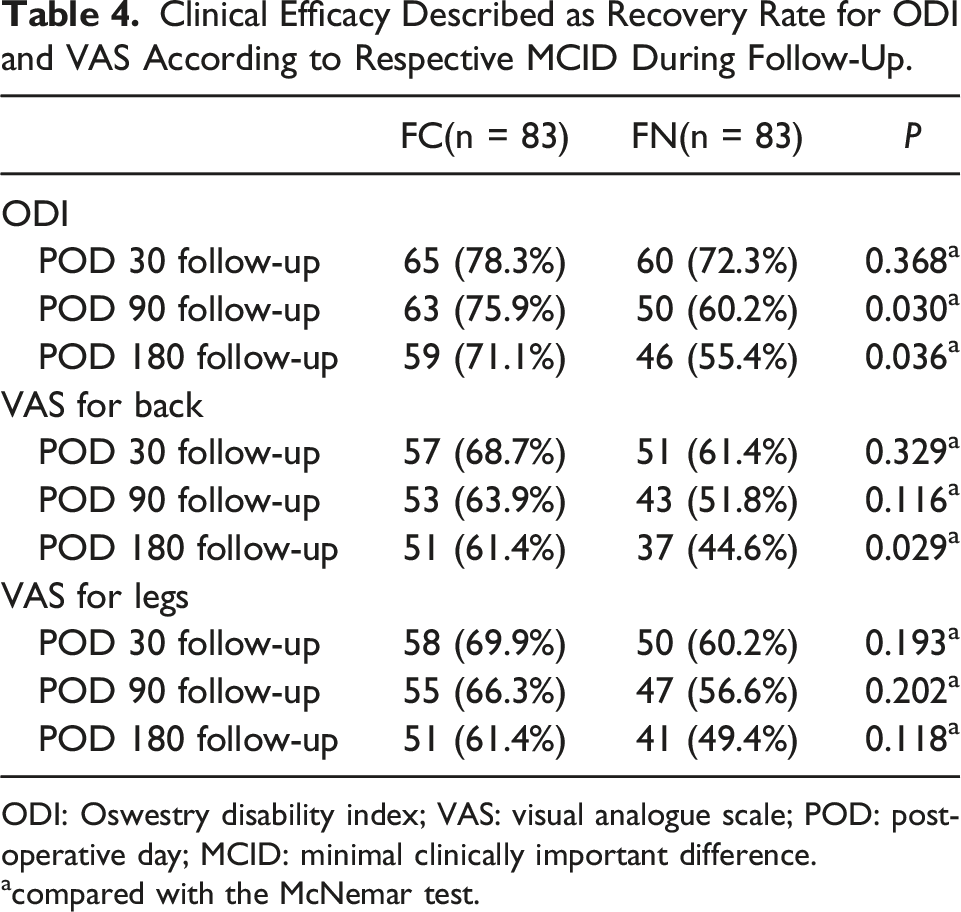
ODI: Oswestry disability index; VAS: visual analogue scale; POD: postoperative day; MCID: minimal clinically important difference.
acompared with the McNemar test.
Discussion
In this study, we found that frail patients with higher ERAS adherence group had a lower incidence of overall complication, major complications, and a shorter LOS than their lower ERAS adherence counterparts. In addition, frail patients with higher ERAS adherence had earlier ambulatioin and bowel movement. More importantly, we found there were significant more patients meeting MCID for ODI at POD 90 and180, and VAS for back at POD 180 in higher ERAS adherence than their lower counterparts.
Identification of the risk of postoperative adverse events may be challenging in geriatric patients due to the heterogeneous physical and comorbidity status. Frailty is a complex age-related clinical condition characterised by a decline in physiological capacity across several organ systems, with a resultant increased susceptibility to stressors. Once frailty is established and progresses in its natural course, other geriatric syndromes are more likely to emerge, including falls, incontinence, rapid functional decline, pressure ulcers, mild cognitive impairment, and delirium. 1 In recent years, numerous literatures indicate that frailty may serve as a strong predictor for postoperative complications.18-20 Frail patients are usually accompanied by the presence of malnutrition, further increasing the risk of surgical site infection.21,22 In addition, frail patients are more likely subjected to longer LOS and higher medical expenditure as well as higher risk of postoperative complications. 23 In a retrospective cohort study, Ton et al 24 uncovered that frailty was associated with higher adds of all perioperative complications, LOS and all-payer costs in geriatric patients and frail patients had significantly higher rates of 90 and 180-day readmission and higher rates of wound disruption at 90-days. 24 Similar results was described by Agarwal et al. they revealed frail patients (measured by Risk Analysis Index) were associated with increased risk of readmission and 90-day and 1-year mortality following spine surgery. 3 Therefore, effective strategies that target the prevention and management of frailty in an ageing population will probably reduce the condition’s burden at the level of the individual.
Given to the characteristic of the definintion, frailty means a decline in comprehensive physiological reserve function. Therefore, taking measures to enhance physiological reserve in anticipation of the predictable detrimental effects of surgery and facilitate postoperative recovery of functional capacity is thought as an alternative interventions in frail patients. However, in a randomized clinical trial, Carli et al. compared the effect of multimodal prehabilitation (involving exercise, nutritional, and psychological interventions) vs postoperative rehabilitation on 30-day postoperative complications for frail patients undergoing resection of colorectal cancer. 2 Surprisingly, the researchers found four weeks of preoperative multimodal prehabilitation did not affect postoperative complications. Such results can interpreted as the prehabilitation program lasting 4 to 5 weeks may not be sufficient to increase physiological reserve preoperatively and reduce postoperative complications. Therefore, alternative strategies should be considered to optimize treatment of frail patients preoperatively. Recent publication elicits that multidimensional interventions conducted by a multidisciplinary specialist team in geriatric settings are likely to be effective in the care of hospitalized frail elderly.8,25 ERAS is an evidence-based, multidisciplinary perioperative approach adopted to decrease postoperative adverse events by mitigating stress response in patients following surgical intervention. Emerging data underscore the crucial role of ERAS in improving perioperative outcomes in frail patients. 9 In a observational retrospective cohort study, Porche et al. found ERAS significantly improves return of physiologic function and LOS in frail patients after 1-2 level transforaminal lumbar interbody fusion. 9 Similarily, previous publication of our department suggested that ERAS significantly improves perioperative outcomes in geriatric patients with frailty undergoing multi-level lumbar fusion surgery. 13 In addition, recent investgitations have focused on establishing the role of ERAS adherence in optimizing perioperative outcomes and the positive effect of ERAS adherence is supported by an established correlation between improved compliance with ERAS and decreased perioperative adverse events in other field of surgery.14,26,27 Therefore, increasing the ERAS adherence may serve as an novel approach for improving the perioperative outcomes in frail patinets undergoing multi-level lumbar fusion surgery for degenerative conditions.
We found patients with higher ERAS adherence had significantly lower overall complications and shorter LOS than their lower ERAS adherence counterparts. Accordingly, the linear fitting results in frail patients confirmed the impact of increasing compliance with ERAS on the decreased LOS. What’s more, patients in FC group did not exhibited suboptimized functional status and postoperative residual pain, defined as recovery rate for ODI and VAS for back as well as legs according to meeting the minimum threshold for MCID during POD 30-180-follow-up. In general, our results corroborated the importance of improved compliance with ERAS in improving perioperative outcomes in frail patients. Early ambulation is an important cornerstone for the successful implementation of ERAS. In our study, patients with higher compliance with ERAS had significantly earlier ambulation than their lower ERAS adherence counterparts in frail patients. The results further confirmed the crucial importance of improved compliance with ERAS in frail patients.
The primary strength of the present study is that we provide practical evidence for improving clinical outcomes in frail patients undergoing multi-level lumbar fusion surgery for degenerative conditions. Our study was not without limitations. First, we cannot rule out that considerable bias was introduced by the observational and retrospective character of this study. Therefore, propensity score matching was used to keep comparable baseline demographic data between groups as much as possible. Additionally, frail patients generally have lower compliance with ERAS than those without frailty, which makes it difficult to determine the threshold for higher compliance, for a higher threshold leads to insufficient number of patients in FC group in the scenario of propensity score matching. Last, because of the nonrandomized nature of this study, despite the correlation found in our study, this does not imply causality.
Conclusion
In this retrospective cohort study, we found that frail patients with higher ERAS adherence group had a lower incidence of overall complication, major complications, and a shorter LOS than their lower ERAS adherence counterparts. In addition, frail patients with higher ERAS adherence had earlier ambulatioin and bowel movement. More importantly, we found there were significant more patients meeting MCID for ODI at POD 90 and 180, and VAS for back at POD 180 in higher ERAS adherence than their lower counterparts.
Footnotes
Acknowledgements
We thank the Department of Orthopedics, The Third Hospital of Hebei Medical University staff and all the patients who participated in the study.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Xiaoying Zhang, Xuewei Dong and Huili Luo. The first draft of the manuscript was written by Yanli Song and Shengmin Chen. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hebei Provincial Health Commission research fund project [No. 20190656]. The funders played no role in the design of this study, the collection, analysis and interpretation of data or preparation of the manuscript.
Ethical statement
Data Availability Statement
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.