
Abstract
Introduction
The aim of this retrospective study was to assess the clinical outcomes of cemented or uncemented total hip arthroplasty (CTHA or UTHA) following prior failed proximal femoral nail antirotation (PFNA) fixation in patients with intertrochanteric femur fractures (IFFs).
Materials and methods
Data from 244 patients with IFFs who experienced a conversion of PFNA to CTHA (n = 120) or to UTHA (n = 124) due to screw cut-out, mal/nonunion, or osteonecrosis during 2008-2018 were retrospectively analyzed. Follow-up occurred 1, 3, 6, and 12 months postoperatively and yearly thereafter. The primary outcome was the incidence of orthopedic complications; the secondary outcome was the Harris hip score (HHS).
Results
The median follow-up was 60 months (range, 50-67 months). The incidences of orthopedic complications were 10% in the PFNA to CTHA group and 19.3% in the PFNA to UTHA group (P = .040). Significant differences were also observed regarding the incidence of prosthesis revision (1.7% for PFNA to CTHA vs 7.2% for PFNA to UTHA, P = .036). From the three years after conversion surgery to the final follow-up, significant differences were detected in HHS between groups (each P < .05). At the final follow-up, a statistically significant difference was detected in the HHS (79.54±18.85 for PFNA to CTHA vs. 75.26±18.27 for PFNA to UTHA, P = .014).
Conclusion
The results of the study may demonstrate a significant statistical advantage with respect to the orthopedic complication rate and HHS in favor of CTHA compared to UTHA in patients with failed PFNA.
Introduction
Therapeutic advances in proximal femoral nail antirotation (PFNA) have extensively improved the outcomes for an increasing number of patients with a clinical diagnosis of intertrochanteric femur fractures (IFFs), a subtype of proximal femoral fractures, which was previously associated with poor prognoses.1-3 The number of IFFs treated with PFNA during the past decade has increased dramatically and will substantially increase, not only as a consequence of an aging population but also owing to its increasing use in young patients.4,5 Hence, the number of failed PFNAs that require revision procedures may also increase accordingly. 2 Regrettably, the available options for revising a failed PFNA are limited. 2 When a failed PFNA intervention is indicated, the treatment strategies remain challenging and controversial. 1 Conversion from PFNA to cemented or uncemented total hip arthroplasty (CTHA or UTHA) tends to be an approved method.6,7 However, the choice of implant material (CTHA or UTHA) is frequently unclear.8,9 Most of those reports have been from academic centers, with a limited number of cases.10,11 The decision as to which type of implant (CTHA or UTHA) is optimal in treating patients with a failed PFNA may lead to a significant difference in the application of each intervention internationally.12,13 However, most of those reports have been from a highly specialized medical institution, with a limited number of cases. 14
A comparative study 15 assessing the clinical outcomes of the conversion to CTHA or UTHA in 198 elderly patients with failed PFNAs showed that CTHA had a lower rate of orthopedic complications than UTHA (19.0% vs. 40.8%, P = .001). In the comparative study patient comorbidities and severity of illness were not mentioned, although comorbidities have been proven to be associated with an increased risk of periprosthetic infection in patients experiencing arthroplasties.16,17 Recently, a retrospective study 18 of 120 patients aged 30-60 years with prior failed primary fixations of proximal femoral fractures undergoing CTHA conversion showed that the rate of orthopedic complications was 18.3%. However, in the retrospective study, the leading etiologies of failure of a secondary CTHA conversion are unclear. Furthermore, the variety of implant versions and the lack of a control group may have some influence on their results.
To date, mid-term outcomes regarding the superiority of PFNA to CTHA over PFNA to UTHA remain limited. In addition, with the increasing use of the PFNA device in clinical practice, it may be particularly important to conduct mid-term evaluations of these two conversions. We therefore performed this retrospective study to compare the clinical and radiographic outcomes of patients with failed PFNA who experienced a conversion to CTHA or UTHA in the Asian population.
Methods
Study Population
The data covering the period of July 1, 2008, to July 31, 2018, were obtained retrospectively from our medical center according to ICD-10 S72.101. The registry records of 292 consecutive patients who had undergone a conversion from PFNA to CTHA or to UTHA during the study period were retrospectively analyzed. These patient details were deidentified according to our protocol. The conversion procedure was executed as stated by the manufacturers’ instructions at three medical institutions by 6 surgeons who were all trained in arthroplasty. Comorbidities related to patients were evaluated with the Charlson comorbidity index (CCI). The inclusion criteria were as follows: active elderly patients aged ≥60 years old; patients with a prior IFF (Type AO/OTA 31. A) treated with PFNA (a solid titanium nail, 200-240 mm in length, 11-16 mm in diameter, 125° or 130° in collodiaphyseal angle, Synthes, USA), followed by CTHA (an Exeter Universal stem and a cemented all-polyethylene cup [Stryker, Mahwah, NJ]) or UTHA (a Taperloc stem [Biomet, Warsaw, Ind] and an uncemented polyethylene cup [HCC, Houston, Tex]); and patients with failed fixation due to screw cut-out, mal/nonunion, or osteonecrosis. The key exclusion criteria included inadequate baseline data, hip dysplasia, active metabolic bone diseases, dyskinesia, lower extremity sensory disorders, metastatic diseases, severe medical diseases, dependence on alcohol or drug abuse, inability to follow instructions, vascular cognitive impairment, and an American Society of Anesthesiologists (ASA) score of IV or V. The ICD -10- Chinese Modification codes were applied to identify the relevant conditions mentioned in the exclusion criteria.
Surgical Procedures
The previous PFNA device was removed using the original incision. CTHAs or UTHAs were implanted using the direct lateral approach. After reaming the femur, third-generation cementing techniques were used. After retrograde pressurization of the cement, the stem was inserted slowly at a uniform speed. The integrity of the greater or lesser trochanter was reconstructed using femoral neck bone masses and fixed with steel cables or steel cables plus metal mesh. The length of the cemented stem was approximately 2 cm greater than the length of the main nail, preventing possible adverse events (ie, malunion, nonunion, periprosthetic femoral fracture) related to stress risers. Small bone fragments from the femoral neck and head were used to fill the proximal and lateral femoral screw holes after PFNA removal. Some of the excess cement was used to fill small defects in the greater or lesser trochanter. A cemented cup was inserted according to the manufacturer’s instructions. Acetabular defects were reconstructed with metal mesh and/or impaction autografts. Segmental posterosuperior defects greater than 20 mm were treated using metal mesh. The trimmed metal mesh was fixed to the iliac bone using 3-5 cm bicortical screws. Small medial wall defects or segmental defects less than 20 mm were treated using impaction autografts. After reconstructing the acetabular defects, we reserved a circumferential 2-mm cement mantle around the definitive cup. After testing the model cups, we used a 2-mm drill bit to drill through the sclerosed bone until blood oozed out to optimize vascularization and facilitate the incorporation of the graft into the cement. Adrenaline-soaked gauze was used to tamp the acetabulum to reduce acetabulum bleeding. Next, antibiotic-loaded cement (1 g cefazolin/50 g cement) was pressurized and the definitive cup was positioned with 40-45° of inclination and 20° of anteversion. The technical details of UTHA and CTHA were the same, except for the third-generation cementing techniques.
Antibiotics (ie Cefazolin, cefalexin, and cefradine) were routinely administered intraoperatively until three days after surgery. Postoperatively, all patients were treated with low-molecular-weight heparin sodium or rivaroxaban for 4 weeks to prevent venous thrombosis. Patients were mobilized three days after surgery. In the case of extended reconstructions, touch weight bearing on the operated side with a walker was allowed for 6-10 weeks. After that, progressive weight bearing was encouraged.
Clinical and Radiographic Analysis
The clinical and radiographic outcomes were retrospectively reviewed by two authors (GL and TH). The primary outcome measure was the rate of orthopedic complications, including prosthesis revision, loosening, periprosthetic fracture, dislocation, periprosthetic infection, intolerable hip pain, lower limb shortening, and thrombotic events. Radiographic analysis consisted of anteroposterior views of the hip and pelvis and a true lateral view of the hip. The secondary outcome measure was the HHS (range, 0-100). Follow-up occurred at 1, 3, 6, and 12 months postoperatively and yearly thereafter. Patients included in the present study were followed up mainly through outpatient follow-up and telephone interviews.
Definition of Variables
The follow-up time was defined as the time interval between the date of PFNA to CTHA or PFNA to UTHA and the date of the final follow-up. The criteria used to define loosening of the acetabular component included >2 mm of radiolucent line, >3 mm of migration, and a change in the amount of lateral tilt of >5°.19,20 Radiographic loosening of the femoral component was diagnosed when there were signs of subsidence of >3 mm, continuous radiolucencies or fractures at the bone-cement or shaft-bone interface, or large defects around the stem. 21 Periprosthetic infection was diagnosed according to the Musculoskeletal Infection Society Criteria. 22 Osteolysis was evaluated by the criteria of McLaughlin et al 13 Heterotopic ossification was assessed per the Brooker classification system. 23 Prosthesis revision was defined as removal of the CTHA or UTHA device for any reason. 24
Statistical Analysis
Categorical variables (ie, sex, side) were compared using the chi-square test or Fisher’s exact test. Continuous variables were compared using two-way ANOVA for normally distributed variables (ie, age, body mass index [BMI], bone mineral density [BMD], HHS, follow-up period) and the Mann-Whitney U test for nonnormally distributed variables (ie, mechanism of injury, IFFs, comorbidities, reasons for revision, time between two surgeries, ASA index, implant-related complications). The survival curve was drawn using the Kaplan–Meier method. A significant difference was defined as a one-sided P value <.05. All statistical analyses were executed using SPSS 26.0 (IBM Corp, Armonk, NY).
Results
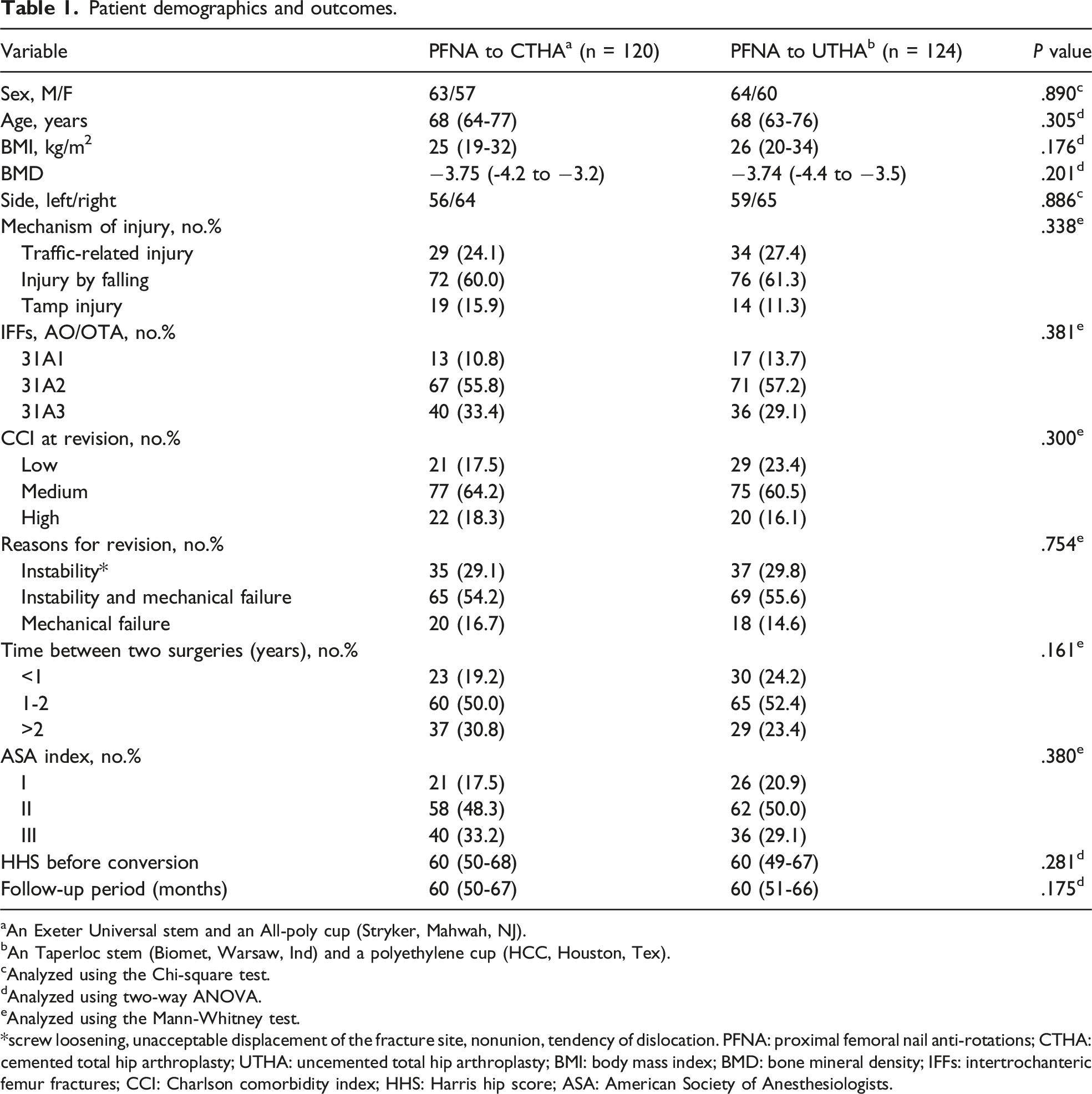
Based on our inclusion and exclusion criteria, 244 consecutive patients (244 hips) were identified from the registry (PFNA to CTHA: n = 120, mean age, 68 years [range, 64-77 years]; PFNA to UTHA: n = 124, mean age, 68 years [range, 63-76 years]), as shown in Figure 1. There were 63 male patients vs. 64 male patients (P = 890). The CCI at revision was low in 17.5%, medium in 64.2%, and high in 18.3% in the PFNA to CTHA group vs. low in 23.4%, medium in 60.5%, and high in 16.1% in the PFNA to UTHA group (P = .300). The ASA index at revision was Ⅰ in 17.5%, Ⅱ in 48.3%, and Ⅲ in 33.2% in the PFNA to CTHA group vs. Ⅰ in 20.9%, Ⅱ in 50.0%, and Ⅲ in 29.1% in the PFNA to UTHA group (P = .380). The HHS before conversion was 60 (range, 50-68) in the PFNA to CTHA group vs. 60 (range, 51-66) in the PFNA to UTHA group (P = .281). The median follow-up was 60 months (range, 50-67 months) for the PFNA to CTHA group and 60 months (51-66 months) for the PFNA to UTHA group (P = .175). The patient-specific details and preoperative data were collected and are shown in Table 1. At the end of the study, no significant differences in mortality were detected (15.0% [21/120] vs. 16.1% [20/124], P = .808). Flow diagram demonstrating methods to assess the clinical outcomes of cemented or uncemented total hip arthroplasty (CTHA or UTHA) following prior failed proximal femoral nail anti-rotations (PFNA) fixation in patients with intertrochanteric femur fractures (IFFs). Patient demographics and outcomes. aAn Exeter Universal stem and an All-poly cup (Stryker, Mahwah, NJ). bAn Taperloc stem (Biomet, Warsaw, Ind) and a polyethylene cup (HCC, Houston, Tex). cAnalyzed using the Chi-square test. dAnalyzed using two-way ANOVA. eAnalyzed using the Mann-Whitney test. *screw loosening, unacceptable displacement of the fracture site, nonunion, tendency of dislocation. PFNA: proximal femoral nail anti-rotations; CTHA: cemented total hip arthroplasty; UTHA: uncemented total hip arthroplasty; BMI: body mass index; BMD: bone mineral density; IFFs: intertrochanteric femur fractures; CCI: Charlson comorbidity index; HHS: Harris hip score; ASA: American Society of Anesthesiologists.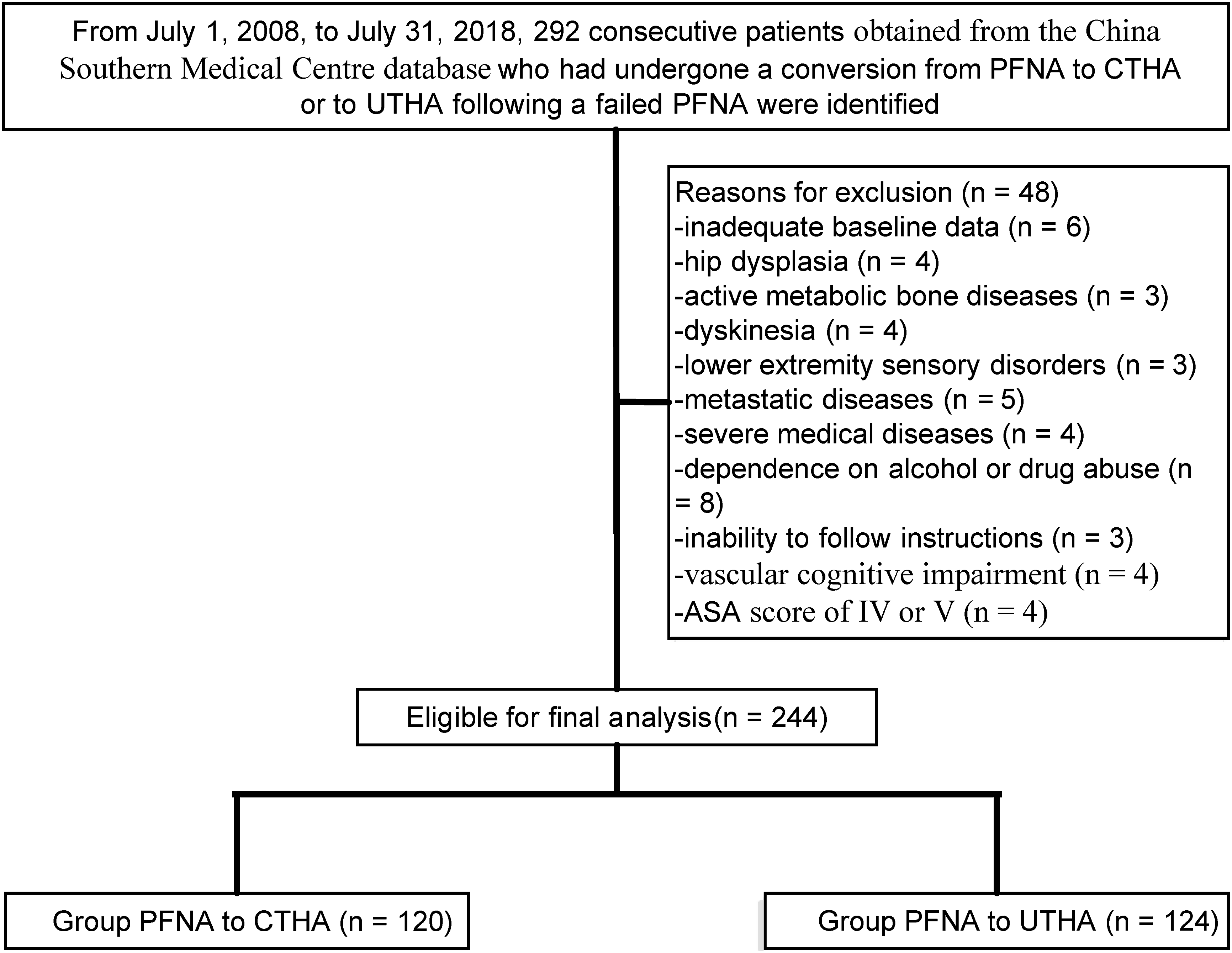
Primary Outcome
Long-term follow-up: implant-related complication rate.

*Statistically significant values.
aAn Exeter Universal stem and an All-poly cup (Stryker, Mahwah, NJ).
bAn Taperloc stem (Biomet, Warsaw, Ind) and a polyethylene cup (HCC, Houston, Tex). PFNA: proximal femoral nail anti-rotations; CTHA: cemented total hip arthroplasty; UTHA: uncemented total hip arthroplasty.
cAnalyzed using the Chi-square test.
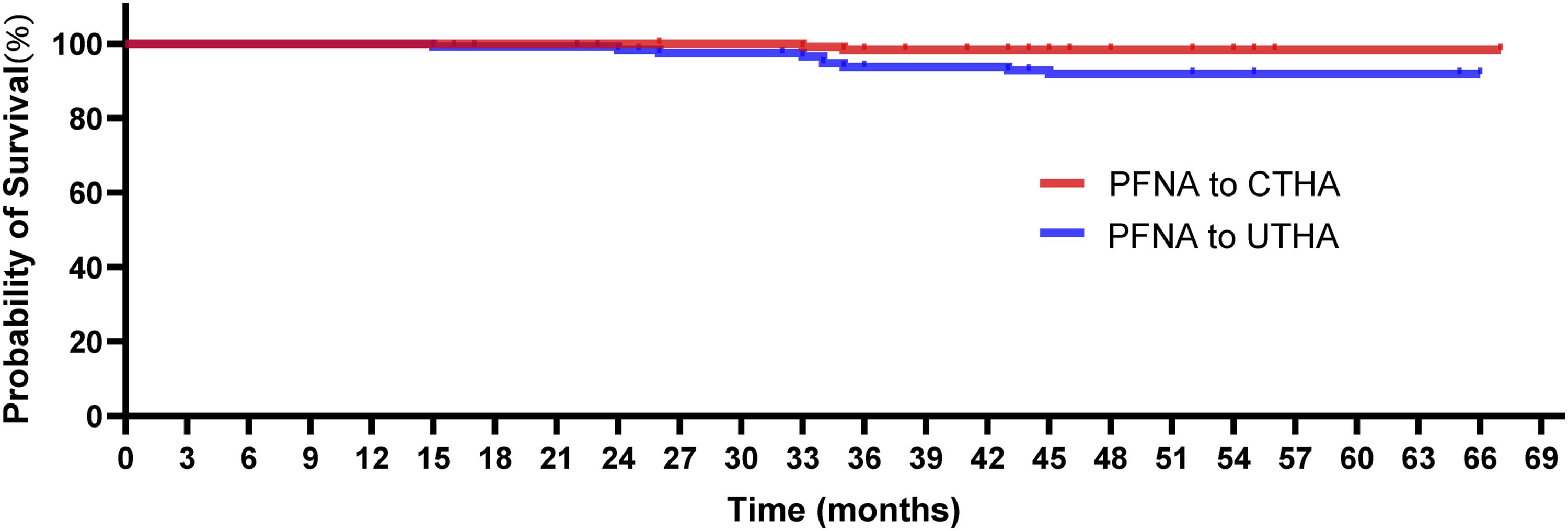
Kaplan–Meier survival curve for both groups with prosthesis revision for any reason as the endpoint.
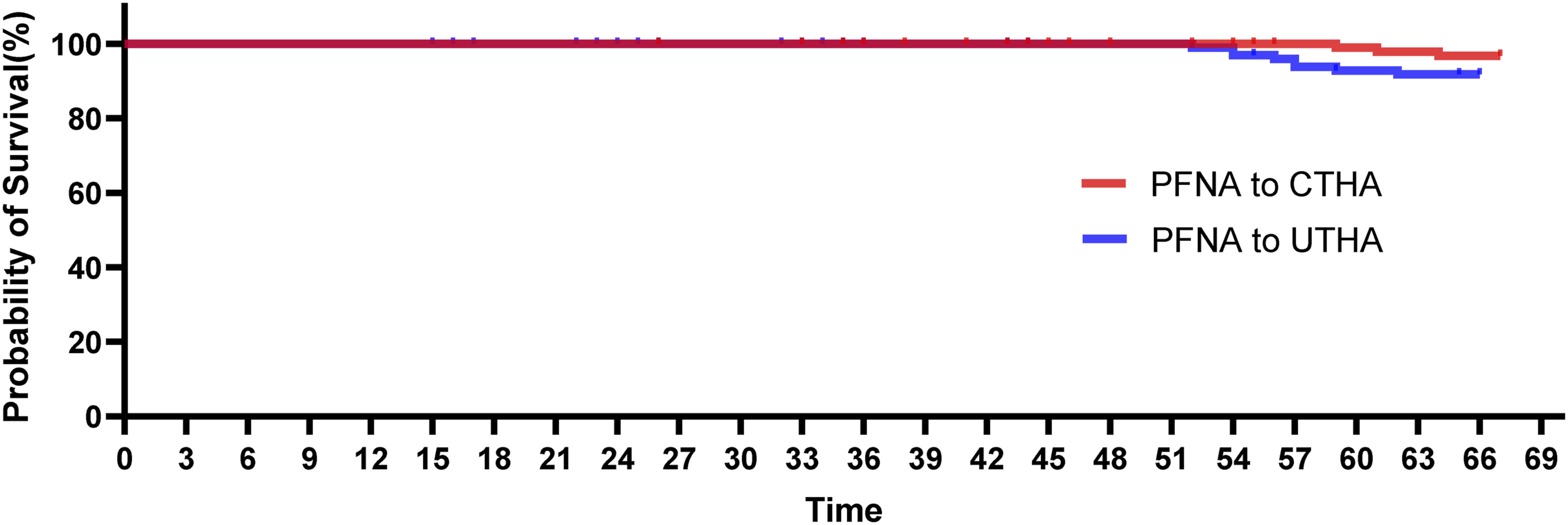
Kaplan–Meier survival curve for both groups with periprosthetic loosening as the endpoint.
Secondary Outcome
At the final follow-up, the scores were 79 (range, 61-97) for PFNA to CTHA and 75 (57-93) for PFNA to UTHA (P = .014). Figure 4 illustrates the variation trend of postoperative functional scores. From the three years after conversion surgery to the final follow-up, significant differences were detected in HHS between groups (each P < .05), and CTHA had a noteworthy functional advantage compared to UTHA in these cases. Within three years after conversion surgery, noteworthy differences regarding the HHS failed to be detected at each follow-up (each P > .05). The variation trend of postoperative functional scores.
Discussion
Mid-term outcomes regarding the superiority of PFNA to CTHA over PFNA to UTHA remain lacking. This retrospective study aimed to evaluate the clinical outcomes of single brands of CTHA or UTHA following failed PFNA fixation in IFF patients and may show a significant advantage in the clinical outcomes of CTHA over those of UTHA. There was a significant statistical advantage with respect to the orthopedic complication rate in favor of CTHA compared to UTHA. The HHS improved in the PFNA to CTHA group after the 36-month follow-up, in contrast to the PFNA to UTHA group, in which there was a significantly lower HHS after 36 months. The diverse developments in the HHS over time may suggest a better HHS in the PFNA to CTHA group at the 5-year follow-up than in the PFNA to UTHA group. Future studies should focus on long-term conversion results. While our analysis may statistically validate the difference in the HHS, it failed to validate the differences in the rate of orthopedic complications during the first 2 years, most likely owing to the short follow-up. The mid-term outcomes of CTHA or UTHA for patients with a failed PFNA are a matter of great debate. 25 However, a growing but still very limited body of literature has investigated the therapeutic role of these two endoprostheses and has suggested that the differences between CTHA and UTHA may be attributed to errors in surgical techniques or indications.26,27 No literature has provided guiding principles to reduce or avert mechanical complications. 28 Consistent with previous studies,29,30 we failed to observe conspicuous differences in the HHS at the end of the 3-year follow-up. This lack of differences could be attributed to the relatively short follow-up.
The outcomes regarding the rate of orthopedic complications were within acceptable limits. 28 Our findings are comparable to those of prior reports with at least a 2-year follow-up.7,27 Nevertheless, the quantitative comparison is problematic for interpretation since a majority of prior reports included a mixed population of proximal femoral fractures and multiethnic, younger patients, and stress shielding of the proximal femur is especially age-dependent. 3 Previous literature29,31 has demonstrated that UTHA has a higher rate of orthopedic complications than CTHA. Additionally, recent evidence favors UTHA for proximal femur fractures with a high rate of orthopedic complications. 26
Our findings are supported by previously available literature30,32 in this area that showed an increased revision rate in UTHA cases. Nevertheless, the majority of population reports that focus on this subject are based on 10-year follow-up data. Few prior studies29,33 have quantified the risk for revision in this setting. Additionally, our study sheds light on the risk for revision surgery for patients with a failed PFNA treated with UTHA. Although it has been previously recognized that this cohort has a higher 5-year revision rate than those undergoing CTHA, the true risk to a patient treated with UTHA tends to be higher than previously reported. 29 The higher rate of revision could be associated with dissimilarities in implant materials. The decision about whether to proceed with surgery is mostly based on the balance between revision risks and benefits. Previous reports34,35 were commonly restricted to specific implants or small populations, without a definite focus on the results of patients. Hence, the decision-making process for such patients failed to be fully considered and could result in an inapposite intervention.
The inherent limitations of the current study are similar to those of other retrospective analyses. First, observational reports such as our study are susceptible to absent variables and the subsequent inability to adjust for certain biases inherent to the methodology. Assessing the superiority of one device over another tends to be restrictive in nature and could be compromised by a relatively small population, improper control of confounding factors, and moderately short follow-up. The exclusion of patients who lost contact during follow-up (ie, death) may have overstated our results. Second, although antibiotics were routinely used in each patient, there were some differences in the type, dosage, and duration of antibiotics in some patients, which could introduce potentially confounding factors when considering periprosthetic infection as an endpoint.
Conclusions
The goal of the current study was to provide a possible explanation that CTHA may have a significant statistical advantage with respect to functional results and fewer orthopedic complications than UTHA in the conversion setting. Our findings could help settle ongoing debates about the decision-making process for revisions in such patients. Future multicenter trials are needed to further validate these findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was approved by the Investigational Ethics Review Board (Wuhan Third Hospital, Wuhan, China), and an exemption from informed consent was obtained from the board.