
Abstract
Objective
To retrospectively compare the mid-term outcomes of uncemented or cemented total hip arthroplasty (THA) revision for prior primary metal-on-metal (MoM) THA failure.
Methods
Data from 278 patients (278 hips) who underwent uncemented THA (UTHA) or cemented THA (CTHA) for prior primary MoM-THA failure from 2006 to 2016 were retrospectively analysed. Follow-up was performed 6 months, 1 year, 2 years, and then every 2 years after conversion. The mean follow-up time was 96 months (range, 64–128 months). The primary endpoint was the modified Harris hip score (HHS). The secondary endpoint was the major orthopaedic complication rate.
Results
The HHS showed significantly greater differences in the CTHA than UTHA group 12 months after conversion. From the 12th month after conversion to the final follow-up, CTHA yielded better functional outcomes than UTHA. There were significant differences between the UTHA and CTHA groups in the rates of re-revision (14.4% vs. 4.9%, respectively), aseptic loosening (17.3% vs. 6.8%, respectively), and periprosthetic fracture (11.5% vs. 3.9%, respectively).
Conclusion
CTHA has more advantages than UTHA in terms of improving functional outcomes and decreasing the major orthopaedic complication rate.
Introduction
Bearing surfaces provided by metal-on-metal total hip arthroplasty (MoM-THA) became increasingly prevalent, particularly in the context of the ageing population, in earlier decades.1,2 In recent years, however, the use of MoM-THA has sharply declined because of the reported low 10-year survival rate and high failure rate, which are associated with several issues including adverse reactions to metal debris (ARMDs), aseptic loosening, and infection.1,3 Failure after MoM-THA is well recognised, has various causes, and frequently requires surgical revision. 4 Failure that occurs secondary to MoM wear tends to be of particular concern among physically active individuals. 5 Although MoM bearings have fallen out of favour as a result, orthopaedists continue to struggle with this issue of revision burden. 2 Poor bone stock may be attributed to the substantial bone and soft tissue destruction caused by an ARMD, which is powerfully implicated in the pathophysiology of MoM-THA failure and contributes to the substantially high revision rate as well as the rapid time to failure. 2
This high MoM-THA-related failure rate may also contribute to the increased use of uncemented THA (UTHA) or cemented THA (CTHA). 6 A few studies5,6 have assessed complications due to conversion of MoM-THA to the use of uncemented or cemented femoral components (UTHA or CTHA). Interest in CTHA has increased during the last decade, with several studies showing higher Harris hip scores (HHSs) and fewer orthopaedic complications in CTHA than in UTHA.7,8 However, other studies have demonstrated no significant differences between the two techniques.9,10 Furthermore, there are concerns that longer-term outcomes of UTHA may not be as robust as those of CTHA in terms of reduced revision rates. 11 Additionally, highly selected patient populations are common in the published literature.2,12 Thus, the findings of these previous studies cannot be considered valid.
No definitive consensus exists on the mid-term outcomes of conversion from primary MoM-THA to UTHA or CTHA of any cause. 9 Given the lack of literature and minimal understanding of these types of conversions, we performed a retrospective study to assess the mid-term outcomes of conversion from primary MoM-THA to UTHA or CTHA.
Materials and methods
Study population
This retrospective study was approved by the Medical Ethics Committee of the Affiliated Hospital of Fujian Medical University, and the investigational review board waived the requirement for informed consent. An initial study cohort comprising 278 patients (278 hips) was identified from our joint registration database. All patients had undergone UTHA or CTHA revision because of prior primary MoM-THA failure from May 2006 to May 2016. The main reasons for revision were ARMD, aseptic loosening, infection, dislocation, and fracture. The inclusion criterion for the study was performance of a conversion procedure from primary MoM-THA (Zimmer Biomet, Warsaw, IN, USA) to UTHA or CTHA. The manufacturer details of the devices used in UTHA and CTHA are shown in Table 1. All conversion procedures were performed by three experienced orthopaedists (J.Y., J.L., and Z.C.) via a direct anterior approach as previously described. 13 The main exclusion criteria were the lack of an MoM-bearing surface at the time of conversion, inadequate clinical data, active infection, dyskinesia, bone-related diseases, an inability to follow instructions, malignant tumours, an injury severity score of ≥10, brain dysfunction of any cause within 6 months, pulmonary complications (e.g., reintubation), cardiovascular complications (e.g., cardiac arrest, myocardial infarction), renal complications (e.g., insufficiency or failure), vascular cognitive impairment, a history of alcohol and/or drug abuse, a body mass index of >40 kg/m2, and an American Society of Anesthesiologists score of IV or V.
Manufacturer details of UTHA and CTHA.

1DePuy, 2Smith & Nephew, 3Biotechni, 4Stryker, 5Waldemar LINK. UTHA, uncemented total hip arthroplasty; CTHA, cemented total hip arthroplasty.
A standard protocol was utilised to obtain clinical and radiographic data. Follow-up was performed 6 months, 1 year, 2 years, and then every 2 years after conversion. The primary endpoint was the modified HHS. The secondary endpoints were the major orthopaedic complication rates. All patients underwent conversion to UTHA or CTHA at our medical centre and were assessed individually with the modified HHS at each follow-up. Imaging data were acquired at these same time points: anteroposterior radiographs of the pelvis and anteroposterior and lateral radiographs of the hip as well as computed tomography or magnetic resonance imaging if necessary. The occurrence of major orthopaedic complications was recorded for each patient during follow-up.
Statistical analysis
Between-group differences in the baseline data and main follow-up data were compared. Follow-up was calculated in days from the date of revision/conversion to the date of death or final follow-up, whichever occurred first. Revision was defined as complete removal of the endoprosthesis. 2 Prosthesis loosening and endoprosthesis failure were judged based on prior descriptions. 4 Continuous data are presented as mean ± standard deviation. A t test was utilised to assess between-group differences if the data were consistent with assumptions regarding a normal distribution and homogeneity of variance. If not, the Wilcoxon rank-sum test was utilised. Categorical data are presented as frequency and percentage and were compared between groups using the chi-squared test or Fisher’s exact test, as appropriate. All statistical analyses were performed using SPSS version 24.0 (IBM Corp., Armonk, NY, USA). A two-sided p value of <0.05 was considered statistically significant.
Results
Based on our inclusion and exclusion criteria, 206 individuals (206 hips) undergoing conversion from primary MoM-THA to UTHA or CTHA were identified for the final analysis in the study. The UTHA comprised 104 patients with a mean age of 65.12 ±7.34 years, and the CTHA group comprised 102 patients with a mean age of 64.67 ± 8.71 years. The interval from primary MoM-THA to failure was 3.7 years (range, 1.1–5.7 years) in the UTHA group and 3.6 years (range, 1.3–6.2 years) in the CTHA group. At the time of analysis, the mean follow-up time from conversion was 96 months (range, 64–128 months) in the UTHA group and 96 months (range, 66–126 months) in the CTHA group. A study flow chart is presented in Figure 1, and the baseline data are shown in Table 2.

Study flow chart. UTHA, uncemented total hip arthroplasty; CTHA, cemented total hip arthroplasty; MoM-THA, metal-on-metal total hip arthroplasty; ISS, injury severity score; BMI, body mass index; ASA, American Society of Anesthesiologists.
Patient demographics and outcomes.
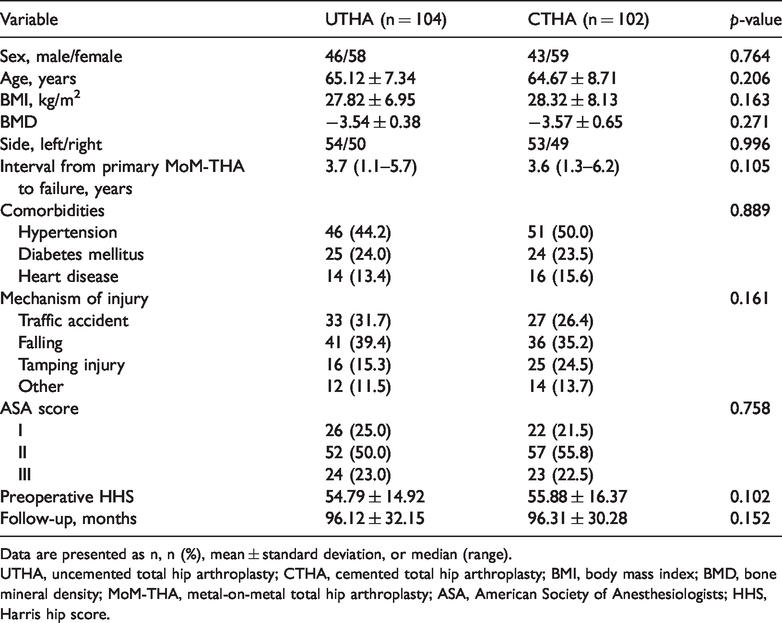
Data are presented as n, n (%), mean ± standard deviation, or median (range).
UTHA, uncemented total hip arthroplasty; CTHA, cemented total hip arthroplasty; BMI, body mass index; BMD, bone mineral density; MoM-THA, metal-on-metal total hip arthroplasty; ASA, American Society of Anesthesiologists; HHS, Harris hip score.
Primary endpoint
The mean HHSs after conversion are shown in Table 3. The mean HHSs in the UTHA and CTHA groups were 82.75 ± 5.13 and 83.12 ± 6.25 6 months after conversion, 85.56 ± 6.24 and 87.18 ± 9.73 12 months after conversion, and 78.22 ± 17.36 and 85.91 ± 15.02 at the final follow-up, respectively. The HHSs showed significantly greater differences in the CTHA than UTHA group 12 months after conversion (p = 0.026). From the 12th month after conversion to the final follow-up, CTHA yielded better functional outcomes than UTHA (all p < 0.05). Almost 76% of the patients who developed MoM-THA failure and underwent conversion to UTHA or CTHA had an acceptable HHS at the final follow-up. Differences in the HHS were not significant between the two groups 6 months after conversion.
Mid-term follow-up: functional outcomes.

Data are presented as mean ± standard deviation.
*Statistically significant values.
HHS, Harris hip score; UTHA, uncemented total hip arthroplasty; CTHA, cemented total hip arthroplasty.
Secondary endpoint
Fifty-four major orthopaedic complications occurred among the 106 patients in the UTHA group versus 27 complications among the 102 patients in the CTHA group. Of the 54 complications in the UTHA group, 12 (11.5%) involved periprosthetic fractures and 18 (17.3%) were associated with aseptic loosening. The re-revision rate was 14.4%. Of the 27 CTHA-related orthopaedic complications, 4 (3.9%) involved periprosthetic fractures and 7 (6.8%) were associated with aseptic loosening. The re-revision rate was 4.9% (Table 4). The between-group difference in the re-revision rate was significant at the last follow-up (14.4% for UTHA vs. 4.9% for CTHA, p = 0.021). The rate of re-revision attributed to aseptic loosening was 73.5% in the UTHA group and 66.5% in the CTHA group (p = 0.014).
Mid-term follow-up: prosthesis-related complications.

Data are presented as n (%).
*Statistically significant values.
UTHA, uncemented total hip arthroplasty; CTHA, cemented total hip arthroplasty.
Discussion
The current findings provide evidence that the revision of primary MoM-THA failure using CTHA results in superior mid-term clinical outcomes compared with the use of UTHA. To our knowledge, this is the largest study of the outcomes of conversion after MoM-THA failure.
Complications of MoM-THA related to ARMD can result in significant bone and soft tissue destruction as well as increased metal ion levels, especially cobalt and chromium, potentially increasing the risk of implant failure and posing a challenge for future revision.14,15 Metal ions can inhibit osteoblast gene expression, and they have a negative impact on osteoblast cell numbers and activity.15,16 This can ultimately result in bone ingrowth failure in the uncemented components utilised during conversion to UTHA after MoM-THA failure. 16
MoM-THA revision is associated with high rates of orthopaedic complications due to periprosthetic fracture, aseptic loosening, and dislocation. 2 In the 2018 National Joint Registry Annual Report, 4 the 14-year cumulative probability of revision was 22.2% for uncemented stemmed MoM-THA. Whether increases in hip stability exist following MoM-THA revision has become one of the key indicators.2,13 Hip stability following conversion to CTHA is superior to that following conversion to UTHA because of the instability of the bone and uncemented components. 17 Macroscopic damage or bone defects are often present at the time of UTHA re-revision. 18 The cause of these bone defects is associated with malpositioning and a design that is too shallow for the acetabular component, resulting in atypically elevated wear triggered by edge loading.19,20 One study showed a high rate of aseptic loosening of the femoral component after UTHA re-revision due to MoM-THA failure. 21 Failure due to aseptic loosening occurs more frequently with UTHA re-revision than with CTHA re-revision.2,7 The most appropriate re-revision intervention to decrease the high rate of aseptic loosening is a matter of ongoing debate. 2 Perhaps there is an effective solution when both the femoral and acetabular components are well ingrown.
Despite the continued advancements in prosthetic materials, the risks associated with conversion from MoM-THA to UTHA or CTHA remain a substantial concern.2,4 However, the obtainable literature 20 on the outcomes of this type of conversion is lacking and contradictory. A growing but still extremely limited body of literature describes the role of UTHA or CTHA revision in the setting of prior MoM-THA failure and has demonstrated significant differences in clinical outcomes, although all the studies are limited by small sample sizes and/or short-term follow-up periods.2,6 Undeniably, invasive revision procedures are associated with a high rate of orthopaedic complications. 4 However, we failed to detect noteworthy distinctions regarding the rates of major orthopaedic complications 12 months after conversion. Concerns have been raised regarding whether these two types of conversion have substantial differences in mid-term outcomes, including orthopaedic complication rates.22,23 In 2009, Eswaramoorthy et al. 24 described 76 patients who underwent conversion from MoM arthroplasty to UTHA. Similar to the findings observed in the current study of failed MoM-THA treatment, both aseptic loosening and periprosthetic fracture were the primary orthopaedic complications due to conversion. The authors also reported a high rate of major orthopaedic complications (24%), mainly attributable to a high rate of aseptic loosening (20%). Stryker et al. 25 reported on 114 cases of conversion from MoM-THA to CTHA and showed a major orthopaedic complication rate of 18% with a re-revision rate of 7%, primarily attributable to aseptic loosening (14%).
Femoral aseptic loosening, especially in young, active patients, was a common factor for re-revision after conversion in the current study. This has also been found by other authors who assessed UTHA or CTHA revisions. CTHA was developed in an effort to improve the fusion of cement and bone tissue and has become conventional for MoM-THA revision failure.2,5 Short-term or mid-term results of CTHA conversion following MoM-THA failure have revealed extremely low rates of major orthopaedic complications, especially aseptic loosening.8,9 Rahman et al. 6 described 20 patients who developed MoM-THA failure and underwent conversion using CTHA; few patients were found to have aseptic loosening.
This current analysis also revealed that the reason for conversion has a prevailing impact on the outcome of conversion. With modern THA and surgical techniques, conversion due to an indication of MoM wear has low rates of re-revision, regardless of the use of UTHA or CTHA for conversion, whereas conversion due to conventional periprosthetic fracture tends to be associated with a higher rate of re-revision. It is imperative that these facts are understood by orthopaedists and patients prior to conversion.
This study has three main limitations. First, selection bias was unavoidable because of the exclusion of a number of patients. Second, this retrospective observational study was susceptible to errors in the recording of differences in comorbidities and orthopaedic complications, which may have created unaccounted confounding variables and may have resulted in a diminished power to draw convincing conclusions. Attempts were made to allow for more than a few confounding variables; nevertheless, we believe that this analysis is inadequate. Third, we failed to include data on metal ion concentrations and information about high- and low-volume orthopaedists. Despite these limitations, we believe that the margin of error is tolerable in the current setting because of the relatively large sample size.
In conclusion, the mid-term results reported in this study support a growing body of evidence that conversion to CTHA after primary MoM-THA failure is associated with more significant improvements in the modified HHS and lower major orthopaedic complication rates than conversion to UTHA.