
Abstract
Objective
To compare the long-term survivorship and Harris hip scores (HHSs) between cemented total hip arthroplasty (CTHA) and uncemented total hip arthroplasty (UTHA) for treatment of acute femoral neck fractures (FNFs).
Methods
Data of 224 hips (CTHA, n = 112; UTHA, n = 112) that underwent primary surgery in our medical institution from 2005 to 2017 were retrospectively analysed. The primary endpoint was the risk of all-cause revision. The difference in the risk of all-cause revision between the two groups was assessed by Kaplan–Meier survival analysis with a log-rank test and Cox regression analysis.
Results
The mean postoperative follow-up was 10 years (range, 3–13 years). The Kaplan–Meier estimated 10-year implant survival rate was significantly higher in the CTHA than UTHA group (98.1% vs. 96.2%, respectively). The adjusted Cox regression analysis demonstrated a significantly lower risk of revision in the CTHA than UTHA group. At the final follow-up, the mean HHS was significantly higher in the CTHA than UTHA group (85.10 vs. 79.11, respectively).
Conclusion
This retrospective analysis demonstrated that CTHA provided higher survival, lower revision risk, and higher functional outcome scores than UTHA. Further follow-up is necessary to verify whether these advantages of CTHA persist over time.
Introduction
Femoral neck fractures (FNFs) are severe injuries that may be associated with long-term disability.1,2 For displaced FNFs, cemented or uncemented total hip arthroplasty (CTHA or UTHA, respectively) is frequently used. 3 Implant failure secondary to primary THA has become a concern and is eventually addressed using THA revision, contributing to a revision rate as high as 15% to 35%.2,4 Nevertheless, there is a paucity of literature on the long-term survivorship and Harris hip scores (HHSs) following primary CTHA or UTHA in the Asian population. 5
Although previous reports have described implant survival and HHSs after primary CTHA or UTHA, they have either focused on complication rates or primary diagnoses.6,7 Additionally, the reported results of implant survival and HHSs vary widely; this variation is mainly attributable to differences in inclusion and exclusion criteria, sample sizes, and length of follow-up.8,9 Data on long-term implant survival and HHSs are lacking. Furthermore, few reports have described implant survival, and most of these reports have been subject to a short duration of follow-up. 10 Lazarinis et al. 11 reported a 10-year revision rate of approximately 7.5% after CTHA. Almost all recent studies have focused on the application of UTHA and have shown exceptional results, with 5-year survival rates approaching 90% to 100%.6,12 However, these first-rate results have not been verified in other studies; e.g., Swarup et al. 8 reported a 10-year survival rate of 87% after UTHA.
To date, there remains limited evidence for the superiority of CTHA over UTHA in terms of implant survival and the HHS. As the number of THA procedures continues to increase, an understanding these two indexes throughout the postoperative period will be especially valuable. We therefore performed this retrospective study to compare the long-term survivorship and HHSs of CTHA versus UTHA in the treatment of acute FNFs in the Asian population.
Materials and methods
Study population
This study was approved by the Medical Ethics Committee of The Third Affiliated Hospital of Guangzhou Medical University, and the Investigational Ethics Review Board waived the requirement for informed consent. Data of patients who underwent unilateral primary CTHA or UTHA for acute FNFs from January 2005 and August 2017 were collected from our tertiary academic medical centre. The manufacturer details of the stems and cups employed in the THA procedures are shown in Table 1. The main exclusion criteria were inadequate study-related data, secondary CTHA or UTHA, bed-ridden status prior to primary CTHA or UTHA, pathological fracture secondary to malignant disease, incapacity to follow instructions, osteoarthritis or rheumatoid arthritis, active hip infection, tumour, injury severity score of >10, multiple injuries (e.g., pelvic fractures, craniocerebral trauma), severe cognitive impairment, drug or alcohol abuse, and American Society of Anesthesiologists (ASA) score of IV or V.
Manufacturer details of stems and cups employed in THA.
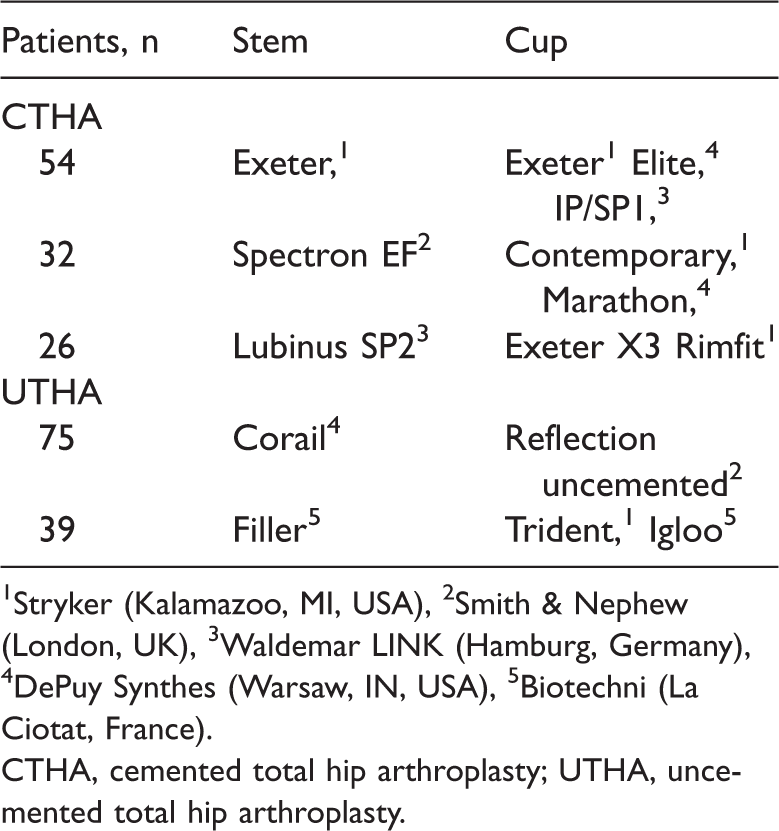
1Stryker (Kalamazoo, MI, USA), 2Smith & Nephew (London, UK), 3Waldemar LINK (Hamburg, Germany), 4DePuy Synthes (Warsaw, IN, USA), 5Biotechni (La Ciotat, France).
CTHA, cemented total hip arthroplasty; UTHA, uncemented total hip arthroplasty.
All surgical procedures were carried out at our medical centre by three high-volume orthopaedists (W.Y., C.Z., and J.Y.), all of whom were experienced with arthroplasties. The indication for surgery was an FNF (OTA/AO classification of 31-B1, 2, or 3). A consistent protocol of antibiotic therapy (1.0 g of cefazolin intravenously twice a day; Baoman Biotechnology, Shanghai, China) was used perioperatively for 3 days. Furthermore, an anticoagulant regimen (4000 aXa IU of enoxaparin sodium [Clexane] intravenously once a day; Aventis, Shanghai, China) was used for each patient without contraindications for 1 month, starting at admission. A similar rehabilitation programme was used for each patient. Early mobilisation was advocated, with weight bearing as tolerated. The follow-up data included the risk of all-cause revision and the HHS. Follow-up occurred 1 year, 2 years, and every 2 years after primary CTHA or UTHA. The primary endpoint was implant survival.
Definitions of variables
Implant survival was calculated from the initiation of primary CTHA or UTHA until the date of final follow-up or revision surgery, whichever occurred first. Signs of cemented or uncemented stem loosening were evaluated by two co-authors in accordance with previous reports,13,14 and the cups were assessed using Charnley zones. 15 Revision was defined as the removal or exchange of any component. 7 Failure was defined as revision of the primary CTHA or UTHA for any reason.
Statistical analysis
The difference in the risk of revision between the groups was assessed by Kaplan–Meier survival analysis with a log-rank test and Cox regression analysis. A Cox proportional hazard model was used to estimate the hazard ratio (HR) and corresponding 95% confidence interval (CI) for survival. The Kaplan–Meier method and Cox analysis were performed with adjustments for age, sex, body mass index (BMI), bone mineral density (BMD), and ASA score. Categorical variables were compared using Pearson’s χ2 test or Fisher’s test, as appropriate. Statistical analyses were performed using SPSS version 24.0 (IBM Corp, Armonk, NY, USA). The level of significance was set at p = 0.05.
Results
Overall survivorship
Based on our criteria, 112 patients (112 hips) with complete data were identified from our medical centre and included in the survival analysis. All patients had a ≥7-year follow-up. The patients comprised 102 (45.1%) men and 124 (54.9%) women with a median age of 68.8 (range, 60–77) years. At the time of analysis, the median follow-up was 10.2 (range, 7–13) years. The median interval from FNF to THA was 8.4 (range, 1–15) days. No statistically significant differences in the baseline characteristics were found between the groups. The baseline data are shown in Table 2.
Patient demographics and outcomes

Data are presented as n or mean ± standard deviation.
aAnalysed using the chi-square test. bAnalysed using an independent-samples t-test. cAnalysed using the Mann–Whitney test.
CTHA, cemented total hip arthroplasty; UTHA, uncemented total hip arthroplasty; HHS, Harris hip score; ASA, American Society of Anesthesiologists; BMI, body mass index; BMD, bone mineral density.
The results of the survival analysis are shown in Figure 1. CTHA provided a significantly better 10-year survival rate (98.1%; 95% CI, 96.1–98.5) than UTHA (96.2%; 95% CI, 95.2–97.3) (p = 0.030). Cox regression demonstrated similar results; patients treated with UTHA had a 1.4-fold higher risk of revision after adjusting for age, sex, BMI, BMD, and ASA score.

Kaplan–Meier survival analysis comparing CTHA with UTHA using the risk of all-cause revision as the primary endpoint. The cumulative survival rate at 10 years after surgery was significantly different between the two groups (p = 0.030). *Hazard ratio was calculated using the Cox proportional hazards model, with adjustment for age, sex, body mass index, bone mineral density, and American Society of Anesthesiologists score as covariates and CTHA/UTHA surgery as the time-dependent factor. CTHA, cemented total hip arthroplasty; UTHA, uncemented total hip arthroplasty.
Functional outcomes
The mean HHS increased from 55.74 ± 10.32 before surgery to 85.10 ± 12.21 at the final follow-up in the CTHA group and from 56.16 ± 11.24 to 79.11 ± 13.19 in the UTHA group. Approximately 72% of the patients who were treated with CTHA or UTHA had a satisfactory HHS at the final follow-up. Table 3 presents the HHS at each follow-up after surgery. The mean HHSs in the CTHA and UTHA groups were 85.12 ± 8.22 and 84.73 ± 6.21 at 1 year after surgery, respectively, with no significant difference. From 2 years after surgery to the final follow-up, CTHA yielded higher HHSs than UTHA (all p < 0.05). Especially at the final follow-up, patients who had undergone CTHA had a significantly higher HHS than patients who had undergone UTHA (85.10 ± 12.21 vs. 78.11 ± 13.19, respectively; p = 0.000).
Long-term functional outcomes.
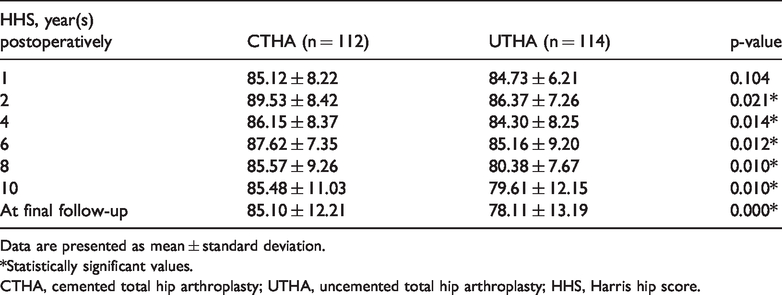
Data are presented as mean ± standard deviation.
*Statistically significant values.
CTHA, cemented total hip arthroplasty; UTHA, uncemented total hip arthroplasty; HHS, Harris hip score.
Discussion
This retrospective review provides evidence that survival is better, the risk of revision is lower, and the HHS is higher after CTHA than after UTHA. To our knowledge, this is the largest study to assess survivorship of patients who have undergone CTHA versus UTHA for treatment of acute FNFs.
A growing but still extremely limited body of literature assessing survivorship between CTHA and UTHA has shown that CTHA provides a survival advantage. 16 In the current analysis, we observed a lower survival rate after UTHA, with 10-year survival approaching 96.2%. Nevertheless, a 10-year survival rate of 57% was reported in a previous study involving 10 patients treated with secondary UTHA. 7 Another study showed a 10-year survival rate of 77% in 20 patients treated with UTHA. 17 The low 10-year survival rate for UTHA was possibly triggered by poor patient survival data and a small sample size. Junnila et al. 18 performed a brand-level comparison of CTHA based on the Nordic Arthroplasty Register Association database and showed that implant survival was higher than the acceptable limit for 10-year survival (95.8%). Laaksonen et al. 19 evaluated 10,113 primary UTHAs and reported that the overall survivorship up to 8 years ranged from 94.4% to 96.25%. However, a recent study showed no significant difference in survival between CTHA and UTHA. 10 This may be partially attributed to the low number of hips (n = 22) in the study. 10 The 10-year survival rate after THA was recently reported in large-sample studies (>100 hips). Davis et al. 20 reported a 10-year survival rate of 95% in a series of 104 CTHA-treated hips. Additionally, a 10-year survival rate of 97% in a series of 112 CTHA-treated hips was reported by Norambuena et al. 21 In two studies from Europe, the 10-year survival rate after CTHA was higher than that after UTHA.22,23 The better hip stability after CTHA than after UTHA is reportedly due to the low stress transfer and good fusion of the cement–bone interface.7,24 The between-component mechanical wear introduced by edge loading is lower in CTHA than in UTHA. 24 Along with our findings, the results reported by these studies seem to confirm that CTHA is the preferred alternative for managing an acute FNF.
The present study showed that CTHA had a lower revision risk than UTHA. The revision risk for CTHA reported in earlier studies tends to vary, ranging from 3.2% to 11.0%.12,24,25 Despite the low revision risk for CTHA in the present study, when previous reports assessing the revision risk for CTHA are regarded as a reference, our revision risk is consistent with previously reported values. 25 Pedersen et al., 4 who used the Nordic Arthroplasty Registry Association database, found that UTHA rather than CTHA in patients younger than 55 years was associated with more short-term revisions because of dislocation, periprosthetic fracture, and infection. Several recent reports have shown a lower revision risk at the midterm follow-up after CTHA than after UTHA.26,27 UTHA appears to be associated with an increased risk of revision following primary THA. 28
The present study has several limitations. First, our study was retrospective, and such a study design tends to lead to errors in evaluating patient characteristics and could be associated with limited power to draw robust conclusions. Second, selection bias was difficult to avoid because of the exclusion of a large number of undesirable cases. Third, the follow-up outcomes are likely to have been influenced by patient-level confounders and the experience of the orthopaedists. Nonetheless, our abidance by arthroplasty guidelines and performance of the procedures in a high-volume environment ensured that we optimised the treatment of patients. Despite the above-mentioned limitations, the error margin seems to be acceptable in the present setting.
In conclusion, the long-term results reported in this study support an increasing body of evidence that CTHA is associated with increased survival benefits, lower revision risk, and higher HHSs than is UTHA. Hence, when proceeding with UTHA in patients with an acute FNF, the patients should be informed of the increased potential for failure, revision, and poor HHS. Furthermore, when interpreting the differences in the survival benefit or revision risk between CTHA and UTHA, strategies to improve implant survival should be directed based on baseline characteristics such as age, sex, BMI, BMD, and ASA score.