
Abstract
Introduction
There is no consensus regarding the superiority between intramedullary nailing and primary arthroplasty in the management of intertrochanteric femoral fractures. This systematic review was performed to investigate and compare the clinical efficacy of intertrochanteric femoral fractures treated with these 2 methods.
Materials and methods
We systematically searched PubMed, Embase, Cochrane, Web of science core collection and ClinicalTrials.gov for randomized controlled trials which compared the clinical outcomes of intertrochanteric fractures treated with either intramedullary nails or primary arthroplasty. Relevant data of the postoperative complications, reoperations, mortality and functional assessment, were pooled and presented graphically.
Results
A total of 6 trials with 427 participants were identified and included in the analyses. The pooled estimates suggested these 2 techniques have comparable risks in terms of overall complications (pooled risk ratio [RR] .80; 95% confidence interval [CI] .43 to 1.43; I2 = 79.94%), the rate of patients with orthopedic complications (RR .71, 95% CI .40 to 1.27; I2 = .00%), reoperations (RR 1.33, 95% CI .48 to 3.71; I2 = .00%), the overall mortality (RR .52; 95%CI .26 to 1.02; I2 = 31.35%) and 1-year mortality (RR .67; 95%CI .38 to 1.19; I2 = .00%). Primary arthroplasty associated with higher HHS at 3 months postoperatively (MD -21.95, 95% CI -28.29 to −15.60; I2 = 70.44%). While the difference was not significant at 6 months (MD 2.32, 95% CI -1.55 to 6.18; I2 = .00%), and even reversed at 12 months postoperatively (MD 13.02, 95% CI 8.14 to 17.90; I2 = 73.42%).
Conclusions
Meta-analytic pooling of current evidences demonstrated that primary arthroplasty is related to a better early functional recovery at the early stage postoperatively, but the long-term result tends to favor to intramedullary nailing. The differences in overall complications, the rate of patients with orthopedic complications, reoperations, overall and 1-year mortality did not reach a significant level.
Keywords
Introduction
Intertrochanteric femoral fractures usually occur in elders, and might lead to pain or even dysfunctions of the lower extremity with a long-term bedridden status. Surgery is considered to be a definitive treatment option as it could allow immediate postoperative weight-bearing and reduce the risks of complications which are the leading causes resulting to disastrous prognosis. 1 There are many methods that can be used for the treatment of intertrochanteric fractures. But the ideal method is still under debate as none of the existing technique could prove its overwhelming superiority.2,3 Internal fixation with an intramedullary nail (IMN) is presently recommended as a typical choice for the majority of intertrochanteric fractures for its excellent performance in mechanical loading and fatigue resistance.2,3 Nevertheless, a satisfactory reduction and a stable fixation could not always be achieved and considerable postoperative complications (eg, Lag screw cut-out, hardware fails) were reported in previous studies, such as Lag breakage of hardware and screw cut-out, which occurs in an incidence of 1.85 to 16.5% and were closely related to tip-apex distance and reduction quality.2,4,5 In response to this, primary arthroplasty was introduced as an alternative option for it shows a lower risk of failure and allows immediately ambulation with full weight-loading regardless of the presence of low bone quality, thus decreasing the complications for bedridden and accelerating functional recovery. 6 Arthroplasty, however, is also associated with a distinct subset of complications, such as dislocation, aseptic loosening and periprosthetic fractures. 2 By reviewing current evidence, it could be found only a limited number of trials directly compared these 2 devices, and different studies demonstrated different results. We therefore presented a meta-analysis on available literature with the aim of evaluating the effectiveness and related harms of these 2 devices in the management of intertrochanteric fractures.
Materials and Methods
This article follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statements. 7 The protocol was registered in the International Prospective Register of Systematic Reviews (registration number: CRD42020195774) and is available online.
Search Strategy
Search Strategy for Pubmed.

Eligibility and Exclusion Criteria
This review considered randomized controlled trials (RCTs) which (1) evaluated adults aged at least 18 years with intertrochanteric fractures; (2) investigated the use of IMN vs primary arthroplasty; (3) reported outcomes of interest; and (4) were published in English. Studies were excluded if they were judged to be at critical risk of bias or there was a major defect such as a high ratio of loss to follow-up (generally ≥20%) and a substantial lack of baseline comparability between groups without adjustment. Studies with patients suffering from previous intertrochanteric fractures, pathological fractures or ambulation dysfunction were ineligible. The titles and abstracts of studies were screened by pairs of independent authors (SZX and YY), and studies that met the prespecified criteria were retrieved for full-text assessment.
Quality Assessment
Two authors (SZX and YY) independently assessed the quality of eligible studies using the Cochrane Risk of Bias tool, in which the risk of bias in domains was rated as “low”, “moderate” and “high”. 9 Discrepancies between them were resolved through discussion or consulting a third reviewer (NW).
Outcome measures and data extraction
Two authors (KFS and FG) worked independently to extract detailed data. An additional author (WN) reviewed the results and resolved conflicts. Basic data included authors, published year, study design, sample size, characteristics of patients and follow-up duration were extracted. The primary outcomes were complications, reoperation rate, mortality and functional outcomes. According to Beaupre et al., the function recovery after hip fracture is time-dependent and the period of significant improvement ranges from 3 months to 12 months. 10 However, we noticed that the follow-up periods unbalanced between the included studies, and different studies use different measurement scales, in which the higher score was not always represent better outcome. Given these facts, only the scores at same time points and using the same measurement tool were pooled and compared.
Statistical Analysis
Data analyses were accomplished and cross-checked by ZJW and FG, and were reviewed by WN. For categorical outcomes, the relative risk (RR) and the associated 95% confident interval (CI) were calculated. Studies with no events in both arms would be excluded from further analyses as they were lacking in indications about the treatment effect and might have potential misdirection on RR. 11 For continuous variables, we calculated the unstandardized mean difference (MD) and the corresponding 95% CI for analyses. If studies didn’t provide the required data which were necessary for meta-analysis, the first choice for this situation was to contact corresponding authors for more detailed information. When there was no response form the authors after 2 times of inquiries, it would be excluded from further analyses. A random-effects model based on the Der Simonian and Laird method was used for data synthesis. Inter-study heterogeneity was determined by using the I2 indicator and was considered to be substantial with I2 more than 50%. Whereafter, we performed a subsequent influence analysis by sequential omission of individual studies to find out the potential outlying study. Publication bias was statistically assessed by the Egger’s test. All statistical analysis was implemented using Stata statistical software (version 16.0, StataCorp LLC). A two-sided P value less than .05 were considered statistically significant.
Result
Characteristics of Included Studies
Our initial literature retrieval identified 1078 articles from database searches and 15 articles from reference lists. After an initial review of titles and abstracts, 30 articles were considered for next full-text assessment. Among them, 21 trials were non-RCTs. One trial did not provide clear description on the study design (RCT or non-RCT).
12
Two trials had problems in their result.13,14 Repeated requests to authors for further detailed information about these trials have been unsuccessful, leaving 6 articles which met the inclusion criteria (Figure 1).15-20 In the 6 trials, 1 was a three-arm study that included an extramedullary fixation group (dynamic hip screw group), which were not considered for statistical synthesis.
18
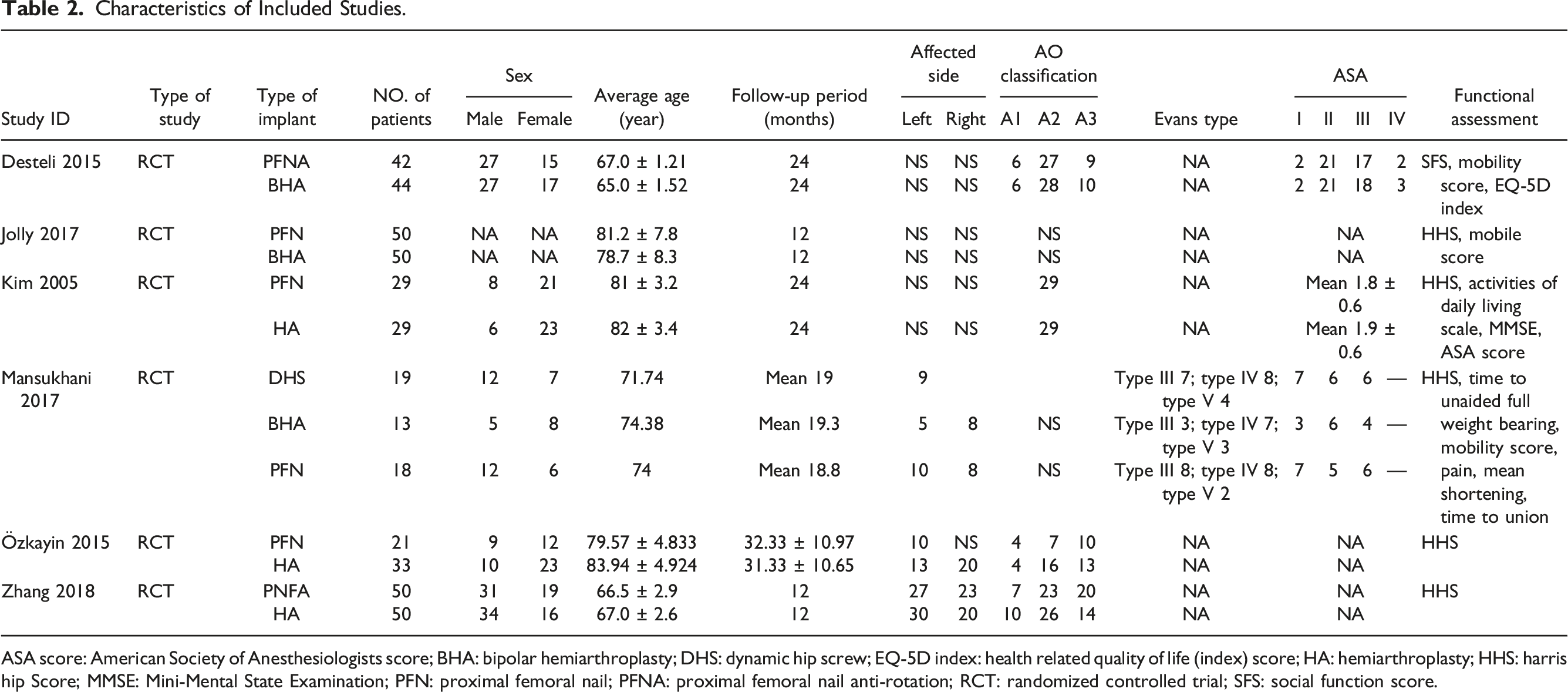
Finally, data from 427 participants, with average age ranging from 65.00 to 83.94 years and mean follow-up period ranging from 12.00 to 32.33 months, were collected for meta-analysis. The characteristics of the eligible studies were summarized in Table 2. Flow diagram of the literature search and selection process. Characteristics of Included Studies. ASA score: American Society of Anesthesiologists score; BHA: bipolar hemiarthroplasty; DHS: dynamic hip screw; EQ-5D index: health related quality of life (index) score; HA: hemiarthroplasty; HHS: harris hip Score; MMSE: Mini-Mental State Examination; PFN: proximal femoral nail; PFNA: proximal femoral nail anti-rotation; RCT: randomized controlled trial; SFS: social function score.
Assessment of Risk of Bias
As shown in Supplemental Material 1, no trials were deemed low risk of bias in all domains according to the Cochrane Risk of Bias tool. The unblinding of participants and personnel, and unblinding of outcome assessors were the most common deficiencies in trials. Random sequence was generated in all 6 studies, but 3 of them didn’t give a clear description on the concealment of allocation,15-17 and 1 study just referred to random assignments without providing the details of random assignments. 20
Due to the limited number of included studies, statistical assessment for publication bias was not routinely performed in all items except for the comparison of overall complications, and no obvious publication bias was detected based on the result of the Egger’s test (P = .4278; n = 5) in that item.
Effects of Interventions
Postoperative complications
Postoperative complications were reported in all the 6 articles. One study just gave a brief description that no dislocation or screw cut-out was observed in both groups.
15
The pooled analysis based on the other 5 studies showed no statistically significant difference between the 2 groups in terms of the incidence of overall complications (RR .80; 95% CI .43 to 1.43; I2 = 79.94%) (Figure 2a). Considerable heterogeneity was noted in this data synthesis. Given the fact that there was substantial variability between studies in monitoring and reporting postoperative complications and 1 patient might have more than 1 complication, and there would be a strong link between these complications (eg, nonunion and breakage of internal fixation/protrusion, prosthetic loosening and periprosthetic fracture/joint dislocation), we conducted a subsequent analysis on the rate of patients with orthopedic complications, which are directly related to the implants and mainly include screw perforation, backing out or cut-out of screws, failure of fixation, nonunion, avascular Necrosis, dislocation, prosthesis loosening and periprosthetic fracture. Three studies provided the detail information about the numbers of the affected patient.16-18 Pooling the estimates showed no statistical difference between the 2 groups (RR .71; 95% CI .40 to 1.27; I2 = .00%) (Figure 2b). Pooled analysis of the rate of overall postoperative complications and patients (a) with orthopedic complications (b).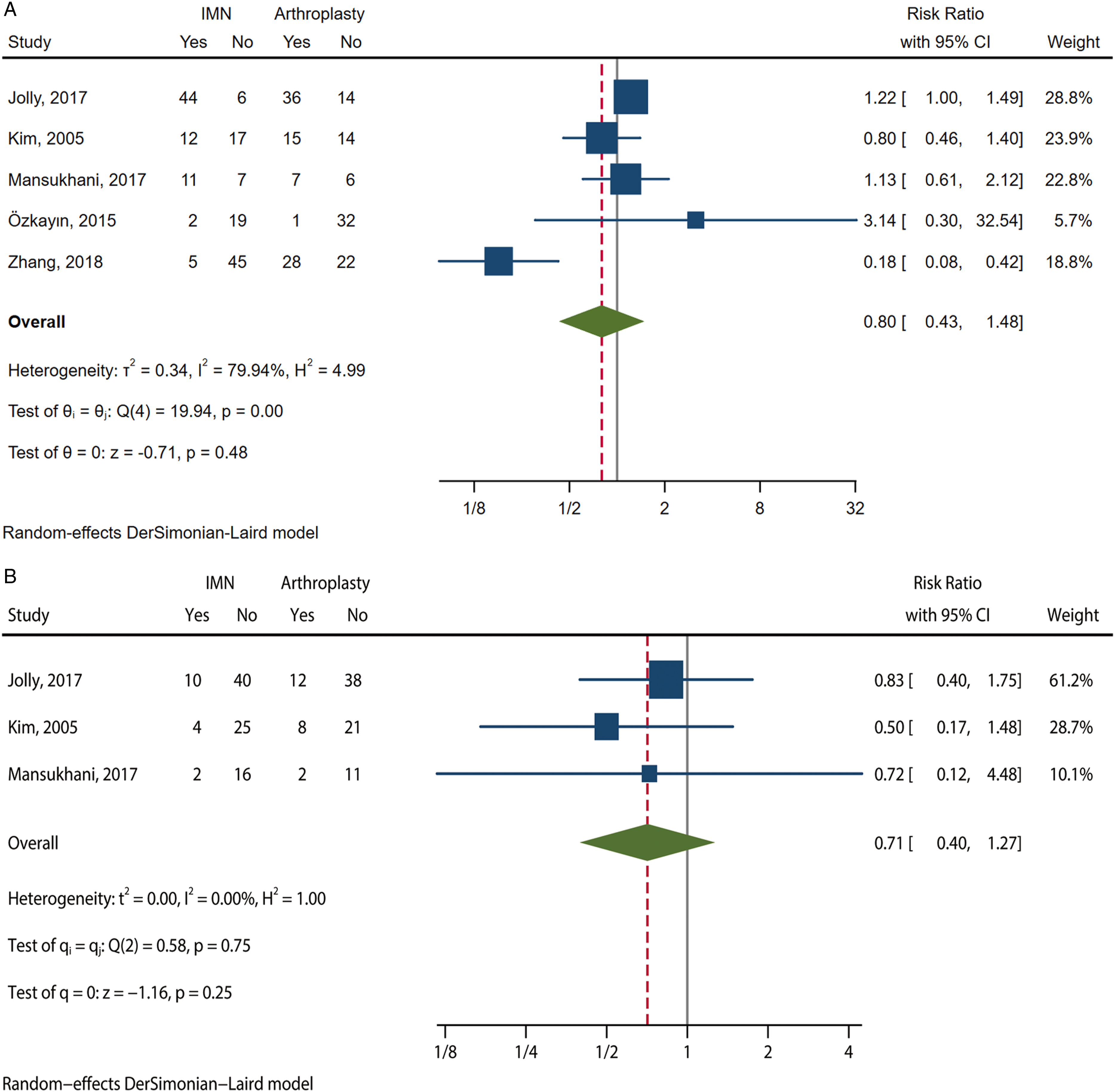
Reoperation rate
The rate of reoperations was reported in 3 articles.17-19 No significant difference was detected in the pooled estimate (RR 1.33, 95% CI .48 to 3.71; I2 = .00%) (Figure 3a). However, the result seems to be unpersuasive. In Jolly 2017, 1 patient developed avascular necrosis and 1 patient developed cutting-out of the screw, but the authors didn’t specify whether the reoperations were performed or not.
16
In Kim 2005, 2 patients had cutting-out of the hip screw, but they refused to accept another surgery.
17
When we took these patients in consideration and re-analyzed the data, the result did not change dramatically (RR 1.82, 95% CI .71 to 4.67). There was also no significant heterogeneity (I2 = .00%) (Figure 3b). Pooled analysis of the rate of reoperations actually incurred (a) and that should theoretically happen (b).
Functional outcomes
Functional evaluations were reported in all 6 trials, but measurement scales used in these studies were many and varied, which included Harris hip score (HHS),
21
mobile score of Parker and Palmer,
22
American Society of Anesthesiologists (ASA) score,
23
social function score (SFS) value,
24
health related quality of life (EQ-5D index) score
25
and Mini-Mental State Examination (MMSE).
26
The details of these findings were listed in Supplemental Material 2. HHS was the most commonly used tool and data form 3 studies were extracted and synthesized.16,19,20 The difference was statistically significant in favor of arthroplasty group at 3 months postoperatively (MD -21.95, 95% CI -28.29 to −15.60; I2 = 70.44%) and was not significant at 6 months (MD 2.32, 95% CI -1.55 to 6.18; I2 = .00%). Whereas the difference reversed at 12 months postoperatively, ai which time a higher HHS was found in the IMN group (MD 13.02, 95% CI 8.14 to 17.90; I2 = 73.42%) (Figure 4). Also, the pooled estimate of mobility score of Parker and Palmer at 12 months postoperatively demonstrated a better result in the IMN groups (MD .14, 95% CI .09 to .19; I2 = .00%) (Figure 4d). Substantial heterogeneity was detected in the pool results of HHS at the 3 and 12 months postoperatively. But the result in each study was consistent with pooled results. No obvious change was detected in the pooled results when we omitted the included study one by one. Pooled analysis of HHS at 3rd month postoperatively (a), 6th month postoperatively (b), 12th month postoperatively (c) and pooled results of mobility score of Parker and Palmer at 12 months postoperatively (d).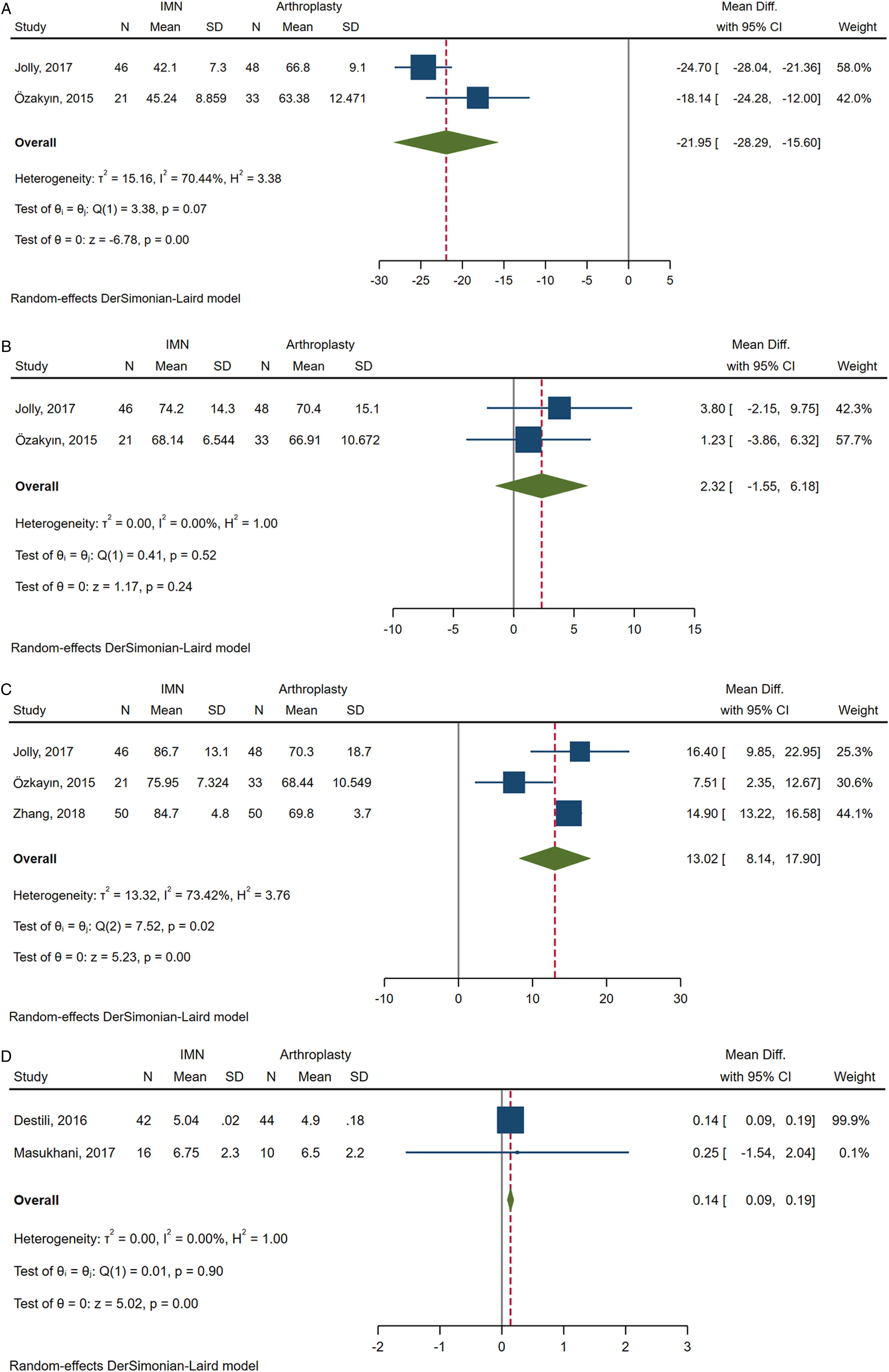
Mortality
Mortality was reported in 4 trials.15-18 Except for 1 trial which just mentioned the overall mortality of the total participants (6/92), 15 the other 3 trials were included in the analysis.
Regardless of the follow-up period, the overall mortality was not statistically significant between the 2 groups (RR .52; 95%CI .26 to 1.02), with moderate heterogeneity (I2 = 31.35%) (Figure 5a). Given the un-balance follow-up period between studies, we conducted a subsequent analysis on the 1-year mortality. The pooled effect size was still not statistically significant (RR .67; 95%CI .38 to 1.19) and there was no significant heterogeneity (I2 = 0%) (Figure 5b). Pooled analysis of over-all mortality (a) and 1-year mortality (b).
Sensitive analysis
We performed sensitivity analyses restricted to trials comparing the PFN and cement arthroplasty, which are the most commonly used implants in these trials. Based on available data, sensitive analyses could be just performed on part of the parameters. Except for the incidence of overall complications, there was no dramatic changing in other parameters (see Supplemental Material 3). Besides, the analyses on the rate of patients with orthopedic complications and 1 year mortality could also be deemed as the sensitive analysis for the overall complications and mortality.
Discussion
This is not the first systematic review on this topic. As the limited number of available evidence, RCTs and non-RCTs were synthesized together in previous system reviews and conclusions were inconsistent between them.27-29 The present study, to some extent, could be deemed as a complement and an update to existing reviews. Compared with previous reviews, it includes the following new information: (1) to reduce the heterogeneity caused by study design, only RCTs were considered in this review; (2) to eliminate the nonuniformity in the definitions of postoperative complications, a subsequent analysis about the rate of patients with orthopedic complications was performed; (3) concerning the time-dependent characteristics of functional recovery, functional scores at the same time point were compared and the clinical course of functional recovery was specified; (4) given the unbalance follow-up period between studies, both the overall mortality and 1-year mortality were compared.
Currently, there is no established indication of the using of primary arthroplasty in the treatment of intertrochanteric fractures. It is generally agreed that intramedullary fixation is the mainstay of treatment options for the majority of intertrochanteric fractures, and primary arthroplasty is used as a salvage protocol for the failure of fixation, or applied to patients with severe osteoarthritis, poor bone quality or urgent needing for immediate ambulation. For individual patients, surgeon’s preferences might have a significant impact on the choice of surgical strategy in clinical practice. The reported benefits of primary arthroplasty are mainly known for the lower risk of failure and immediately free ambulation regardless of bone quality, thus reducing the complication and reoperation rate, accelerating functional recovery.2,6,26 However, primary arthroplasty is still a technical challenge for surgeons, and there is no special-designed prosthesis for intertrochanteric fractures. While with upgrading and modifying, the newer designed intramedullary implants, favoring minimally invasive insertion and possessing more biomechanics advantages, have high mechanical resistance to failure and allow early mobility even for patients with advanced age and serious osteoporosis. 30 Multiple trials demonstrated that the prescription regarding bedridden time after internal fixation is not indispensable as before.15,17-19,31 In 4 of the 6 trials included in this review, patients underwent IMNs were allowed to get out of bed with or without crutches within 4 days after surgery.15,17-19 The other 2 trials didn’t provide detailed information on that issue.16,20 In the present review, when we pooled the data from individual studies together, the results suggested there were no significant differences with regard to the risks of complications, as well as the rate of reoperations. These results are in conflict with a previous meta-analysis by Nie et al, 28 but consistent with Tu et al. 29 The different criteria of eligible studies and non-identical definitions of compilations might be possible reasons for the discrepancy.
A higher HHS favoring to the intramedullary fixation group at the last follow-up was observed in 2 previous meta-analyses conducted by Kumar et al. and Nie et al.27,28 While a comparable result was reported in the meta-analysis by Tu et al. 29 They did not, however, specify and analyze the course of functional recovery at different time, which might be the reason for the inconsistent conclusions in their studies. Our study attempted to address this issue. We compared the functional scores according to the time point instead of that at the last follow-up. Interestingly, a rapid functional recovery in patients experienced arthroplasty was noted at the early postoperative stage (mostly within 3 months). While patients with IMNs tended to display a subsequent higher increasing rate of functional rehabilitation, and the differences were comparable or even reversed from 6 to 12 months postoperatively.
As mentioned above, there might be no significant difference with respect to bedridden time. But there were still differences in effective weight-bearing between patients underwent intramedullary fixation or arthroplasty.16,20 Commonly, patients who underwent arthroplasty could bear full load at the early postoperative stage, whereas patients with IMNs often need a period of partial weight-bearing training, especially when an adequate reduction and a stable fixation were not achieved.17-19 Early postoperative weight-bearing is supposed to be a major contributing factor to the superior functional outcome, while non-weight-bearing status or weight-bearing restrictions will result in the accelerated loss of muscle in elder patients, which in turns affects the ability of motion of patients at early the stage. 32 Shortly afterwards, when patients with IMNs could move without restriction, they tended to display a higher increasing rate of functional rehabilitation, and might obtain a better result in the middle and long term. Many authors owe that to the minimally invasive procedures and the preservation of anatomical structures that could conduce to less physiological and functional disturbances on patients.16,33
The pooled effect estimate showed the mortality rate was slight lower in the IMN group, but without statistical significance. Many authors believed that the treatment method could not be regarded as an independent risk factor as multiple other factors might have statistical influences on postoperative mortality. 34 Mariconda et al. carried out multivariate analyses and identified that the general complications and pre-operative comorbidities of the patients had a strong correlation with the postoperative mortality. 35 While, others insisted that arthroplasty might worsen the already grave situations of patients and result in fatalities, especially for patients with advanced age (>80 years) or high ASA scores.33,36,37 Ucpunar et al. compared 64 patients who were treated using PFN with 76 patients who underwent hemiarthroplasty, and found the latter demonstrated poor health status with increased postoperative cumulative illness rating scale (CIRS) score at the 3-month follow-up. 37 These findings suggested that surgeons should take the patient-specific factors, especially the general healthy condition and the physiological age, into consideration before making a therapeutic decision to prevent causing more detriments than benefits.
The effects of surgical duration and intraoperative blood loss were not synthesized in this review. Surgical duration with statistical difference favoring the IMN group was observed in 4 trials,16,17,19,20 whilst a comparable result between the 2 groups was showed in 1 trial, 18 and an unfavorable outcome associated with the IMN group was detected in 1 trial. 15 Four trials reported intraoperative blood loss and found a statistically significant difference favoring the IMN group. Nonetheless, as tabulated in Supplemental Material 4, the mean value and range of surgical duration and blood loss differed greatly between each study. We notice that the definition of surgical duration (with or without the time spending on traction bed) was not unified between studies, and the hidden blood loss, which might exceed the observed blood loss during surgery and plays a more important role in total blood loss, was not calculated in these studies. 38 That might reduce the convincement of the assessment on surgical duration and blood loss. Overall, this group of heterogenous studies was too limited to draw valid conclusions in terms of the surgical duration and intraoperative blood loss.
Limitations
There is currently still a paucity of high-level evidence on this topic and only 6 RCTs with small sample size were identified in this review. The number of trials in each meta-analysis were small, thus statistical assessments on publication bias or small study effects (eg, contour-enhanced funnel plots, Egger regression test) were not routinely implemented. Owing to the feature of surgical treatment, rigorous double-blinding in real clinical settings was difficult to be implemented. These limitations highlight the need for additional rigorous studies, RCTs or otherwise, to provide further investigations into this issue.
The types of implants and the differences in patients’ age might influence the clinical outcomes. We have pooled the treatment effects based on available data to investigate whether there were differences caused by cemented or uncemented arthroplasty (see Supplemental Material 5). But the limited number of included studies might reduce the convincing and the universality of the results. However, we noticed the analyses on rate of patients with orthopedic complications, reoperation and mortality were already based on the studies with patients in narrow range of mean age (from 78.7 years to 83.94 years) (Table 1, Figure 2 to 5). To a certain extent, that might reduce the influencing effects and between-study heterogeneity caused by the difference of age. While, the comparisons of functional recovery were based on studies with patients in an age gap of nearly 17 years (mean age range from 66.5 years to 83.94 years), which might be a possible reason for the substantial heterogeneity observed in the analyses of HHS.
Conclusions
Evidences based on current studies reveal that there are some differences in the changing trend in functional recovery. Primary arthroplasty is associated with better functional rehabilitation at within 3 months postoperatively, but the long-term outcome tends to favor IMNs. Beyond that, there is no significant difference in postoperative complications, reoperation, the overall and 1-year mortality.
Supplemental Material
Supplemental Material - Intramedullary Nail or Primary Arthroplasty? A System Review and Meta-Analysis on the Prognosis of Intertrochanteric Femoral Fractures Based on Randomized Controlled Trials
Supplemental Material for Intramedullary Nail or Primary Arthroplasty? A System Review and Meta-Analysis on the Prognosis of Intertrochanteric Femoral Fractures Based on Randomized Controlled Trials by Zhaojun Wang, Fei Gu, Shizhuang Xu, Yang Yue, Kefu Sun and Wei Nie in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.